 Time to Open6 monthsSetup window
Time to Open6 monthsSetup windowHow to Open a Concussion Assessment Clinic in 4-9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open6 monthsSetup window  Launch Sequence7 stagesCompliance first
Launch Sequence7 stagesCompliance first Key BottleneckStaffing gapPayer and referrals
Key BottleneckStaffing gapPayer and referrals First Revenue StepEval bookingsReferral intake
First Revenue StepEval bookingsReferral intake


Key Takeaways
- Licensing and ownership rules can delay launch.
- Protocols must be ready before adding services.
- Payer-ready staff drive capacity and clean billing.
- Referral outreach should start before opening day.
Time to Open6 monthsSetup windowLaunch Sequence7 stagesCompliance firstKey BottleneckStaffing gapPayer and referralsFirst Revenue StepEval bookingsReferral intakeLaunch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9
Compliance
- Scope service lines
- Review state rules
- Prepare filing packet
- Submit applications
- Confirm compliance signoff
Facility buildout
- Finalize floor plan
- Start leasehold work
- Install treatment rooms
- Complete safety checks
- Receive occupancy approval
Equipment and IT
- Select diagnostic vendors
- Order key equipment
- Set up EHR
- Install security network
- Test rehab tools
Staffing and training
- Define headcount plan
- Hire medical director
- Recruit clinicians
- Complete credentialing
- Train front desk
Payer setup
- Map payer list
- Build fee schedule
- Submit credentialing files
- Confirm billing workflow
- Test claim entry
Referral launch
- Draft referral script
- Meet referral sources
- Build waitlist funnel
- Run soft opening
- Go live review
Why test launch timing before you sign?
Before you sign, open the Concussion Assessment and Treatment Clinic Financial Model Template to test launch timing, ramp, and runway.
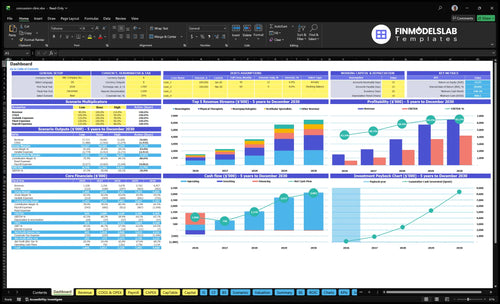
What the model should show
- Month 1-60 dashboard tabs
- Staffing schedule and utilization
- Revenue by clinician type
- 45/35/8/6 cost rates
- Year 1 revenue: $127,325
What launch mistakes create the biggest readiness risks?
The biggest readiness risk is opening the Concussion Assessment and Treatment Clinic before referral pathways, payer credentialing, and billing are live, because patients can show up before cash does. A launch gate review should confirm legal setup, clinician coverage, EHR, equipment, patient flow, referral commitments, and Month 1 capacity assumptions. If onboarding takes 14+ days or billing fails early, collections lag even when demand exists.
Biggest launch risks
- No steady referral flow
- Slow payer credentialing
- Clinicians out of protocol
- Unclear care scope
Launch gate checks
- Legal setup complete
- Billing workflow tested
- EHR ready for documentation
- Equipment and patient flow set
What are the requirements to open a concussion clinic?
To open a Concussion Assessment and Treatment Clinic, you need state-law clearance, credentialed clinicians, malpractice coverage, HIPAA-compliant systems, payer setup, and a billing model tied to your services; use How To Launch Concussion Assessment And Treatment Clinic Business? as the practical launch path. Demand is real: the Centers for Disease Control and Prevention reported 214,110 TBI-related hospitalizations in 2020 and 69,473 TBI-related deaths in 2021 in the US.
Legal and clinical
- Confirm state medical practice ownership rules
- Name a supervising clinician or medical director
- Verify clinician credentials and service scope
- Carry malpractice coverage before patient care
Operations and billing
- Use HIPAA-compliant patient records and consent forms
- Set EHR, claims, and documentation workflows
- Define evaluation, therapy, and rehab services
- Choose cash-pay, insurance, or mixed billing
How long does it take to open a concussion clinic?
If you’re opening a Concussion Assessment and Treatment Clinic, the practical range is 4–9 months. Faster launches usually use limited evaluation services, leased medical space, fewer payers, and referral-based rehab; slower launches add buildout, broader payer contracting, multidisciplinary hiring, therapy rooms, and diagnostic tools.
Faster launch path
- Use leased medical space
- Start with limited evaluations
- Contract fewer payers first
- Build rehab by referral
Main delay drivers
- Lease negotiation slows opening
- Medical buildout adds weeks
- Payer credentialing takes time
- State rules can shift timing
Confirm what must be ready before the clinic sees patients
Launch readiness checklist
Use this go-live approval checklist to confirm the concussion clinic is ready before opening.
Licensing
- Entity and scope approvedCritical
The clinic needs a clear legal scope before contracts and hiring move ahead.
- State practice rules checkedCritical
Licensure and supervision rules must fit the services you plan to offer.
- Malpractice policy boundCritical
Coverage should be live before any patient exam or treatment.
Clinical
- Medical director assignedCritical
A named clinical lead keeps supervision and signoff clear.
- Care protocols approvedHigh
Standard steps reduce variation in diagnosis and treatment.
- Consent forms finalizedHigh
Patients must understand risks, limits, and follow-up expectations.
Facility
- Rooms and flow readyHigh
Exam and therapy spaces must support safe patient movement.
- Diagnostic tools testedCritical
Testing must work before you promise same-day assessment.
- Therapy equipment installedHigh
PT and vestibular gear must be usable on day one.
Systems
- EHR templates builtCritical
Templates should capture symptoms, exams, and treatment plans.
- Patient portal liveHigh
Patients need a working way to complete intake and message staff.
- HIPAA controls verifiedCritical
Role access and privacy settings must protect health data.
Staffing
- Licensed clinicians scheduledCritical
Launch needs licensed coverage for each promised service line.
- Referral intake routedHigh
Referrals must land in one clear path or first visits will slip.
- Opening-week coverage setHigh
You need backup coverage for no-shows, PTO, and intake spikes.
- Intake team trainedHigh
Front desk and care coordinators must handle scheduling and handoffs.
Revenue
- Payer files submittedCritical
Unsigned or missing payer files delay claims and cash.
- Billing workflow testedCritical
Clean claims and collection steps must work before first volume.
- Cash runway confirmedCritical
Opening cash must cover setup spend and early operating gaps.
- Go-live signoff completeCritical
Signoff should confirm licensed staff, workflow, and first-month revenue readiness.
Which launch drivers decide opening-day readiness?
1Compliance
4-9 moVerified ownership, licensing, and HIPAA controls reduce opening delays and payer onboarding friction.
2Care Model
Day-one pathA written concussion pathway keeps intake, testing, follow-up, and escalation consistent from launch.
3Staffing
Y1 mixYear 1 staffing of 2 neurologists, 1 neuropsychologist, 2 physical therapists, 1 vestibular specialist, and 1 occupational therapist sets capacity.
4Equipment
Live setupLive EHR, testing tools, and therapy rooms must work together or opening slips.
5Billing
22% varPayer setup, claim checks, and collection rules speed cash and keep denial cleanup from slowing visits.
6Referrals
$127K/moReferral outreach before opening drives first visits and supports about $127K in modeled monthly revenue.
Compliance, Licensing, And Ownership
Licensing and ownership gate
State medical practice rules can block opening if they control who owns, supervises, and bills for care. For a concussion clinic, day-one readiness means the ownership structure is verified, licensed clinicians are in place, malpractice coverage is active, and consent forms, HIPAA policies, secure records, and documented scope of care are finished before the first visit.
Here’s the quick math: one missing license, one weak payer file, or one unsigned privacy workflow can slow scheduling and claims from day one. The safest move is a legal review before lease finalization, then align payer files, incident reporting, and staff training before patient booking starts, so opening delays stay low and payer onboarding is cleaner.
Verify each state, not just one
Do the compliance work before opening week so the clinic can see patients without a launch gap. Check ownership and supervision rules in every state tied to the practice, then lock down records, privacy, and consent so front desk and clinical staff use the same process on day one.
- Confirm ownership and supervision rules.
- Verify every clinician license.
- Test HIPAA and secure records.
- Approve consent and incident steps.
- Align payer files before visits.
1
Care Model And Treatment Protocols
Care Model And Treatment Protocols
For a concussion clinic, the service menu decides staffing, rooms, scheduling, and billing. If the day-one pathway is not written, you cannot safely open because staff will improvise on intake, triage, and follow-up. A clean launch needs one approved path for evaluation, screening, balance testing, symptom tracking, return-to-play, return-to-work, follow-up, and referral escalation.
Build the pathway before the schedule
Start with intake forms, triage rules, visit templates, and outcome measures. Then test handoffs from first visit to follow-up so each clinician knows when to document, when to refer, and when to stop adding services. If protocols lag behind booking, first-day visits slow down, notes get inconsistent, and billing gets messy.
Run mock visits and confirm room setup, testing access, and note templates match the protocol before the first patient is booked. One clean workflow beats three half-built ones.
2
Qualified Clinical Staffing
Qualified Clinician Mix
You can't open on time if the right clinicians aren't signed, credentialed, and trained. In this clinic, staffing is not just payroll; it's the capacity, billing, and care-quality gate. If a clinician lacks payer-ready credentials, you may see patients but still wait to bill, which strains cash and can delay day-one launch.
The Year 1 model assumes 2 neurologists, 1 neuropsychologist, 2 physical therapists, 1 vestibular specialist, and 1 occupational therapist. At the stated monthly treatment assumptions, that is 850 treatments/month before utilization. One vacancy can remove 80 to 140 visits per month, so the mix has to be locked before opening.
Credential First, Hire Second
Start with signed coverage, payer credentialing, schedule templates, and protocol training. Here’s the quick math: 2 neurologists at 120 each = 240, 1 neuropsychologist = 80, 2 physical therapists = 280, 1 vestibular specialist = 120, and 1 occupational therapist = 130. That totals 850 monthly treatments.
- Verify license status first.
- Confirm payer enrollment dates.
- Match templates to each role.
- Train on one care protocol.
Do not hire to fill seats first and sort credentials later. Verify license status, scope of practice, supervision rules, and billing enrollment before you publish the schedule. If onboarding slips, patient slots open late, the first-week plan shrinks, and the clinic can miss revenue even with rooms ready.
3
Facility, Equipment, And Patient Flow
Room and Flow Readiness
A concussion clinic cannot open on time if the exam rooms, therapy space, and testing workflow are not linked. Day-one care depends on live EHR, outcome tools, neurocognitive testing access, balance or vestibular setup, and private documentation areas, plus a check-in and check-out flow that works without chaos.
This matters because the Year 1 model assumes capacity from 2 neurologists, 1 neuropsychologist, 2 physical therapists, 1 vestibular specialist, and 1 occupational therapist. If room mapping or software access slips, those visits stall, patient handoffs break, and first revenue starts late. The bottleneck is treating equipment like a shopping list instead of a dependency chain.
Set the launch sequence, not just the purchase list
Start with the dependency chain: room map, software access, data security, then equipment procurement. Confirm where patients check in, where testing happens, where therapy happens, and where notes are private before you order anything that needs space or network access.
Run mock visits before opening. Test intake, room turnover, documentation, and check-out with real staff tasks, not just a checklist. If the EHR, testing tools, or patient movement fail in rehearsal, fix them before launch so the clinic can serve patients from day one without scrambling.
4
Payer, Billing, And Revenue Cycle
Billing and Cash Flow Readiness
For a concussion clinic, revenue starts only after credentialing, clean documentation, and claims setup are live. If you book visits before payers are ready, you can treat patients but still wait on cash, which strains opening payroll and vendor bills.
One clean rule: no open schedule until the claim path is tested end to end. That means payer applications tracked, prior auth workflow defined, and CPT documentation expectations reviewed by billing staff.
Test the claim path before day one
Set the cash-pay policy, assign denial follow-up, and run at least one mock claim scrub before opening. In this model, 6% goes to medical billing and collection fees, and 35% to diagnostic software licensing, so weak billing setup hits early margin fast.
Here’s the quick math: if claims are rejected or delayed, collections slow even when the clinic is busy. That can push back cash conversion and make first-month staffing and software costs harder to cover.
- Track payer applications daily.
- Document prior auth steps.
- Test claim scrub rules.
- Assign denial follow-up.
- Review CPT notes with billing.
5
Referral Network And First-Patient Pipeline
First-Patient Referral Pipeline
For a concussion clinic, first revenue starts with scheduled evaluations, not with a finished buildout. If outreach starts in opening week, you can have licensed staff and empty slots, which slows cash in and weakens day-one patient flow.
The readiness signal is a pre-opening list of physicians, urgent care centers, emergency department discharge coordinators, neurologists, schools, sports clubs, employers, local search pages, and community education events. That pipeline has to match intake, referral, and follow-up so leads turn into booked visits.
Pre-Open the Referral Engine
Start outreach before opening, and make sure every source gets the same referral form, intake script, and follow-up cadence. Use compliant education materials so staff can send the same message without slowing legal review or payer setup.
- Assign each referral source an owner.
- Track booked evaluations by source.
- Test response times before launch.
- Set follow-up reminders in advance.
- Budget 8% for marketing and referral development.
The cash risk is simple: no pipeline means no first visits, even if the clinic is open. Build the outreach calendar now so day-one schedules already have patients on them.
6
Related Products
- Concussion Assessment and Treatment Clinic Porter's Five Forces Analysis
- Concussion Assessment and Treatment Clinic BCG Matrix
- Concussion Assessment and Treatment Clinic Business Model Canvas
- What Are The 5 Core KPI Metrics For Concussion Assessment And Treatment Clinic?
- Concussion Assessment And Treatment Clinic Business Plan Template in Pre-Written Word
- How Increase Profitability Concussion Assessment And Treatment Clinic?
- What Are Operating Costs For Concussion Assessment And Treatment Clinic?
- Concussion Clinic Startup Costs: Plan Around $80K+ in Known CAPEX
- Concussion Clinic Financial Model Template in Excel
- How Much Can a Concussion Clinic Owner Make? $240k+ Planning View
- How To Write A Business Plan To Launch A Concussion Assessment And Treatment Clinic?
- Concussion Assessment and Treatment Clinic Marketing Mix
- Concussion Assessment and Treatment Clinic Marketing Plan
- Concussion Assessment and Treatment Clinic Business Proposal
- Concussion Assessment and Treatment Clinic PESTEL Analysis
- Concussion Assessment And Treatment Clinic Pitch Deck Example Editable PPTX
- Concussion Assessment and Treatment Clinic Business SWOT Analysis
- Concussion Assessment and Treatment Clinic Value Proposition Canvas
Frequently Asked Questions
Start by defining the clinical scope, then verify state medical practice rules, ownership structure, clinician credentials, malpractice coverage, EHR, billing, and referral workflows A practical launch plan runs 4-9 months The Year 1 planning model uses 7 clinical staff across neurology, neuropsychology, physical therapy, vestibular care, and occupational therapy