 Owner incomeUp to $726k
Owner incomeUp to $726kHow Much Can a Concussion Clinic Owner Make? $240k+ Planning View

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner incomeUp to $726k  Net margin42.5%
Net margin42.5% Revenue for target pay$1.71M
Revenue for target pay$1.71M Business difficultyHard
Business difficultyHard


A US concussion assessment and treatment clinic can show $240,000 in annual owner salary if the owner fills the Medical Director role, plus operating profit if cash is distributed This first-year model uses $127,325 monthly collections, 531 monthly visits, and a 318% operating margin, before taxes, debt service, reserves, and any clinician payroll not listed in the wage assumptions
Owner incomeUp to $726kNet margin42.5%Revenue for target pay$1.71MBusiness difficultyHardCan this clinic support your target owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate only, not guaranteed salary, tax advice, or owner distribution advice.
Want to test the full concussion clinic model?
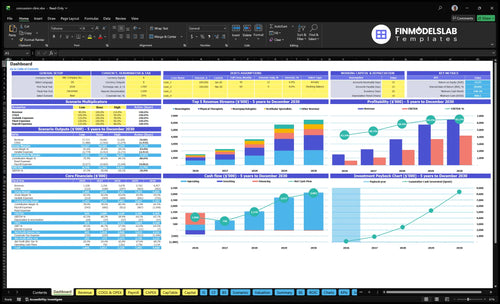
This dashboard in the Concussion Assessment and Treatment Clinic Financial Model Template shows revenue, visit volume, capacity, EBITDA, reserves, and owner pay assumptions. Open the model.
Model highlights
- $127,325 monthly collections
- 531 visits first year
- $19,650 fixed overhead
- $470,000 wages cost
- $486,000 operating profit
Can a concussion clinic owner make a living?
Yes, a How To Launch Concussion Assessment And Treatment Clinic Business? owner can make a living under this model if they also serve as Medical Director: the salary line is $240,000 per year before taxes. The model also shows about $486,000 in first-year operating profit before debt, reserves, taxes, and any unlisted clinician payroll.
Owner pay case
- $240,000 Medical Director salary
- $486,000 operating profit before major deductions
- 531 collected visits per month
- 65% to 70% early core-service capacity
Key limits
- Keep referrals steady
- Collect cleanly and on time
- Fund debt, reserves, and taxes
- Pay another clinician if unlicensed
What affects concussion clinic profit margin most?
The biggest margin swing in a Concussion Assessment and Treatment Clinic is provider pay and collections quality, not the billed charge on the claim. If you’re mapping the setup in How To Launch Concussion Assessment And Treatment Clinic Business?, start with $470,000 in listed wages, 22% first-year combined COGS and variable costs, and $19,650 a month in fixed overhead. High charges still miss the point if denials rise, reimbursement falls, or payroll sits outside the model.
Main margin drivers
- Provider compensation hits hardest.
- Payer mix changes cash collected.
- Billing fees take 6% of collections.
- Marketing takes 8% in year one.
Fixed cost pressure
- COGS is 8% of collections.
- Fixed overhead runs $19,650 monthly.
- Rent, equipment, EHR add steady drag.
- Malpractice and admin labor also matter.
How much revenue is needed for concussion clinic owner pay?
If the Concussion Assessment and Treatment Clinic needs to cover payroll and fixed overhead, it needs about 315 visits per month at the first-year average collection of $23,978 and a 78% contribution margin. That gets the clinic to break-even before owner distributions. The $240,000 Medical Director salary is already inside the $470,000 wage base, but extra owner pay still depends on operating profit, cash reserves, and payer collections. Payer delays can make a profitable month feel cash-tight.
Break-even math
- 315 visits covers fixed costs
- Average collection is $23,978
- Contribution margin is 78%
- Break-even comes first
Owner pay
- $240,000 is in the wage base
- Wage base totals $470,000
- Extra draws need operating profit
- Payer delays can squeeze cash
Want the six main concussion clinic income drivers?
1
531Patient Volume
More first-year visits spread rent, wages, and software over more billable work, so owner take-home rises fast.
2
$23.98KPayer Mix
Better reimbursement and payer mix lift average cash per visit, so the same caseload produces more margin.
3
85%-90%Provider Utilization
Higher clinician use turns paid time into billable visits and keeps salary cost from dragging down profit.
4
78%Service Mix
A stronger mix of higher-priced neuro visits and therapy services supports the 78% contribution margin.
5
315Fixed Overhead
With about $19.65K in monthly fixed overhead, the clinic needs roughly 315 visits before profit starts to build.
6
$127.3K/moCollections
At about $127.3K in monthly collections, cleaner billing and follow-up protect cash and owner pay from claim delays.
Concussion Assessment and Treatment Clinic Core Six Income Drivers
Qualified Patient Volume And Referral Flow
Qualified Patient Volume
This driver is the count of qualified patient visits that actually get completed, not website leads. The first-year model assumes 531 monthly visits across neurology, neuropsychology, physical therapy, vestibular therapy, and occupational therapy. More visits spread fixed clinic costs and raise owner distributions. If flow stays strong, the clinic stays above the 315-visit break-even point; if it slips, profit falls fast.
Referral flow usually comes from primary care, emergency departments, schools, athletic programs, employers, and attorneys. The key inputs are collected visits by source and the conversion from referral to booked, completed care. A clinic can look busy online and still miss income if leads do not turn into visits. Here’s the quick math: completed visits, not clicks, pay the rent and owner draw.
Track Collected Visits
Track weekly collected visits by referral source and service line. Compare each source to the 531-visit plan and flag any channel that slows below target. One clean metric beats a pile of marketing clicks: visits completed, authorization approved, and claim collected. That shows whether capacity is filling or sitting empty.
To improve owner pay, build source relationships and shorten time to first appointment. If referrals drop and volume falls under 315 visits, fixed costs get harder to cover and cash for distributions shrinks. Keep a simple referral log, ask every new patient where they came from, and review it monthly so weak channels get fixed before they hit margin.
1
Reimbursement And Payer Mix
Reimbursement And Payer Mix
Your income here is the cash collected per visit, not the amount billed. In this model, the first-year average collection is $23,978 across all modeled services, and commercial insurance, Medicare, workers’ compensation, personal injury, and cash-pay testing can each collect differently. One payer shift can change take-home pay fast when volume is high.
The risk is denials and authorizations. If claims get stuck or underpaid, usable revenue falls even when the schedule looks full. Model this locally because billed charges are not cash, and cash timing can matter as much as the fee itself.
Measure Net Collection by Payer
Track collected visits, collection per visit, denial rate, authorization delay, and days in accounts receivable. Split the data by payer so you can see which mix lifts cash and which mix slows it. Here’s the quick math: volume × net collection per visit = usable monthly revenue.
- Monthly collected visits
- Payer mix by percent
- Net collection per payer
- Denial and write-off rates
- Authorization turnaround time
- Days in accounts receivable
- Cash-pay share
Build the forecast from local contracts and denial history, not billed charges. If a payer takes longer to pay, price that delay into cash planning and owner draws. Small reimbursement changes move margin fast when the schedule is full.
2
Service Mix And Visit Depth
Service Mix and Visit Depth
Service mix changes revenue per patient and how fast the clinic fills provider time. At modeled prices, neurology visits are $350, neuropsychology is $275, physical therapy is $175, vestibular care is $200, and occupational therapy is $185. The owner earns more when the mix fits patient need and clinical scope, not just billing goals.
Deeper care plans can raise collections if outcomes and authorization support them. Here’s the quick math: moving 10 visits from $175 PT to $275 neuropsychology adds $1,000 in gross revenue before labor. But if the extra depth slows access or adds unpaid work, profit and owner pay can flatten fast.
Price the right depth
Track revenue per patient, visits per episode of care, and the share of initial evaluations, follow-ups, neurocognitive testing, vestibular rehab, return-to-play, and care coordination. One clean rule: add depth only when the plan is clinically justified and pre-authorization is solid. If the service helps outcomes but not collections, it is not earning its keep.
- Track revenue per episode.
- Track visits per service type.
- Track authorization approval rates.
- Track provider time per visit.
Use that data to keep the mix tight. A $350 neurology visit and a $175 PT visit do not hit margin the same way, so small mix shifts matter. If deeper plans raise collections but stretch schedules, the fix is usually more capacity or tighter visit rules, not more volume at any cost.
3
Provider Utilization And Staffing Efficiency
Provider Utilization
This driver is how much paid clinician time turns into collected visits. In year one, the model assumes 65% neurologist utilization, 60% neuropsychologist utilization, 70% physical therapist utilization, 55% vestibular specialist utilization, and 50% occupational therapist utilization. Higher utilization spreads fixed payroll, including a $240,000 Medical Director and $85,000 Clinic Manager, across more revenue, so owner pay improves.
The risk is simple: if provider count grows faster than referrals, payroll rises before collections do. Once admin, billing, or clinical flow gets tight, margin stops improving even if calendars look full. The real test is collected visits per provider, not just booked hours or headcount.
Measure Collected Visits per Provider
Track utilization by specialty every week and compare it to the target mix. Use booked, completed, and collected visits, then tie each provider to cash, not activity. If one line falls short, slow hiring or trim open slots until referrals catch up.
- Collected visits by provider type
- Template fill rate
- No-show rate by specialty
- Authorization lag days
Build staffing in steps. Add support only when billing lag, no-shows, and room turnover stay steady for 4 to 6 weeks. That keeps payroll from outrunning the 315-visit break-even point and protects cash for owner draw.
4
Fixed Overhead And Startup Cost Pressure
Fixed Overhead Sets the Cash Floor
The clinic’s monthly fixed overhead is $19,650, led by $12,500 rent, $3,200 malpractice insurance, and $1,400 for utilities and data. That bill hits before referral volume settles, so owner pay only opens up after collections clear the fixed floor. If visits stay soft, the same overhead gets spread over fewer cases and compresses take-home income.
Startup equipment adds $140,000 in upfront cash needs: $45,000 neuroimaging software, $35,000 balance platform, and $60,000 physical therapy gym outfitting. That spend does not pay back until patient flow is steady, so early distributions are usually the first thing to shrink. One line to watch: cash burn before utilization stabilizes.
< /div>Hold the Burn Until Referrals Steady
Track monthly collected visits against the $19,650 fixed cost base, not booked demand. Here’s the quick math: every extra collected visit helps absorb rent, insurance, software, and admin, while weak early utilization leaves owner pay exposed. Keep the draw modest until collections can cover the fixed floor with room left for cash reserve.
- Track collected visits weekly.
- Separate fixed from variable costs.
- Buy equipment after volume proof.
- Link owner draw to cash coverage.
5
Billing, Collections, And Cash Conversion
Billing and Cash Conversion
This driver is how fast billed care turns into cash. At $127,325 in monthly collections and 6% billing and collection fees, the clinic spends about $7,640 a month just to collect. That cash matters more than charged rates, because rent, payroll, and owner draws are paid from cash, not from the claim file.
Watch clean claims, denial rates, patient balances, prior authorization, and accounts receivable (AR) timing. If AR slows, profit can look fine while the bank balance stays tight, which forces the owner to hold cash instead of taking it home. Faster collection timing supports steadier owner pay.
Track the Cash Lag
Measure collections as a percent of billed charges, not just visit count. Here’s the quick math: $127,325 × 6% = $7,640 in monthly billing and collection fees, so every delay hits both cash and margin. Track clean-claim rate, denial rate, days in AR, and patient balance aging each month.
- Track days in AR by payer.
- Separate denials by cause.
- Check unpaid patient balances weekly.
- Pre-check authorizations before visits.
- Reconcile billed charges to cash.
What this estimate hides is timing risk: a clinic can show profit and still miss owner pay if collections slip. Faster follow-up on denials and patient statements shortens the cash lag and makes distributions more dependable.
6
Compare low, base, and high concussion clinic owner income scenarios
Owner income scenarios
Income swings with visit volume, collections, staffing, and fixed clinic costs. The modeled cases show how fast owner pay can rise once the clinic fills capacity.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | This is a cautious first-year path with an early ramp and pay anchored by the Medical Director role. | This is the modeled growth path once referral flow and capacity start to stabilize. | This is the stronger earnings path once the clinic reaches mature volume and fuller capacity. |
| Typical setup | Year 1 runs 531 monthly visits and $127,325 monthly collections, with 318% margin, 65% to 80% provider capacity, and a $240,000 Medical Director salary. | Year 3 reaches 1,239 monthly visits and $306,505 monthly collections, with 561% margin and a larger clinical team supporting the load. | Year 5 reaches 2,029 monthly visits and $538,115 monthly collections, with 652% margin and the largest staffing mix in the model. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $240,000 - $486,000Low Case | $2,148,000Base Case | $4,205,000High Case |
| Best fit | Best for founders stress-testing a slow ramp and a single-provider pay floor. | Best for a steady ramp with Year 3 scale and a balanced clinic team. | Best for owners testing a mature clinic with full capacity and strong referral flow. |
Planning note: These ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Concussion Assessment and Treatment Clinic Porter's Five Forces Analysis
- Concussion Assessment and Treatment Clinic BCG Matrix
- Concussion Assessment and Treatment Clinic Business Model Canvas
- What Are The 5 Core KPI Metrics For Concussion Assessment And Treatment Clinic?
- Concussion Assessment And Treatment Clinic Business Plan Template in Pre-Written Word
- How Increase Profitability Concussion Assessment And Treatment Clinic?
- What Are Operating Costs For Concussion Assessment And Treatment Clinic?
- Concussion Clinic Startup Costs: Plan Around $80K+ in Known CAPEX
- Concussion Clinic Financial Model Template in Excel
- How to Open a Concussion Assessment Clinic in 4-9 Months
- How To Write A Business Plan To Launch A Concussion Assessment And Treatment Clinic?
- Concussion Assessment and Treatment Clinic Marketing Mix
- Concussion Assessment and Treatment Clinic Marketing Plan
- Concussion Assessment and Treatment Clinic Business Proposal
- Concussion Assessment and Treatment Clinic PESTEL Analysis
- Concussion Assessment And Treatment Clinic Pitch Deck Example Editable PPTX
- Concussion Assessment and Treatment Clinic Business SWOT Analysis
- Concussion Assessment and Treatment Clinic Value Proposition Canvas
Frequently Asked Questions
Under the model, the owner can receive $240,000 per year if they fill the Medical Director role The clinic also shows about $486,000 in first-year operating profit on $153 million in collections That profit is not guaranteed take-home because taxes, debt, reserves, and any unlisted clinician payroll come first