 Time to Open6-12 monthsLaunch runway
Time to Open6-12 monthsLaunch runwayHow To Open A Constipation Management Clinic In 6 To 12 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6-12 monthsLaunch runway  Launch Sequence7 stagesCompliance first
Launch Sequence7 stagesCompliance first Key BottleneckPayer credentialingProvider coverage
Key BottleneckPayer credentialingProvider coverage First Revenue StepInitial consultsReferral intake
First Revenue StepInitial consultsReferral intake


A constipation management clinic can typically open in 6 to 12 months if licensing, payer enrollment, EHR setup, staffing, clinical protocols, and referral outreach run in the right order The researched planning model starts Year 1 with 5 clinical role groups and modeled monthly revenue capacity of about $110,500 at Year 1 utilization assumptions The main bottleneck is payer credentialing, followed by specialist hiring and referral development First revenue should come from booked initial consultations through primary care, GI, colorectal surgery, pelvic floor therapy, and local search demand
Time to Open6-12 monthsLaunch runwayLaunch Sequence7 stagesCompliance firstKey BottleneckPayer credentialingProvider coverageFirst Revenue StepInitial consultsReferral intakeLaunch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10
Legal / licensing
- Form entity
- Get NPI
- Bind malpractice
- Build HIPAA workflows
- File permits
Site / buildout
- Sign lease
- Finalize floorplan
- Order equipment
- Complete buildout
- Install exam rooms
EHR / billing
- Select EHR
- Configure templates
- Set billing rules
- Build patient portal
- Test claims flow
Payer / contracting
- Submit payer apps
- Credential lead physician
- Enroll specialists
- Track approvals
- Load fee schedules
Hiring / training
- Confirm lead physician
- Hire physician assistant
- Hire dietitian
- Hire pelvic specialist
- Hire nurse team
Launch / marketing
- Define protocols
- Train team
- Start referrals
- Soft opening
- Go-live review
Why test the launch plan before signing the lease?
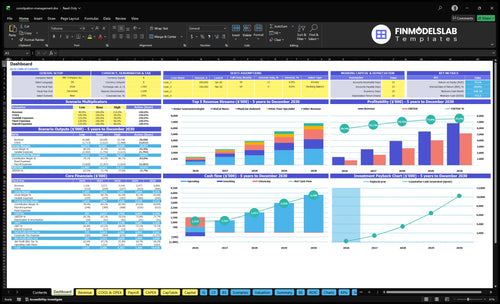
Dashboard and assumptions tabs show revenue, costs, cash needs, assumptions, and break-even logic. Open the Constipation Management Clinic Financial Model Template.
Financial model highlights
- Fixed overhead: $235k monthly
- Year 1 revenue: ~$1.105M
- Runway to break-even
How do you get patients for a constipation clinic?
Patients for a Constipation Management Clinic usually come first from primary care referrals, GI specialist networks, colorectal surgeons, pelvic floor therapy partners, local search, and patient education. The first revenue step is booked initial consultations, and before outreach you need referral forms, scheduling scripts, insurance verification, and follow-up workflows in place; see What Are Operating Costs For Constipation Management Clinic? for the cost side.
Where patients come from
- Primary care sends first referrals.
- GI specialists feed complex cases.
- Colorectal surgeons and therapists refer.
- Search visibility drives local bookings.
What must work first
- Book consults, not broad campaigns.
- Set scripts for intake and follow-up.
- Verify insurance before the visit.
- Model Year 1 below full capacity: 65%, 50%, 40%, 45%, 55%.
How long does it take to open a constipation clinic?
A Constipation Management Clinic usually takes 6 to 12 months to open. The biggest gating item is payer credentialing, because insurer approval can block paid visits, so start it early. The electronic health record (EHR), lease, buildout, and provider hiring all need to be lined up before scheduling goes live.
Start early
- Start payer credentialing first
- Lease must fit exam room flow
- Buildout needs privacy and ADA access
- Vendor setup should match the room plan
Protect opening day
- Finish EHR before scheduling opens
- Hire specialists to fill appointment slots
- Start referrals before soft opening
- Watch billing and referral activation bottlenecks
What do you need to open a constipation management clinic?
You need compliance cleared first: licensed physician leadership, a compliant medical entity, malpractice coverage, payer enrollment, National Provider Identifier setup, HIPAA-ready systems, EHR, billing, staff, diagnostics, and treatment protocols. For a deeper startup cost view, see How Much To Open Constipation Management Clinic Business?; the first revenue gate is legal setup before predictable patient volume from adults with symptoms lasting more than 3 months.
Must-Haves
- Licensed physician medical leadership
- Compliant medical entity structure
- Malpractice insurance coverage
- Payer enrollment and NPI setup
Year 1 Team
- 1 senior gastroenterologist
- 1 physician assistant
- 1 registered dietitian
- 1 pelvic floor specialist and 2 nurses
Confirm whether the clinic is safe, legal, and operationally ready to open
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Regulatory
- Entity and licenses activeCritical
No opening until the medical entity and state licenses are live.
- Malpractice policy boundHigh
Coverage must start before the first patient visit.
- NPI and payer enrollment doneHigh
Claims will stall if payers are not active at launch.
Clinic setup
- Lease and buildout signed offCritical
You need a usable site before scheduling the first visit.
- Rooms meet privacy and ADAHigh
Patients need private rooms and accessible entry on day one.
- Equipment installed and testedHigh
Manometry, transit, ultrasound, and biofeedback must work before intake.
Care flows
- HIPAA workflows and consents readyHigh
Protected health data needs a clear path before opening.
- Intake templates loaded in EHRHigh
Templates keep first visits consistent and cut charting delays.
- Triage and follow-up rules setHigh
Clear routing and follow-up reduce missed care and repeat calls.
Vendors
- Labs and imaging vendors contractedHigh
External testing needs a working handoff before the first referral.
- Billing and claims workflow testedHigh
Cash depends on clean claims and fast payer follow-up.
- Scheduling, portal, and telecom liveMedium
Patients need a way to book, confirm, and reach the clinic.
Staffing
- Year 1 care team staffedHigh
Opening needs the gastroenterologist, PA, dietitian, pelvic floor specialist, and nurses.
- Practice manager onboardedHigh
This role drives flow, staffing, and issue control.
- Training completed on protocolsHigh
Staff should know intake, escalation, and referral steps before go-live.
Cash
- Launch cash covers Month 2Critical
The model shows minimum cash in Month 2, so runway matters early.
- Fixed overhead fits modelHigh
Lease, insurance, software, and admin spend must stay inside plan.
- Go-live signoff approvedCritical
Do not open if credentialing, templates, billing, or scheduling are still open.
Which launch drivers matter most before opening?
1Credentialing
Payer gatePayer enrollment clears insured visits and keeps opening schedules from filling with out-of-network claims.
2Clinical Design
ProtocolsDocumented consult, triage, and follow-up paths keep patients moving and reduce missed handoffs.
3Location Access
Access readyA private, ADA-ready office with portal and front desk flow cuts no-shows and speeds intake.
4Staff Capacity
5-clinician teamThe Year 1 team of five clinicians keeps day-one capacity realistic and avoids schedule gaps.
5Referral Network
8% revReferral forms and outreach cadence fill the calendar faster and reduce the risk of an empty launch.
6Revenue Cycle
Live billingLive coding, verification, and claims submission tighten cash collection and cut denied visits.
Credentialing And Compliance
Credentialing And Compliance
Credentialing and compliance are the gate for opening this constipation clinic on time because insured visits are not really “ready” until the physician has active licensure, malpractice coverage, a National Provider Identifier, payer applications in motion, and signed contracts where needed. If any one of those is missing, the first schedule can fill with visits that turn into unpaid or out-of-network claims.
For day-one operations, this work also includes HIPAA workflows, privacy policies, billing permissions, entity setup, state rule review, compliance files, EHR access controls, and patient consent forms. The bottleneck is usually incomplete documentation, not the clinical plan. One clean rule: if the payer file is not ready, the appointment should not be treated as fully reimbursable.
Lock The Payer File Before The Calendar Opens
Start with physician leadership and make one owner responsible for the full credentialing packet. Verify licensure, malpractice proof, NPI setup, and all payer applications before you open booking. That keeps the launch schedule honest and lowers the chance that early insured patients get billed wrong or sit in out-of-network status.
Then sequence the compliance work fast: entity setup, state rule review, HIPAA policies, EHR access controls, and signed consent forms. Here’s the quick test: if front desk, billing, and clinical staff cannot answer what is covered, what is documented, and who can access records, the clinic is not ready to see its first patient.
- Confirm licensure and malpractice first.
- Submit payer applications early.
- Document consent and privacy steps.
- Restrict EHR access by role.
- Do not schedule before billing permissions.
1
Clinical Service Design
Clinical workflow and handoff design
The clinic can’t open cleanly without a clear visit path for consults, diagnostic workups, medication management, nutrition counseling, pelvic floor referrals, motility testing links, follow-up cadence, and escalation criteria. The readiness signal is documented protocols and handoffs between the senior gastroenterologist, physician assistant, registered dietitian, pelvic floor specialist, and clinical nurses. If triage is loose, day-one flow turns into delays, duplicate work, and messy notes.
One clean handoff is worth more than another open slot. The big risk is inconsistent follow-up, because that slows care, weakens referral confidence, and creates chart gaps that are hard to fix after launch.
Map the care path before the schedule opens
Build the first-visit script, workup checklist, and follow-up rules before the first patient books. Tie each visit type to an owner, a handoff, and a next step, then test the flow with the full team. That keeps the clinic aligned with the Year 1 staffing plan, where capacity only works if roles run at 40% to 65% utilization without gaps.
- Define consult, workup, and follow-up slots.
- Assign who escalates unresolved cases.
- Document referral and motility test links.
- Standardize nurse, PA, and RD handoffs.
2
Location And Patient Access
Location Access
For a constipation clinic, location is not just real estate. It decides whether patients can get in easily, feel private, park without stress, and move through check-in and exam rooms without delay. A leased and equipped medical office with portal, telecom, utilities, maintenance, and front-desk workflow ready is the launch signal that you can see patients on day one.
The fixed facility load is already heavy: $12k per month for lease plus $18k per month for utilities and maintenance, or $30k per month before staffing. The risk is opening in space that cannot handle referral volume or private visits. That can slow intake, hurt patient trust, and push no-shows up right when the schedule should be filling.
Ready the Site Before First Visits
Verify the space against the real patient flow: parking, ADA compliance (Americans with Disabilities Act), referral-source proximity, lab and imaging links, room flow, and check-in steps. If any one of those is weak, opening day gets messy fast. One clean visit path matters more than a polished lobby.
- Test portal, phones, and intake forms.
- Confirm front-desk coverage and scripts.
- Walk the path from parking to exam room.
- Check privacy in waiting and consult areas.
- Match room count to referral demand.
Here’s the quick math: if access problems slow check-in or make visits feel exposed, patients delay care and schedules get thin. A site that supports private digestive health visits and fast intake helps the clinic start with fewer no-shows and cleaner first-day operations.
3
Staffing And Provider Capacity
Day-One Provider Coverage
The clinic’s opening date depends on whether each clinician is scheduled, credentialed, and backed up. With 1 senior gastroenterologist, 1 physician assistant, 1 registered dietitian, 1 pelvic floor specialist, and 2 clinical nurses, a shortfall in any role cuts real appointment capacity fast and can delay first revenue.
Year 1 utilization is only 40% to 65%, so the schedule must be built on realistic slots, not full theoretical capacity. Here’s the quick math: the 160-slot role becomes 64 to 104 treatments, and the 200-slot nurse role becomes 80 to 130. One staffing gap can turn a full clinic into a half-empty calendar.
Build Backup Into The Schedule
Lock coverage before the first patient books. Confirm named people for visit flow, patient education, billing support, and same-week backfill so no role depends on one person. If the clinic opens with no backup, PTO, illness, or onboarding delays will show up immediately as lost slots and slower ramp.
- Map slots by role and room.
- Test intake, education, and billing handoffs.
- Cross-train nurses on patient flow.
- Hold backup coverage for absences.
4
Referral Network Development
Referral Network Development
This driver decides whether the clinic opens to a real patient flow or an empty schedule. Early demand has to come from primary care physicians, gastroenterologists, colorectal surgeons, pelvic floor therapists, local search visibility, and patient education content, so the referral path must be live before the first appointment slot opens.
The launch risk is simple: no referrals, no first consults. Readiness means referral forms are ready, the contact list is built, outreach cadence is set, scheduling scripts are written, insurance verification works, and referring clinicians get a feedback loop. Keep all outreach factual and avoid cure claims or guaranteed outcomes.
Build the referral engine before opening
Start with a clean referral packet for each source group, then test it with a short outreach list and a booked-first-visit workflow. If the front desk cannot answer referral calls, verify insurance, and place patients fast, the schedule can slip even when demand exists.
Use digital patient acquisition as support, not the whole plan: it is modeled at 8% of revenue in Year 1 and 5% by Year 5. The goal is not just traffic; it is first consultations and a steadier ramp.
- Confirm referral forms before launch.
- Load a verified contact list.
- Set outreach cadence by source.
- Train scheduling and insurance scripts.
- Close the loop with referring clinicians.
5
Revenue Cycle Readiness
Revenue Cycle Ready
A constipation clinic can’t open cleanly if EHR and billing are not live before the first visit. Revenue depends on coding workflows, documentation templates, insurance verification, claim submission, patient balances, scheduling rules, denial follow-up, and payer mix tracking, so a weak setup turns day-one visits into slow cash and avoidable denials. Billing and claims fees are modeled at 4% of revenue in Year 1, with external lab and imaging fees starting at 4% too.
Here’s the quick math: the software stack is modeled at $22k per month, so this is not a back-office detail. It is a launch gate. If claims are not clean at first submit, cash collection slows, patient balances pile up, and the clinic may be open but still not functioning like a real business.
Set Billing Live First
Before opening, verify that each visit type has a code, a note template, and a charge path. Test insurance checks at scheduling, claim edits before submission, and denial handling after submission. Build a payer mix report on day one so you can see which plans drive cash and which ones slow it down.
One clean claim beats ten rushed visits. Assign one person to check patient balances, one to track denials, and one to confirm the billing queue is moving before the first appointment hits the schedule.
- Test coding on real visit types.
- Verify benefits before booking.
- Reconcile balances weekly.
- Track denials by payer.
6
Related Products
- Constipation Management Clinic Porter's Five Forces Analysis
- Constipation Management Clinic BCG Matrix
- Constipation Management Clinic Business Model Canvas
- What 5 KPIs Should Constipation Management Clinic Business Track?
- Constipation Management Clinic Business Plan Template in Pre-Written Word
- How Increase Profits For Constipation Management Clinic?
- What Are Operating Costs For Constipation Management Clinic?
- Constipation Management Clinic Startup Costs: $310K+ Before Runway
- Constipation Management Clinic Financial Model Template in Excel
- How Much Can a Constipation Management Clinic Owner Make? $570K Year 1
- How To Write A Business Plan For Constipation Management Clinic?
- Constipation Management Clinic Marketing Mix
- Constipation Management Clinic Marketing Plan
- Constipation Management Clinic Business Proposal
- Constipation Management Clinic PESTEL Analysis
- Constipation Management Clinic Pitch Deck Example Editable PPTX
- Constipation Management Clinic Business SWOT Analysis
- Constipation Management Clinic Value Proposition Canvas
Frequently Asked Questions
Start with physician leadership, a compliant medical entity, payer enrollment, malpractice coverage, EHR, billing, and written care pathways The planning model assumes a 6 to 12 month launch and Year 1 staffing of 1 senior gastroenterologist, 1 physician assistant, 1 registered dietitian, 1 pelvic floor specialist, and 2 clinical nurses