 Owner income$787K-$5.1M
Owner income$787K-$5.1MHow Much Can a Constipation Management Clinic Owner Make? $570K Year 1

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$787K-$5.1M  Net margin59%-76%
Net margin59%-76% Revenue for target pay$1.33M
Revenue for target pay$1.33M Business difficultyHard
Business difficultyHard


A constipation management clinic owner can make meaningful income if collections are high enough to cover staffing, fixed overhead, billing, marketing, and reserves In the researched assumptions, the clinic collects about $1105K per month in the first year and $5672K per month by Year 5 Operating profit after listed costs is about $570K in Year 1 and $511M in Year 5, but that is not guaranteed owner take-home The estimate excludes clinical provider salaries, debt service, taxes, and required reserves
Owner income$787K-$5.1MNet margin59%-76%Revenue for target pay$1.33MBusiness difficultyHardWant to test your own owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice, and it excludes startup CAPEX and one-time opening costs.
How do you check owner income in the model?
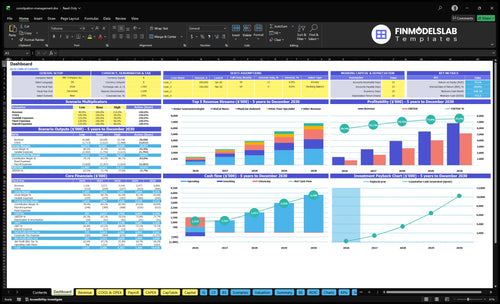
It shows revenue, margin, costs, reserves, and owner take-home assumptions in the Constipation Management Clinic Financial Model Template; open it. Charts compare $133M Year 1, $392M Year 3, and $681M Year 5 revenue, and tables show COGS at 10% and 72% plus variable expenses from 12% to 8%.
Owner income model highlights
- Owner take-home output
- Revenue and margin view
- Scenarios and assumptions
Can a constipation management clinic be profitable and scalable?
Yes—the Constipation Management Clinic can be profitable if referral flow and utilization stay strong, because its fee-for-service model scales with practitioner capacity. In Year 1, the owner-operated setup uses 1 senior gastroenterologist, 1 physician assistant, 1 dietitian, 1 pelvic floor specialist, and 2 nurses; by Year 5, it grows to 3, 3, 2, 2, and 6, so the main risk is collections and the unmodeled cost of non-owner clinical payroll.
Why it can scale
- Revenue tracks practitioner capacity.
- Year 1 stays lean and focused.
- Year 5 adds more clinical reach.
- Specialized care supports repeat demand.
Main profit risks
- Referral flow can slow volume.
- Utilization can miss capacity.
- Collections can weaken cash.
- Clinical payroll can outrun revenue.
What should a constipation clinic owner pay themselves?
Pay yourself from collected revenue, not from the $570K Year 1 operating profit alone. If you work as the senior gastroenterologist in the Constipation Management Clinic, first set fair clinical pay for your labor, then treat the rest as true profit after reserves, debt service, and reinvestment.
Set pay in this order
- Start with collected cash, not booked revenue.
- Price owner clinical work at replacement cost.
- Hold cash for reserves and debt service.
- Keep reinvestment separate from salary.
Don’t overstate distributions
- $570K is not all take-home pay.
- Clinical payroll and taxes come first.
- Owner labor needs fair market pay.
- Residual profit is what you can distribute.
What affects constipation management clinic profit margin?
At the Constipation Management Clinic, profit margin moves with payer mix, collections rate, provider utilization, and service mix, so even small billing leaks matter; for the cost stack, see What Are Operating Costs For Constipation Management Clinic? The model shows $235K in monthly fixed overhead, $182K in Year 1 admin wages, plus 10% COGS and 12% variable expenses, with a projected 430% margin after listed costs. Every denied claim, empty slot, or slow authorization cuts owner take-home and reserve capacity.
Margin drivers
- Payer mix changes collections.
- Utilization sets provider output.
- Service mix shifts revenue per visit.
- No-shows leave revenue on the table.
Cost pressure
- Rent stays fixed.
- Malpractice insurance adds overhead.
- EHR and billing fees stack fast.
- Equipment and admin wages stay costly.
Want the six income drivers that matter most?
1
524-2,387Patient Volume
More visits are the main growth engine, and the model scales from 524 monthly treatments in Year 1 to 2,387 in Year 5.
2
65%-90%Provider Utilization
Higher schedule fill turns the same provider base into more revenue, so empty slots hurt EBITDA fast.
3
$100-$510Reimbursement Mix
A better payer mix and higher visit rates lift realized revenue, since treatment prices run from $100 to $510.
4
430%-751%Service Mix
More higher-value diagnostics and ancillaries widen listed-cost margin, which drops more cash to the owner.
5
$41K/moOverhead Control
Fixed overhead starts near $41K a month, so once volume clears that base, extra revenue falls through faster.
6
4%-3%Collections Discipline
Tighter claims handling keeps billing fees near 3% instead of 4%, so less cash leaks after the visit.
Constipation Management Clinic Core Six Income Drivers
Patient Volume
Patient Volume
When referral flow, consult demand, follow-up cadence, and slot fill rate improve, planned monthly treatments rise from 524 in Year 1 to 2,387 in Year 5. That lifts monthly revenue from $1,105K to $5,672K; the implied revenue per treatment is about $2.1K to $2.4K.
The risk is hiring before demand shows up. Every empty slot still carries fixed overhead, so open capacity burns cash and delays owner pay. Watch referrals, no-shows, and rebooking speed weekly; if slots stay open, protect margin before adding staff.
Fill Slots Before You Expand
Estimate volume from referral flow, consult demand, follow-up cadence, and filled appointment slots. If these inputs are soft, collections stay soft too, because the clinic only earns when treatment time is booked and kept.
- Track referral source by week.
- Track consult show rate.
- Track follow-up rebook rate.
- Track open slots by provider.
Use those counts to decide when to add staff. If volume rises first, fixed overhead is spread across more visits and owner take-home improves faster; if staffing rises first, profit gets squeezed before cash comes in.
1
Reimbursement And Payer Mix
Reimbursement and Payer Mix
Reimbursement and payer mix is the cash you actually collect from commercial insurance, Medicare, Medicaid, and cash-pay after denials and patient balances. Use collected revenue, not billed charges, because owner take-home can fall before profit looks weak.
Year 1 prices range from $100 for clinical nurse visits to $450 for senior gastroenterologist visits, rising to $120 and $510 by Year 5. Same visit count, different payer mix, different cash. Track collection rate by payer and service line.
Track Net Collections by Payer
Measure commercial, Medicare, Medicaid, cash-pay, denials, and patient balances each month. The core inputs are visit volume, payer mix, denial rate, and how fast patients pay. If collections slip, the clinic may look busy but still leave the owner short on draw.
- Review denial reasons weekly.
- Check patient balance aging.
- Verify eligibility before visits.
- Collect copays at check-in.
- Match staffing to paid volume.
Use net collections in the forecast, then stress test weaker payer mix or slower collections. That shows whether owner pay holds up when cash comes in late, even if visit volume stays flat.
2
Diagnostic And Ancillary Service Mix
Service Mix per Patient
This driver changes revenue per patient by shifting the share of gastroenterology consults, follow-ups, registered dietitian visits, pelvic floor specialist visits, nurse visits, and diagnostic activity. The model also includes medical consumables and diagnostic kits, which are 60% of revenue in Year 1 and 40% by Year 5. Only medically appropriate activity should be modeled, since unused services do not add income.
What matters is collected revenue per case, not just visit count. A clinic can see the same 524 treatments in Year 1 or 2,387 by Year 5, but a different mix of consults, follow-ups, and diagnostics will change cash flow, direct supply use, and owner pay. If the mix skews too hard toward low-yield activity, profit per patient drops.
Track Mix by Visit Type
Measure collected revenue, kit usage, and direct cost by service line every month. Compare actual case mix with the planned shift from 60% to 40% revenue from consumables and kits, then test whether consults and follow-ups are covering the gap in collected dollars.
Forecast from approved care paths, average collected price, and payer mix. Keep the schedule aligned to medically needed visits only, because extra kit use can pull cash into inventory and supplies before it reaches owner income.
3
Provider Utilization
Provider Utilization
Utilization turns provider hours and room capacity into collections. Year 1 planned volume is 524 treatments against 1,000 monthly capacity, or about 52.4%. By Year 5, 2,387 treatments against 2,740 capacity is about 87.1%. As schedules fill, more fixed payroll gets spread over more visits, so owner income improves if the clinic avoids unsafe overbooking.
The main inputs are available slots, booked treatments, and staffing mix. Benchmarks move from 65% to 90% for the senior gastroenterologist, 50% to 85% for the physician assistant, and 55% to 90% for the clinical nurse. What this hides: if demand slows or no-shows rise, revenue drops fast while labor and room costs stay in place.
Track Fill Rate by Provider
Measure booked visits versus open slots each week, then split the view by provider type. Keep a close eye on the gap between capacity and volume; a clinic at 52.4% in Year 1 should tighten referral flow and recall systems before adding staff. One simple rule: do not hire ahead of sustained fill.
Use waitlists, follow-up booking, and referral tracking to push each role toward its utilization range. Keep growth tied to safe clinical pacing, because overbooking can lift short-term collections but hurt care quality, denials, and patient retention, which then pulls owner take-home income back down.
4
Operating Overhead
Operating Overhead
Operating overhead is the fixed monthly cost load before the first patient visit clears. Here, the base is $235K per month for lease, malpractice insurance, clinical software, utilities, office supplies, portal hosting, and compliance. Admin wages add $182K in Year 1 and $376K by Year 5, so owner pay only starts after a very large fixed nut is covered.
Here’s the quick math: $235K a month is $2.82M a year in core overhead, before admin wages. If volume or collections slip, those costs stay put, so profit and cash flow fall fast. The key inputs are rent, insurance, software, utilities, support staff, and compliance hours; each extra dollar needs real collections, not just more bookings.
Control the fixed nut
Track overhead by line item each month and tie admin staffing to booked visits and claim load. Watch overhead as a share of collected revenue, plus admin wa ge dollars per visit, so you can see when growth is funding profit instead of just feeding fixed costs.
- Review lease and software annuals.
- Match admin hours to volume.
- Protect compliance spend.
- Cut waste, not care.
5
Collections Discipline
Collections Discipline
This driver is the revenue cycle: visits, denials, coding, prior auth, patient balances, and no-shows. In this clinic, booked care only helps the owner if it becomes cash. With billing and claims processing fees at 40% of revenue in Year 1 and 30% from Year 3 onward, cleaner collections leave more for overhead and owner pay.
Here’s the quick math: on $100 collected, fee drag is $40 in Year 1 and $30 from Year 3 on. What this hides is timing risk: if claims sit, denials rise, or balances age, cash flow weakens even when the schedule looks full, and the owner’s draw gets pushed back.
Tighten the cash path
Track denial rate, days in accounts receivable, prior-auth turnaround, no-show rate, and patient balance aging by payer and visit type. The goal is simple: every completed visit should hit cash fast. If a code is wrong or auth is late, the clinic keeps the cost but loses the cash timing.
Use a same-day billing rule, verify eligibility before the visit, and send patient statements on a weekly cadence. Watch fee drag against the model’s 40% Year 1 and 30% Year 3 benchmarks. If collections slip, protect owner pay only after the revenue cycle is fixed, not before.
6
Compare lean, base, and high-performing owner-income cases
Owner income scenarios
Owner income rises with visit volume, pricing, and staff use. Year 1 is the lean case, Year 3 is the base case, and Year 5 shows the stronger capacity path.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | This is the lower owner-income path with Year 1 scale and early utilization. | This is the modeled owner-income path with Year 3 volume and steadier operations. | This is the stronger owner-income path with Year 5 scale and fuller throughput. |
| Typical setup | Year 1 runs at $1.326M revenue, 524 monthly treatments, about 43.0% margin, and $570k operating profit before provider payroll, debt, taxes, reserves, and startup costs. | Year 3 runs at $3.918M revenue, 1,448 monthly treatments, about 68.1% margin, and $2.67M operating profit before provider payroll, debt, taxes, reserves, and startup costs. | Year 5 runs at $6.806M revenue, 2,387 monthly treatments, about 75.1% margin, and $5.11M operating profit before provider payroll, debt, taxes, reserves, and startup costs. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $570kLow case plan | $2.67MBase case plan | $5.11MHigh case plan |
| Best fit | Use this to stress-test early demand and capacity fill in the first operating year. | Use this as the main planning case for budgeting and hiring. | Use this to test upside if demand, staffing, and room use all land well. |
Planning note: Scenario figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Constipation Management Clinic Porter's Five Forces Analysis
- Constipation Management Clinic BCG Matrix
- Constipation Management Clinic Business Model Canvas
- What 5 KPIs Should Constipation Management Clinic Business Track?
- Constipation Management Clinic Business Plan Template in Pre-Written Word
- How Increase Profits For Constipation Management Clinic?
- What Are Operating Costs For Constipation Management Clinic?
- Constipation Management Clinic Startup Costs: $310K+ Before Runway
- Constipation Management Clinic Financial Model Template in Excel
- How To Open A Constipation Management Clinic In 6 To 12 Months
- How To Write A Business Plan For Constipation Management Clinic?
- Constipation Management Clinic Marketing Mix
- Constipation Management Clinic Marketing Plan
- Constipation Management Clinic Business Proposal
- Constipation Management Clinic PESTEL Analysis
- Constipation Management Clinic Pitch Deck Example Editable PPTX
- Constipation Management Clinic Business SWOT Analysis
- Constipation Management Clinic Value Proposition Canvas
Frequently Asked Questions
The model shows about $570K of first-year operating profit after listed COGS, variable expenses, fixed overhead, and admin wages That comes from $1326M in annual revenue, 524 monthly treatments, and a 430% listed-cost margin It is not final owner take-home because clinical provider payroll, taxes, debt, and reserves are excluded