 Time to Open8-16 weeksOpening prep
Time to Open8-16 weeksOpening prepHow To Open Contact Dermatitis Patch Testing In 8–16 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open8-16 weeksOpening prep  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckPayer gatePayer approvals
Key BottleneckPayer gatePayer approvals First Revenue StepConsult bookedReferral intake
First Revenue StepConsult bookedReferral intake


You can often open a contact dermatitis patch testing service in about 8 to 16 weeks if licensed clinical capacity, exam space, allergen panel sourcing, electronic health record scheduling, payer setup, and referral outreach are already moving The researched Year 1 model assumes 1 Senior Dermatologist, 1 Physician Assistant, 1 Nurse Practitioner, 1 Clinical Specialist, and 2 Allergy Technicians supporting about 242 treatments per month at ramped capacity First revenue starts when referred patients complete the consult, patch placement, 48-hour reading, and delayed follow-up The common bottleneck is payer credentialing, provider enrollment, and dependable allergen supply
Time to Open8-16 weeksOpening prepLaunch Sequence6 stagesCompliance firstKey BottleneckPayer gatePayer approvalsFirst Revenue StepConsult bookedReferral intakeLaunch timeline
Short web summary of the launch plan; the XLSX export contains the detailed Gantt chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9
Clinical governance
- Confirm medical authority
- Bind malpractice coverage
- Draft clinical protocols
- Approve consent forms
Compliance and credentialing
- Check licensing status
- Set HIPAA controls
- Submit credentialing packet
- File payer enrollments
- Close compliance binder
Facility setup
- Finish clinic buildout
- Install exam rooms
- Set secure storage
- Add clinic signage
Vendor onboarding
- Shortlist panel vendors
- Compare panel quotes
- Sign supply contracts
- Receive initial stock
EHR and billing
- Configure EHR workflow
- Build visit templates
- Set billing rules
- Test claims routing
Staffing and launch
- Hire coordinator
- Train team
- Run mock visits
- Start referral outreach
- Open soft launch
- Book first patients
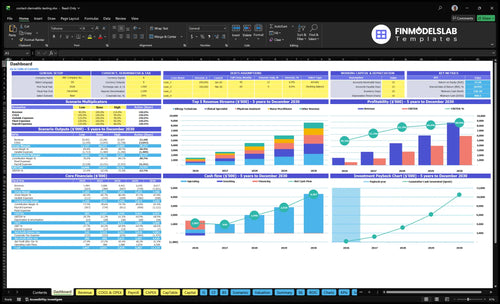
Why test the financial model before opening Contact Dermatitis Patch Testing?
This screenshot shows revenue, costs, cash needs, assumptions, and break-even logic—open the Contact Dermatitis Patch Testing Financial Model Template.
Financial model highlights
- Launch timing and ramp
- Provider and staff scheduling
- Runway and break-even path
What do you need to open a patch testing clinic?
To open a Contact Dermatitis Patch Testing clinic, you need licensed clinical authority before launch: provider licensure, a medical director or supervising physician, malpractice coverage, written protocols, patient consent, emergency escalation, Health Insurance Portability and Accountability Act (HIPAA) controls, Occupational Safety and Health Administration (OSHA) procedures, and state medical compliance. The launch blocker is unclear scope of practice or missing supervision, not demand; the model serves millions of Americans with chronic rashes, eczema, and suspected contact dermatitis, and the profit side is covered here: How Increase Profits From Contact Dermatitis Patch Testing?
Launch Must-Haves
- Confirm provider licensure before opening
- Set 1 Medical Director structure
- Carry active malpractice coverage
- Use written clinical and consent protocols
Year 1 Staffing
- Hire 1 Senior Dermatologist
- Staff 1 Physician Assistant and 1 Nurse Practitioner
- Add 1 Clinical Specialist and 2 Allergy Technicians
- Run admin with 1 Practice Manager and 1 Patient Coordinator
How do you get patients for patch testing?
Get patients for Contact Dermatitis Patch Testing by starting with referrals, not broad ads, and use What Is The Monthly Operating Cost For Your Business? Please Provide The Business Name. to check overhead before you spend. The first channels should be dermatologists, allergists, primary care physicians, occupational medicine clinics, employer health programs, and self-pay patients with persistent rash or suspected allergic contact dermatitis. In Year 1, the model sets Physician Referral Outreach at 25% of revenue and Marketing and Website Hosting at $2,200 per month, so the key is getting referred patients scheduled through the full multi-visit testing path.
Start with referrals
- Target dermatologists first
- Reach allergists and PCPs
- Use occupational medicine clinics
- Ask employer health programs
Then capture demand
- Serve self-pay rash patients
- Focus on persistent dermatitis searches
- Budget 25% for outreach
- Keep hosting and marketing at $2,200/month
How long does it take to start patch testing?
Contact Dermatitis Patch Testing usually takes about 8 to 16 weeks to start when licensing, space, vendors, billing setup, and referral work move in parallel. A new standalone site can take longer if payer credentialing and state filings are not ready. Here’s the quick math: you need room for consult, placement, 48-hour reading, and delayed reading from day one.
Main delays
- Payer credentialing slows opening
- Provider enrollment can bottleneck billing
- Allergen panels need procurement lead time
- EHR billing setup takes time
Launch schedule
- Build consult slots first
- Reserve placement visits next
- Hold 48-hour reading capacity
- Leave room for delayed readings
Confirm the clinic is ready before accepting referrals
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening and taking first patients.
Compliance
- Clinician licenses verifiedCritical
No patient care can start until each clinician is licensed in the clinic state.
- Supervising structure approvedCritical
Patch testing needs a clear supervising provider chain before the first visit.
- Malpractice coverage boundCritical
Coverage must be active before any patient is seen or staff is scheduled.
- State board rules reviewedHigh
State medical board rules can change who may test and who may supervise.
- CLIA need assessedMedium
This matters if lab testing is added alongside patch testing.
Safety
- Consent form approvedCritical
Patients need written consent before allergens are applied to the skin.
- Patch instructions readyHigh
Clear home instructions lower missed reads and avoidable reactions.
- Emergency response testedHigh
Staff need a set response if a patient has a strong skin reaction.
- Allergy history intake setMedium
Good intake helps match the right panel and avoid wasted visits.
Facility
- Exam room layout setHigh
The room must support application, read visits, and safe patient flow.
- Allergen storage controls workingCritical
Panels can fail if storage is off, so control matters before opening.
- Expiration tracking activeHigh
Expired panels create clinical risk and waste inventory dollars.
- Reading equipment calibratedHigh
Accurate reads support clean charting and payer defense.
Billing
- CPT 95044 codedCritical
Coding must be set before the first claim goes out.
- Payer workflows testedCritical
Claims need a working path or first revenue will stall.
- Claim denial steps readyMedium
Denied claims are common, so a fast fix loop protects cash.
- Referral pipeline seededHigh
No referral flow means empty schedules even with a ready clinic.
Staffing
- Technician training signed offCritical
Training must cover panel handling, placement, and read timing.
- Multi-visit scheduling trainedHigh
Patch testing needs follow-up visits booked before the patient leaves.
- Escalation paths assignedHigh
Staff must know who handles reactions, billing issues, and no-shows.
- Coverage model staffedMedium
Coverage has to match the Year 1 team plan or visits will back up.
Finance
- Launch cash runway checkedCritical
Cash must cover the $808k minimum and the Month 2 low point.
- Fixed overhead budgetedHigh
Rent, insurance, software, and payroll need a locked monthly plan.
- Startup capex fundedCritical
Buildout, inventory, and IT spend must be funded before opening.
- Go-live signoff completeCritical
The final signoff should confirm compliance, staff, supply, and billing.
Which launch drivers matter most before opening?
1Clinical Authority
8-16 wkLicensure, oversight, and compliance gates shape the 8-16 week launch window and avoid claim and consent failures.
2Billing Readiness
Claim readyEnrollment, CPT 95044 setup, and claim workflows speed first reimbursements and reduce denials.
3Allergen Vendors
Panels readyVendor-ready panels with backup supply prevent canceled placements and keep launch dates on track.
4Workflow Scheduling
242 tx/moBooked consult, placement, and reading slots protect the 242-treatment run rate and reduce complaints.
5Staffing Protocols
2 techsTwo trained technicians and clear escalation steps make day-one patch placement safer and steadier.
6Referral Pipeline
$124K/moActive referral outreach fills the modeled $124K monthly run rate faster and supports first revenue.
Clinical Authority And Compliance
Clinical Authority
Licensed provider readiness is the first launch gate for patch testing. Before opening, the business needs documented licensure, Medical Director oversight, malpractice coverage, patient consent, HIPAA safeguards, OSHA procedures, and state medical board compliance. If supervision is unclear, the launch can stall even when rooms, staff, and supplies are ready.
No license, no launch. Tight clinical authority lowers claim, consent, and care-quality failures on day one.
Preopen Compliance Check
Lock protocol approval, scope of practice, adverse reaction escalation, and documentation standards before the first patient is booked. The Medical Director should sign off on who can place patches, who reads reactions, and who escalates issues. That keeps the first billable cases from getting delayed by missing approvals or charting fixes.
- Document provider licensure.
- Name the Medical Director.
- File consent workflows.
- Test HIPAA access controls.
- Post OSHA procedures.
- Define reaction escalation.
1
Payer And Billing Readiness
Payer And Billing Readiness
Patch testing can be clinically ready and still miss opening on time if billing is not set up. Provider enrollment, payer contracts, prior authorization rules where needed, and CPT 95044 setup must be done before the first referrals turn into cash. If these pieces lag, services happen first and reimbursement comes later, which strains working capital.
For Year 1, Medical Billing and Claims Processing are modeled at 50 percent of revenue, so weak claim setup becomes a real launch risk, not an admin issue. Clean templates, claim workflows, and collection tracking protect first revenue and cut denials. If reimbursement is slow, the clinic can look busy while cash stays tight.
Set Claims Up Before First Visits
Build the billing stack before the schedule opens. The founder should verify payer enrollment, confirm contract status, map any prior authorization steps, and test how patch testing will be billed under CPT 95044. One clean claim on paper is worth more than ten future fixes.
- Lock documentation templates first.
- Test claim submission end to end.
- Track denials and unpaid claims weekly.
- Assign one owner for collections.
That sequence keeps the first referrals from becoming delayed cash. It also reduces avoidable denials, which is the fastest way to protect opening liquidity and keep day-one operations stable.
2
Allergen Panels And Vendors
Allergen Panel Supply Readiness
Patch testing panels define what you can actually see on day one. If the standard or expanded testing series isn’t selected, ordered, and stored with active vendor accounts, the clinic can open late or cancel first placements. That hits patient trust fast, because the service only works when the right allergens are on hand and ready.
The setup also needs storage controls, expiration tracking, a backup supply process, and stocked placement supplies. Year 1 planning puts Allergen Test Kits and Panels at 120% of revenue and Clinical Disposal and Medical Consumables at 30%, so weak inventory control turns into a cash and service bottleneck, not just a purchasing issue.
Lock Vendor Coverage Before Booking Patients
Before scheduling the first patch test, verify which allergens are in the standard series and which require expanded testing. Then confirm vendor lead times, re-order points, and a named backup supplier so a missed shipment does not stop placements. One clean rule helps: no stocked panel, no booking.
Use a simple readiness check for first-day supply: vendor accounts active, inventory counts current, expiration dates logged, placement materials stocked, and disposal supplies on site. That lowers the risk of inconsistent inventory, which is the main reason early placements get canceled and provider confidence drops.
3
Workflow And Scheduling
Patch Test Scheduling
This launch driver decides whether the clinic can open on time and finish each case cleanly from day one. A patch testing service needs a locked schedule for consult, patch placement, 48-hour reading, and delayed reading, plus time for documentation and follow-up interpretation. If those slots are not protected, the service looks open but cannot complete care.
The weak point is overbooking placement visits without enough reading capacity. That creates late results, messy records, and patient frustration when staff have to reschedule reactions or explain next steps after the fact. One clean rule: every placement slot needs a matching read slot before opening the calendar.
Protect Reading Slots
Build the schedule backward from the 48-hour reading and the delayed read, then fit consults and placement around that capacity. Staff must also give clear no-shower rules and activity limits at placement, because weak instructions can ruin the test and trigger complaints.
Before opening, verify these inputs:
- Consult and reading slots match.
- Delayed reading coverage is assigned.
- Documentation happens the same day.
- Patient instructions use one script.
- Follow-up interpretation has an owner.
If the calendar cannot hold all three touchpoints, consult, placement, and read, the launch is not ready. The first-day risk is not demand; it is a workflow that cannot close the loop without delay.
4
Staffing And Protocols
Day-One Staff Readiness
For contact dermatitis patch testing, the launch gate is whether the first 2 Allergy Technicians and 1 Clinical Specialist can deliver the same placement, documentation, and escalation process every time. If technique varies, day-one reliability drops, patient flow slows, and provider confidence takes a hit.
The core setup includes provider interpretation workflow, photo or reaction documentation, adverse response escalation, and clear patient education scripts. That matters because patch testing is hands-on and timing-sensitive, so the service cannot open cleanly unless staff can explain restrictions, spot reactions, and hand off concerns without confusion.
Train Before First Placement
Use a written protocol and role-play each step before scheduling the first patient. One clean rule: if two staff members would do the same placement differently, keep training.
- Standardize patch application technique.
- Document photos the same way.
- Set escalation triggers in writing.
- Test patient scripts for no-shower rules.
- Verify provider sign-off on interpretation.
The staffing model should scale from 2 Allergy Technicians and 1 Clinical Specialist in Year 1 to 6 Allergy Technicians and 5 Clinical Specialists by Year 5, so the launch process should already be built for handoffs, supervision, and repeatable flow. If training is rushed, the clinic may open on paper but still miss safe first-day capacity.
5
Referrals And Demand Creation
Referral Pipeline
Patch testing opens on time only if the referral pipe is live on day one. The launch gate is active outreach to dermatology, allergy, primary care, occupational medicine, employer health, and self-pay search channels, because empty schedules waste clinical capacity and slow cash coming in.
Year 1 assumes physician referral outreach equals 25% of revenue and marketing plus website hosting runs $2,200 per month. If that work starts late, the clinic may be ready to test but still miss the modeled 242 treatments per month ramp.
Build demand before launch
Before opening, lock the source mix, outreach cadence, and who owns each channel. One clean rule: no referral engine, no realistic launch. Map contacts, scripts, website pages, search terms, and follow-up timing so the first patient requests can turn into booked visits fast.
- Assign channel owners before opening.
- Track referrals by source weekly.
- Launch search and website together.
- Prebook follow-up for every lead.
- Test messaging with nearby doctors.
What this plan hides: outreach takes time to compound, so early demand can lag even when clinical staffing is ready. If bookings stay thin, fixed spend like $2,200 per month still runs, and the team has to keep pushing physician and self-pay channels until volume closes the gap.
6
Related Products
- Contact Dermatitis Patch Testing Porter's Five Forces Analysis
- Contact Dermatitis Patch Testing BCG Matrix
- Contact Dermatitis Patch Testing Business Model Canvas
- What Are 5 KPIs For Contact Dermatitis Patch Testing Business?
- Contact Dermatitis Patch Testing Business Plan Template in Pre-Written Word
- How Increase Profits From Contact Dermatitis Patch Testing?
- How Increase Contact Dermatitis Patch Testing Profitability?
- Contact Dermatitis Patch Testing Startup Costs: $808k Funding Plan
- Contact Dermatitis Patch Testing Financial Model Template in Excel
- Contact Dermatitis Patch Testing Owner Income: $398K Year 1
- How To Write A Business Plan For Contact Dermatitis Patch Testing?
- Contact Dermatitis Patch Testing Marketing Mix
- Contact Dermatitis Patch Testing Marketing Plan
- Contact Dermatitis Patch Testing Business Proposal
- Contact Dermatitis Patch Testing PESTEL Analysis
- Contact Dermatitis Pitch Deck Example Editable PPTX
- Contact Dermatitis Patch Testing Business SWOT Analysis
- Contact Dermatitis Patch Testing Value Proposition Canvas
Frequently Asked Questions
Start with licensed clinical authority, not marketing Confirm provider licensure, supervising structure, malpractice coverage, state medical compliance, allergen vendor accounts, electronic health record templates, and Current Procedural Terminology code 95044 billing setup The researched launch plan assumes an 8 to 16 week opening window and Year 1 staffing that includes 1 Senior Dermatologist, 1 Physician Assistant, and 2 Allergy Technicians