 Owner income$398K-$678K
Owner income$398K-$678KContact Dermatitis Patch Testing Owner Income: $398K Year 1

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$398K-$678K  Net margin39%
Net margin39% Revenue for target pay$1.48M
Revenue for target pay$1.48M Business difficultyHard
Business difficultyHard


A contact dermatitis patch testing owner can make about $398K in first-year pre-tax operating profit under the researched assumptions, before reserves, taxes, debt service, and any final owner draw policy That case assumes about 242 completed tests per month, or roughly 56 per week, with average collected revenue of about $511 per completed test Direct testing, billing, and referral costs equal 225% of revenue, leaving a 775% contribution margin If the owner also fills the Medical Director role, the model separately includes a $280K annual wage, but that is working compensation, not passive profit
Owner income$398K-$678KNet margin39%Revenue for target pay$1.48MBusiness difficultyHardWant to test your own owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from monthly revenue, gross margin, labor, fixed overhead, marketing, reserves, and target owner pay.
Planning note: Research-based planning estimate only. Actual owner income depends on collections, staffing, payer mix, taxes, debt, and reinvestment. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to see the owner income forecast?
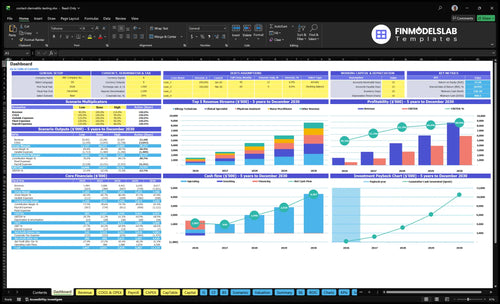
Open the Contact Dermatitis Patch Testing Financial Model Template for tabs on provider counts, capacity, pricing, costs, payroll, and owner income; it also shows charts for monthly revenue, contribution margin, EBITDA-like profit, and annual scenarios. Year 1 revenue is $148M, with 775% contribution margin, $21.8k monthly overhead, $491k annual wages, and $398k operating profit.
Income forecast highlights
- Owner income: $398k profit
- Revenue and margin: $148M, 775%
- Scenarios: annual take-home
What affects patch testing profit margin?
For Contact Dermatitis Patch Testing, margin is driven first by how steady test volume is, because the direct test economics improve when kits, panels, and referrals keep moving. If you also need the cost base, What Is The Monthly Operating Cost For Your Business? Please Provide The Business Name. In the model, Year 1 allergen kits and panels run at 120% of revenue, disposal and consumables at 30%, billing at 50%, and referral outreach at 25%; direct and variable costs then fall to 181% by Year 5, while margin gets hit when broader panels, staff time, denied claims, or repeat visits use more labor and supplies.
Cost drivers
- 120% Year 1 kits and panels
- 30% disposal and consumables
- 50% billing cost pressure
- 25% referral outreach spend
Margin leaks
- Broader panels add supply cost
- Staff time raises labor load
- Denied claims slow cash
- Repeat visits use more supplies
How much revenue does a patch testing clinic make per patient?
A Contact Dermatitis Patch Testing clinic makes about $511 in collected revenue per completed test in Year 1, based on $123,700 monthly revenue across 242 completed tests. That is collected revenue, not gross billed charges, and the real payment can move with payer, geography, coding, documentation, and contract terms. Provider-level Year 1 pricing runs from $350 at Allergy Technician capacity to $850 at Senior Dermatologist capacity, and follow-up revenue should be modeled separately because the source assumptions do not isolate it.
Base case math
- $123,700 monthly revenue
- 242 completed tests
- $511 per completed test
- Follow-up revenue is separate
Price range by provider
- $350 Allergy Technician capacity
- $850 Senior Dermatologist capacity
- Reimbursement varies by payer
- Contract terms change cash collected
How many patch tests per week does a contact dermatitis testing business need?
Contact Dermatitis Patch Testing needs about 37 completed patch tests per week to break even in the Year 1 case; the base model runs at 56 completed tests per week, leaving only a 19-test weekly cushion. For margin tactics tied to this service line, see How Increase Profits From Contact Dermatitis Patch Testing?.
Break-even math
- $62,717 monthly overhead and wages
- $511 average revenue per test
- 77.5% contribution margin
- 158 tests/month, about 37/week
Volume cushion
- Base model: 56 tests/week
- Cushion: 19 tests/week
- Risk: no-shows and referral gaps
- Control schedule and referral flow
Want the six income drivers?
1
56-295/wkTest Volume
More completed tests spread fixed clinic costs over more revenue, so this is the fastest path to higher owner take-home.
2
$511-$562Revenue/Test
A higher collected price lifts revenue on every test, and that gain drops straight into gross margin if costs stay flat.
3
MixCollections Mix
The model uses collected pricing with no payer split, so real cash can move fast if collection rates slip or improve.
4
$491K-$907KLabor Load
Clinical wages are a big earnings drag, so staffing mix and hours decide how much revenue reaches the owner.
5
150%-122%Supply COGS
Testing kits and consumables are cost of goods sold (COGS), and tighter panel use keeps more margin on each test.
6
$21.8K/moOverhead Spread
Clinic rent, insurance, software, and admin costs are fixed, so higher volume later makes each test more profitable.
Contact Dermatitis Patch Testing Core Six Income Drivers
Completed patch tests per week
Completed patch tests per week
Completed patch tests per week is the main income lever because fixed costs stay in place even when volume dips. The Year 1 model completes 242 tests per month, or about 56 per week, and break-even is about 37 per week under Year 1 assumptions. Above that line, each extra completed test helps pay overhead and owner draw.
The inputs are referral flow, booked slots, show rate, multi-visit timing, and provider capacity. By Year 5, volume reaches 1,279 tests per month, or about 295 per week. What this estimate hides: no-shows, scheduling gaps, referral softness, and staffing limits can make booked demand look fine while collected revenue lags.
Track completions, not just bookings
Measure scheduled, arrived, completed, and billed tests each week. If completions slip under 37 per week, the model is below break-even and owner income gets squeezed fast. Use reminders, tighter referral handoffs, and block scheduling so open slots do not sit empty.
Watch completion rate by provider day, not just monthly totals. The goal is simple: turn booked patients into completed, collected tests. A weekly dashboard for referrals, no-shows, and collected revenue per test shows whether extra volume is creating cash or just more admin work.
1
Patch testing revenue per completed test
Collected revenue per completed test
For this service, the cash engine is collected revenue per completed test, not billed charges. Year 1 is about $511 per completed test, with provider price assumptions from $350 to $850; by Year 5, the range rises to $390 to $950. At 77.5% contribution, a $511 test produces about $396 before rent and payroll, so better collections lift owner pay fast.
Track cash, not sticker price
Use three inputs: completed tests, collected revenue per test, and follow-up billing success. Gross charges do not pay the bills; collected revenue does. If payer contracts, documentation, or claim follow-up slip, the same volume can produce less cash and less profit. A clean monthly check is collected revenue ÷ completed tests, then compare it with the $511 Year 1 benchmark.
2
Patch testing payer mix
Patch Testing Payer Mix
Payer mix changes cash timing, denial risk, and realized revenue even when test volume stays flat. The model gives collected pricing assumptions, but it does not give a commercial, Medicare, or cash-pay split, so the collection rate should be an editable field. No reimbursement amount is guaranteed, so booked revenue can overstate take-home cash.
Here’s the quick math: if billing and claims processing runs at 50% of revenue in Year 1 and 42% in Year 5, weak execution can turn a full schedule into slow or unpaid cash. That hits the owner twice: lower profit and delayed draw capacity. This is a revenue-quality problem, not just a billing problem.
Track Collections, Not Just Charges
Set one collection rate for each payer bucket and update it monthly. Watch collected revenue, denial rate, days in accounts receivable, and write-offs; those four lines tell you if the payer mix is helping or hurting cash. If commercial or Medicare payments slow, owner pay should follow cash, not booked charges.
Build the forecast from actual remits and denials, then compare it to the 50% and 42% billing cost benchmarks. If claims lag or documentation is thin, tighten coding, appeal flow, and patient payment rules before adding more test volume.
3
Patch testing staffing costs
Patch Testing Labor Cost Load
Labor decides whether margin becomes owner income or payroll. Year 1 listed wages total $491K: $280K Medical Director, $85K Practice Manager, $52K Patient Coordinator, $29K Billing Specialist FTE, and $45K Medical Assistant. By Year 5, wages rise to $907K, so staffing has to support more completed tests and collected cash, not just more people.
If the owner fills the Medical Director role, that $280K is working pay, not passive profit. The pressure points are supervision load, schedule gaps, and underused clinical staff; if test volume stalls, payroll drains cash fast and owner draw gets squeezed.
Track Payroll per Completed Test
Build the model from FTE count, salary, and completed tests. A simple check is total wages ÷ completed patch tests; then compare it each month as volume changes. If tests rise but payroll stays flat, owner income improves. If staff time grows faster than tests, margin leaks into idle labor.
- Track wages by role monthly
- Match staffing to booked tests
- Watch no-shows and open slots
Keep the Medical Director, coordinator, and billing load tied to booked and collected volume. One clean rule: no added FTE without enough tests to cover the salary and supervision drag.
4
Contact dermatitis patch testing supply costs
Supply Cost per Patch Test
Every completed test eats materials, so this driver can swing owner pay fast. In Year 1, COGS = 150% of revenue: 120% for allergen kits and panels plus 30% for disposal and consumables. At a $511 collected test, supply cost is $766.50 per patient, so gross margin is negative before labor and overhead.
By Year 5, COGS improves to 122%, but it still stays tied to volume and panel cost. If revenue per test rises or waste falls, more cash reaches owner pay; if kit prices or disposables jump, margin shrinks even when test count holds steady.
Track Cost per Completed Test
Measure kit cost, disposables, waste, and completed tests each month. Here’s the quick math: supply COGS ÷ collected revenue. Use it to test how panel mix, vendor price changes, or re-tests affect cash and profit per patient, not just total sales.
Keep a per-patient sheet by payer and panel type. If supply cost stays above collected revenue, owner income gets squeezed before rent and wages even hit. That’s the number to watch when setting prices, buying inventory, and planning how much profit the owner can safely draw.
5
Patch testing clinic overhead
Fixe d Overhead per Test
Fixed overhead is $21,800 per month in the source model, made up of $12,500 rent, $3,200 malpractice insurance, $1,800 for EHR and practice management software, $1,500 for utilities and maintenance, $600 for office supplies, and $2,200 for marketing and website hosting. This cost base sits under every test, so it hits owner income even when volume is soft.
Here’s the quick math: at 242 tests per month, overhead is about $90 per test ($21,800 / 242). At 1,279 tests per month, it falls to about $17 per test. That spread is why volume matters so much: more completed tests push more revenue over the same fixed base and leave more room for owner pay. Local rent, insurance, and admin needs can change the result.
Track Overhead Against Completed Tests
Measure overhead in cost per completed test, not just total spend. Track monthly tests, rent, insurance, software, admin hours, and marketing, then divide fixed overhead by completed volume. If tests slip, the same $21,800 gets spread across fewer cases, and profit drops fast. One clean rule: if volume falls, owner draw should not be set from gross revenue alone.
Watch the two biggest levers first: rent and staffing/admin load. If a lease or insurance quote pushes fixed costs up, you need more completed tests just to hold the same margin. Build forecasts at both 242 and 1,279 tests per month so you can see how much cash remains for wages, tax, debt service, and the owner’s take-home pay.
6
Compare low, base, and high owner income scenarios
Owner income scenarios
Owner income rises with test volume, provider mix, and staffing. More tests boost revenue, but wages and fixed clinic costs keep the low, base, and high cases far apart.
| Scenario | Low CaseLean | Base CaseScaled | High CaseMulti-provider |
|---|---|---|---|
| Launch model | This is the lean earnings path with Year 1 volume and smaller owner income. | This is the modeled middle case with Year 2 volume and steady staffing. | This is the stronger earnings path with Year 5 volume and a multi-provider setup. |
| Typical setup | It models 56 tests a week, about $511 revenue per test, 77.5% contribution margin, $491K wages, $21.8K monthly fixed overhead, and about $398K pre-tax operating profit. | It tracks 102 tests a week, about $509 revenue per test, 78.6% contribution margin, $617K wages, $2.69M revenue, and about $1.23M pre-tax operating profit. | It models 295 tests a week, about $562 revenue per test, 81.9% contribution margin, $907K wages, $8.62M revenue, and about $5.89M pre-tax operating profit. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $398KLean profit | $1.23MModeled profit | $5.89MUpside profit |
| Best fit | Use this to test launch staffing, referral flow, and cash buffer needs. | Use this as the working plan for normal ramp and staffing. | Use this to test what happens if multiple clinicians stay full and referrals hold. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Contact Dermatitis Patch Testing Porter's Five Forces Analysis
- Contact Dermatitis Patch Testing BCG Matrix
- Contact Dermatitis Patch Testing Business Model Canvas
- What Are 5 KPIs For Contact Dermatitis Patch Testing Business?
- Contact Dermatitis Patch Testing Business Plan Template in Pre-Written Word
- How Increase Profits From Contact Dermatitis Patch Testing?
- How Increase Contact Dermatitis Patch Testing Profitability?
- Contact Dermatitis Patch Testing Startup Costs: $808k Funding Plan
- Contact Dermatitis Patch Testing Financial Model Template in Excel
- How To Open Contact Dermatitis Patch Testing In 8–16 Weeks
- How To Write A Business Plan For Contact Dermatitis Patch Testing?
- Contact Dermatitis Patch Testing Marketing Mix
- Contact Dermatitis Patch Testing Marketing Plan
- Contact Dermatitis Patch Testing Business Proposal
- Contact Dermatitis Patch Testing PESTEL Analysis
- Contact Dermatitis Pitch Deck Example Editable PPTX
- Contact Dermatitis Patch Testing Business SWOT Analysis
- Contact Dermatitis Patch Testing Value Proposition Canvas
Frequently Asked Questions
The researched first-year case shows about $398K in pre-tax operating profit after listed wages, before reserves, taxes, debt, and final owner draw choices That assumes $148M revenue, 242 completed tests per month, and a 775% contribution margin If the owner also works as Medical Director, the model separately includes $280K of working compensation