 Owner income$2.7M–$13.5M
Owner income$2.7M–$13.5MHow Much Cosmetic Surgery Center Owners Can Make on $39M-$169M

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$2.7M–$13.5M  Net margin61.1%–81.1%
Net margin61.1%–81.1% Revenue for target pay$3.9M
Revenue for target pay$3.9M Business difficultyHard
Business difficultyHard


A cosmetic surgery center owner’s income is the cash left after operating costs, surgeon/provider economics, debt service, reserves, and reinvestment In the provided model, revenue rises from $3924M in Year 1 to $16912M in Year 5, with known variable costs falling from 180% to 140% Before unspecified provider compensation, debt service, reserves, and owner taxes, the model shows EBITDA-like operating profit of about $24M to $137M Treat that as a planning ceiling, not guaranteed cosmetic surgery center owner earnings
Owner income$2.7M–$13.5MNet margin61.1%–81.1%Revenue for target pay$3.9MBusiness difficultyHardWant to test your owner income case?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income depends on revenue, costs, debt, reserves, taxes, and execution.
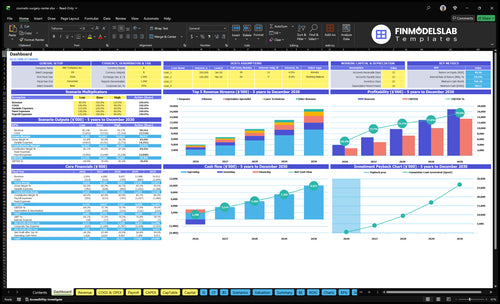
Can you check owner income in the Cosmetic Surgery Center financial model?
This dashboard shows revenue, margins, costs, reserves, and owner take-home assumptions in the Cosmetic Surgery Center Financial Model Template; open it.
Owner-income model highlights
- Owner take-home view
- Revenue and margin build
- Scenario-based assumptions
What cosmetic surgery center operating costs reduce owner take-home most?
Owner take-home gets squeezed most by surgeon compensation, clinical payroll, operating-room support, and the cost stack behind each case: supplies, implants, pharmaceuticals, anesthesia, labs, insurance, rent, marketing, equipment financing, and compliance. If you’re mapping the fixed load, What Is The Estimated Cost To Open A Cosmetic Surgery Center? puts the backdrop at $56k/month in fixed overhead, including a $25k lease and $15k malpractice insurance.
Biggest variable drags
- Medical supplies and implants: 50%–60%
- Pharmaceuticals: 15%–20%
- External anesthesia and lab fees: 25%–30%
- Marketing: 50%–70%
Heavy fixed monthly load
- Lease: $25k/month
- Malpractice insurance: $15k/month
- Total fixed overhead: $56k/month
- Equipment financing and compliance add more pressure
How much revenue does a cosmetic surgery center need for owner pay?
For a Cosmetic Surgery Center, break-even is not the same as owner pay. Revenue has to cover known variable costs, $56k/month fixed overhead, a $150k director salary, provider compensation, financing, reserves, and reinvestment; the clean formula is required revenue = (target owner pay + fixed costs + debt + reserves + reinvestment) / contribution margin after provider pay. The model’s revenue path rises from $3.924M in Year 1 to $9.657M in Year 3 and $16.912M in Year 5, while monthly surgeon case volume moves from 12 to 45, so volume and case mix drive the gap.
Break-even floor
- Covers variable costs first
- Add $56k monthly overhead
- Include provider compensation
- Owner pay sits above break-even
Volume gap
- Cases move from 12 to 45
- Year 1 revenue: $3.924M
- Year 3 revenue: $9.657M
- Year 5 revenue: $16.912M
How does owner involvement change cosmetic surgery center income?
Owner involvement changes income at the Cosmetic Surgery Center a lot. An owner-surgeon can earn clinical compensation plus distributions, a management owner can earn management pay plus distributions, and an investor-style owner may rely mostly on distributions. With 2 surgeons in Year 1 and 6 in Year 5, more profit can shift to hired surgeons, so owner income before taxes depends on the pay model, cash reserves, debt, and whether the owner’s labor is already paid through payroll.
Owner pay types
- Owner-surgeon gets clinical pay plus distributions
- Management owner gets management pay plus distributions
- Investor-style owner depends mostly on distributions
- Payroll can already cover owner labor
What changes the split
- Year 1 starts with 2 surgeons
- Year 5 grows to 6 surgeons
- Hired surgeons change profit share
- Cash reserves and debt affect take-home pay
Want the six income drivers in one view?
1
12-45/moCase Volume
More monthly surgical cases spread the same room, nurse, and admin base across more revenue, so owner cash climbs fast.
2
$15K-$17.5KCase Price
A higher collected surgeon fee boosts revenue without much extra overhead, so each case leaves more cash for the owner.
3
HighProvider Mix
If the owner performs cases, more margin stays inside the center; hired or contracted surgeons take a bigger cut first.
4
$56K/moOverhead
With about $56K a month in fixed costs and a $150K director salary, empty slots drain cash fast, while fuller schedules improve take-home.
5
7%-5%Acquisition
Marketing & patient acquisition drops from 7.0% to 5.0% of revenue, so better conversion leaves more profit after each booked case.
6
RequiredDebt Reserve
Debt payments and reserve funding come before distributions, so operating profit is not the same as owner income.
Cosmetic Surgery Center Core Six Income Drivers
Monthly surgical case volume and utilization
Monthly surgical case volume
This driver is how many qualified surgical cases the center actually completes each month. The source model shows 12 surgeon cases/month in Year 1, 28 in Year 3, and 45 in Year 5, with 2 surgeons in Year 1, 6 in Year 5, and capacity moving from 600% to 750%. More filled cases spread fixed overhead like the $56k/month base across more revenue, so owner pay rises only when cases stay qualified.
Utilization means how much of the usable schedule turns into billed cases. The inputs are surgeon count, cases per surgeon, consultation conversion, show rate, cancellations, staffing, and safe room capacity. If any of those slip, the ceiling drops fast. Do not chase volume if standards or recovery safety weaken; weak staffing can cut profit faster than one extra open day helps.
Track fill before adding cases
Track booked cases, completed cases, and lost slots by reason. Here’s the quick math: every extra qualified case helps cover fixed costs, while every unused block leaves the same bills in place. Watch the weekly fill rate by surgeon and room, plus consult-to-case conversion, because those are the earliest signs that monthly income will miss plan.
Set a hard gate before adding volume: enough staff, enough block time, and enough safe room capacity. Use 12, 28, and 45 cases/month as planning checkpoints from Year 1, Year 3, and Year 5, but only if the center can staff and stage those cases safely without overtime or rushed turnovers.
1
Average collected revenue per case and procedure mix
Average Collected Revenue per Case
This driver is the net cash collected per case after discounts, financing fees, refunds, and cancellations. It matters because each operating slot still has to cover staff, rent, insurance, and financing, so a low-collected case can wipe out margin fast. The disclosed surgeon collected fee rises from $15,000 in Year 1 to $17,500 in Year 5, so mix and price discipline directly lift owner pay.
Here’s the quick math: higher-ticket surgical cases like facelifts, body contouring, breast procedures, liposuction, and combined cases carry more revenue per slot than injectables at $800-$950 or laser at $500-$600. If collections slip, the owner still pays the same fixed costs, so profit and cash flow fall even when booked volume looks strong.
Track Collected Case Yield
Measure collected revenue per completed case, not posted price. Break it out by procedure type, financing approval rate, refund rate, and cancellation rate so you can see which mix actually pays. A simple dashboard should show surgical cases, injectables, laser, and combined cases, plus the gap between billed and collected dollars. That gap is what hits owner income.
- Track net collected per procedure.
- Split by surgeon and case type.
- Watch discounts and financing fees.
- Cut cancellations before day-of surgery.
Use the data to steer mix toward higher-collected cases when capacity is tight. If a lower-ticket service fills the calendar but leaves little after fees, it can crowd out better-margin surgical work. The owner’s take-home improves when each slot clears enough cash to cover fixed overhead and still leave surplus for draw.
2
Surgeon and provider compensation economics
Provider pay structure
This driver matters because the center uses revenue-producing surgeons, anesthesiologists, nurses, injectable specialists, and laser techs, but the pay schedule is not disclosed. If provider pay is a variable share, margin changes on every case. If pay is fixed, then utilization and schedule fill rate decide whether the owner keeps enough spread after labor.
At 12 cases per month in Year 1 and 45 cases per month by Year 5, the owner’s take-home can swing fast. With collected revenue per surgeon case rising from $15,000 to $17,500, the key question is how much of each case stays after provider pay, because that is what funds overhead and owner draw.
Model pay per case
Build the forecast around collected revenue per case, provider pay method, and case volume. Track the spread after anesthesia, nursing, and tech labor, then test whether the owner earns more from a fixed salary model or a revenue-share model. The simple rule is: more cases help only if each case still leaves contribution.
- Track pay by provider and case.
- Separate fixed from variable labor.
- Watch contribution per surgical slot.
- Stress-test low-utilization months.
What this estimate hides: if provider pay rises with every added case, a full calendar can still disappoint the owner. If pay is fixed, weak utilization leaves more labor and overhead uncovered, so the monthly schedule must stay tight and the case mix must stay profitable.
3
Fixed overhead and facility cost leverage
Fixed Overhead Leverage
Fixed costs hit owner pay hard here because they stay on even when cases slow down. The disclosed base includes $56k/month before provider compensation and financing, plus a $150k Center Director salary a year, so weak utilization quickly squeezes operating profit and cash available for distributions.
The named monthly items include $25k lease, $15k malpractice insurance, $35k utilities, $2k software and EMR, $4k cleaning, $25k security, $1k general liability, and $3k professional fees. Empty capacity still carries the same bill load, so every light month pushes the owner’s take-home lower.
Track the Fixed Base, Not Just Revenue
Measure fixed overhead per booked case each month: total fixed cost divided by completed cases. Use the same view for consultation volume, because fewer surgeries mean each case must absorb more rent, insurance, and payroll. Here’s the quick math: if fixed load rises and case count falls, owner margin shrinks even when pricing holds.
- Reconcile the true monthly fixed base.
- Track cases booked vs. staffed capacity.
- Watch utilization before adding payroll.
- Test whether director time is underused.
What this estimate hides: the disclosed figures show both a $56k/month overhead base and line items that add more cost, so the owner should confirm which costs are already included before forecasting draw. The goal is simple: spread fixed bills over more completed procedures without forcing unsafe volume.
4
Patient acquisition, consultation conversion, and reputation
Qualified consult flow
For a cosmetic surgery center, patient acquisition only helps if it turns into booked surgical consults. The model says marketing and acquisition cost falls from 70% of revenue in Year 1 to 50% in Year 5, which is about $275k/year in Year 1 and $846k/year in Year 5. If spend brings in weak leads, owner pay gets squeezed fast.
The key inputs are lead quality, consult show rate, financing approvals, reviews, referrals, and consult-to-case conversion. Better reputation lifts each step, so the center fills capacity without buying extra traffic. One clean rule: more qualified consults, less wasted ad spend.
Track conversion, not just clicks
Measure the path from lead to consult to surgery. If consult show rates or financing approvals slip, acquisition cost rises as a share of revenue and cash available for owner draw falls. Track cost per qualified consult, case conversion rate, and review volume together, not in isolation.
Set weekly checks on source mix, no-show rate, and referral share. The goal is simple: spend only where the center can convert interest into paid procedures. Filled consult slots protect margin; empty slots turn ad dollars into overhead.
5
Debt service, reserves, and reinvestment
Debt service and cash reserves
Profit is not the same as take-home pay here. With $56k/month in fixed overhead and $15k/month in malpractice insurance, cash has to cover debt service, refunds, cancellations, equipment, hiring, compliance, and growth before the owner can draw anything.
This driver includes loan payments, reserve set-asides, and reinvestment budgets. To estimate owner income, you need monthly principal and interest, any working capital reserve rate, refund reserve, and planned capital spending. If those are missing, operating profit will overstate distributable cash.
Hold cash before draws
Track cash after debt service, not just operating margin. A clinic can look profitable and still pay the owner little if premiums, equipment needs, or compliance spend come due in the same month. Distributions should come only after business operating needs are funded.
- Forecast debt service monthly
- Set reserve targets first
- Protect cash for refunds
- Fund equipment replacements
- Delay draws when cash is tight
6
Compare low, base, and high owner income scenarios without treating them as guarantees
Owner income scenarios
Owner income changes with case volume, revenue mix, and cost load. Provider pay is not shown here, so these are operating profit ceilings, not promised take-home.
| Scenario | Low CaseAssumption-based | Base CaseProvider pay missing | High CaseUpside only |
|---|---|---|---|
| Launch model | This is the lower-earnings path built on Year 1 ramp. | This is the modeled middle path using Year 3 performance. | This is the stronger earnings path built on Year 5 volume. |
| Typical setup | Year 1 uses 12 surgeon cases a month, $3.924M revenue, 180% known variable costs, and about $2.396M operating profit before provider pay, debt, reserves, and taxes. | Year 3 uses 28 surgeon cases a month, $9.657M revenue, 161% known variable costs, and about $7.280M operating profit before provider pay, debt, reserves, and taxes. | Year 5 uses 45 surgeon cases a month, $16.912M revenue, 140% known variable costs, and about $13.722M operating profit before provider pay, debt, reserves, and taxes. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $2.4MNot guaranteed | $7.3MReserves required | $13.7MNot guaranteed |
| Best fit | Use this to stress-test a slower ramp and heavy cost load. | Use this as the core planning case for budgeting and hiring. | Use this to test upside if volume and pricing hold. |
Planning note: These ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. Provider compensation is missing, reserves are still required, and results are not guaranteed.
Related Products
- Cosmetic Surgery Center Porter's Five Forces Analysis
- Cosmetic Surgery Center BCG Matrix
- Cosmetic Surgery Center Business Model Canvas
- 7 Critical KPIs for a Cosmetic Surgery Center
- Cosmetic Surgery Center Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Cosmetic Surgery Center Profitability
- Analyzing the Running Costs of a Cosmetic Surgery Center
- Cosmetic Surgery Center Startup Costs With $92K Opening-Month Overhead
- Cosmetic Surgery Center Financial Model Template in Excel
- How To Open A Cosmetic Surgery Center In 9–18 Months
- How to Write a Business Plan for a Cosmetic Surgery Center
- Cosmetic Surgery Center Marketing Mix
- Cosmetic Surgery Center Marketing Plan
- Cosmetic Surgery Center Business Proposal
- Cosmetic Surgery Center PESTEL Analysis
- Cosmetic Surgery Center Pitch Deck Example Editable PPTX
- Cosmetic Surgery Center Business SWOT Analysis
- Cosmetic Surgery Center Value Proposition Canvas
Frequently Asked Questions
Owner income depends on what remains after provider pay, debt, reserves, and reinvestment The provided model shows revenue from $3924M to $16912M and known operating profit before unspecified provider compensation from about $24M to $137M Treat that as a planning ceiling, not guaranteed take-home pay