 Time to Open3-6 monthsLaunch runway
Time to Open3-6 monthsLaunch runwayHow to Open a Dental Sleep Medicine Practice in 3 to 6 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open3-6 monthsLaunch runway  Launch Sequence6 stagesTraining first
Launch Sequence6 stagesTraining first Key BottleneckBilling flowClaims and referrals
Key BottleneckBilling flowClaims and referrals First Revenue StepCase startsScreened patients
First Revenue StepCase startsScreened patients


Key Takeaways
- Train clinical workflows before pushing marketing volume.
- Build physician referral paths for steadier diagnosed patients.
- Lock billing and documentation to protect cash flow.
- Standardize lab and staff handoffs to start cases faster.
Time to Open3-6 monthsLaunch runwayLaunch Sequence6 stagesTraining firstKey BottleneckBilling flowClaims and referralsFirst Revenue StepCase startsScreened patientsLaunch timeline
This is the short web summary; the XLSX export contains the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Clinical setup
- Sleep training kickoff
- Consent forms draft
- Screening scripts set
- Clinical protocol final
- Chart templates ready
Vendors and equipment
- Scanner order
- Chair installation
- Sterilization setup
- Lab partner onboard
- Appliance kit stock
Billing and claims
- Payer enrollment
- Fee schedule build
- Claim templates test
- Benefits check flow
- Denial workflow set
Staffing and training
- Hire coordinator
- Hire assistant
- Front desk training
- Role drills
- Coverage schedule
Referral and marketing
- Physician list build
- Intro visits
- Referral packet ready
- Local pages live
- Outreach follow-up
Go-live and ops
- Internal screening start
- Consults scheduled
- First impressions
- Appliance starts
- Weekly review
Why test the launch plan before you commit?
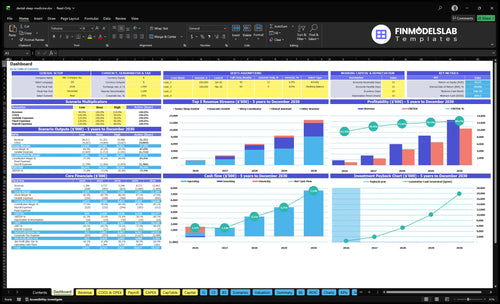
This model shows revenue, costs, runway, and breakeven logic; open the Dental Sleep Medicine Practice Financial Model Template.
Financial model highlights
- Launch timing and consults
- 40 treatments monthly
- 60% capacity ramp
- $4,500 treatment price
- $108k planned revenue
- $13.1k fixed overhead
- 225% Year 1 variable
- $65k billing salary
- Runway and breakeven path
- Reimbursement timing charts
How long does it take to start a dental sleep medicine practice?
A dental sleep medicine practice usually takes 3 to 6 months to launch if it’s added onto an existing office; a standalone practice takes longer. The real clock starts when medical billing, physician referral ties, team training, appliance vendor onboarding, scheduling, payer documentation, and local marketing are ready. Launch month should not start until consult, lab, delivery, adjustment, and follow-up workflows are rehearsed.
What speeds launch
- Use an existing office setup
- Automate billing from day one
- Train the team early
- Lock in vendor onboarding fast
What causes delays
- Manual benefits checks slow intake
- Unclear diagnosis paths stall starts
- Weak referral links cut volume
- Unpracticed workflows delay launch
What do you need to start a dental sleep medicine practice?
To start a Dental Sleep Medicine Practice, you need an active dentist license, sleep medicine training, oral appliance therapy protocols, physician diagnosis coordination, lab workflow, patient records, informed consent, medical billing, and trained staff; How Increase Dental Sleep Medicine Practice Profits? covers the profit side after launch. Certification can help credibility, but don’t treat it as a universal legal requirement.
Launch basics
- Hold an active dentist license
- Set oral appliance therapy protocols
- Coordinate physician diagnosis and referrals
- Build appliance lab and records workflows
Year 1 team
- 1 senior sleep dentist
- 1 sleep coordinator
- 1 clinical assistant and 1 hygienist
- 1 medical billing manager
What launch mistakes hurt a dental sleep medicine practice?
If a Dental Sleep Medicine Practice opens before the medical billing workflow is ready, or bets only on physician referrals, it can stall cash and patient starts fast. The Year 1 model is already tight with 120% lab fees, 30% supplies, 40% billing, and 35% outreach, so one weak step can hurt both acceptance and cash flow. Here’s the quick fix: run readiness checks, test consult scripts, confirm payer documents, and track screened patients to appliance starts.
Big launch risks
- Open before billing is ready
- Rely only on physician referrals
- Undertrain front desk and hygiene teams
- Use weak documentation and follow-up
What to tighten first
- Test consult scripts before launch
- Confirm payer documents early
- Clarify the appliance lab process
- Track screened patients to starts
Confirm the practice is ready before accepting sleep apnea and snoring patients
Launch readiness checklist
Use this go-live approval checklist to confirm the practice is ready before opening.
Compliance
- Active dental licenseCritical
No launch until the treating dentist can legally practice in the state.
- State scope reviewedCritical
Sleep apnea and snoring care must fit state dental scope.
- Informed consent packet readyHigh
Patients need clear consent before oral appliance therapy starts.
- Documentation standards setHigh
Good notes support care, billing, and audit defense.
- Privacy workflow testedHigh
Protected health data must move safely from consult to follow-up.
Care flow
- Screening forms readyHigh
Screening has to sort likely cases before the first visit.
- Consult template loadedHigh
A fixed consult flow keeps diagnosis and benefits checks consistent.
- Benefits check script readyHigh
If payer documents are unclear, case starts slow down fast.
- Records capture worksHigh
The team needs a clean record path from intake to follow-up.
- Follow-up protocol approvedHigh
Titration and follow-up visits must be set before launch.
Lab setup
- Lab contract signedCritical
Appliance output depends on one confirmed oral appliance lab.
- Scanner or impression process readyCritical
Cases stall if the scan or impression path is not stable.
- Supplies stocked for launchHigh
You need enough kits and materials for the first case wave.
- Maintenance contracts activeMedium
Broken scanners or chairs can stop revenue in the first month.
Staffing
- Core clinical team hiredCritical
Year 1 needs the senior sleep dentist, coordinator, assistant, and hygienist.
- Medical billing manager assignedHigh
Billing work must be owned before claims and payer follow-up start.
- Team training completedHigh
Staff must know intake, consent, appliance flow, and escalation.
- Coverage schedule setMedium
Opening coverage should match the expected case load.
Demand
- Hygiene screening activeHigh
Hygiene visits should feed the first case-start funnel.
- Physician materials readyHigh
Primary care and sleep partners need a clear referral path.
- Sleep lab outreach queuedMedium
Outreach helps fill the schedule while search demand ramps.
- Local SEO liveMedium
Local search must support early patient discovery near launch.
Finance
- Cash runway covers launchCritical
Minimum cash is $854k at Month 2, so launch needs deep runway.
- Overhead model ties outCritical
Monthly fixed overhead is $13.1k before the billing manager salary.
- Go-live signoff completeCritical
Ready means diagnosis path, benefits checks, lab flow, and follow-up all work.
Which launch drivers decide whether early cases happen?
1Clinical Training
Protocol gateWritten oral appliance protocols cut inconsistent handling and keep first starts moving.
2Referral Path
ReferralsA clear diagnosis and referral flow steadies consults beyond internal screening.
3Billing Setup
40% + $65KBenefits checks and claim ownership protect cash and reduce lost starts after consults.
4Lab Workflow
120% / 30%Confirmed lab steps and records keep appliance delivery and adjustments from stalling.
5Team Training
1+1+1 staffOne coordinator, assistant, and hygienist need scripts so patients book instead of walking out.
6Revenue Ramp
$108K/moForty treatments at 60% capacity and $4,500 price set the first-year revenue ramp.
Clinical Training And Protocols
Clinical Protocols Before Patient Volume
Open-day readiness here means the dentist and team can screen, collect records, choose the right appliance, fit it, titrate it, and set follow-up without guesswork. The written oral appliance therapy protocol is the gate: if the team cannot follow one process, consults stall and first starts get messy.
This driver affects launch timing because clinical workflow comes before marketing volume. If handoffs, templates, and follow-up cadence are not set, every case becomes custom troubleshooting. On the plan’s math, 40 monthly treatments at $4,500 each implies $108,000 in monthly planned revenue, so even a few delayed starts can hit cash flow fast.
Write the Protocol Before the First Consult
Build and test the full workflow before opening: consult template, records checklist, appliance selection rules, fitting steps, titration schedule, follow-up timing, and physician handoff notes. The goal is simple: every patient should move through the same path, and every team member should know the next step.
- Train dentist and team together
- Document handoffs in writing
- Set follow-up cadence now
- Test one mock case end to end
If the team cannot run the process without coaching, launch volume should stay low until it can. That protects first-day experience and keeps the opening from turning into a series of stalled consults and redo visits.
1
Physician Referral And Diagnosis Pathway
Referral and Diagnosis Path
Without a live path for physician diagnosis and referral intake, the practice can’t reliably reach diagnosed patients on day one. This is the gate between internal screening and a compliant consult flow. If records exchange or follow-up notes are slow, cases stall, and marketing just creates more unfinished leads.
Medical diagnosis stays with the physician; the dental team handles oral appliance therapy. That line has to be clear in the intake packet, note templates, and case-status updates. Weak trust or vague documentation can delay starts, and the first weeks can feel empty even when demand is there.
Build the handoff before launch
Set the referral path before opening, not after consults start. The launch-ready version is simple: referral materials, sleep physician outreach, sleep lab education, communication templates, and a status tracker for each case. Test one full loop from diagnosis to records exchange to follow-up note before the first appointment lands.
- Separate diagnosis from treatment.
- Use one records checklist.
- Assign one case-status owner.
- Send note templates early.
- Track every referral source.
One clean handoff matters more than more marketing. If trust is weak or documentation is incomplete, first-day capacity looks smaller than planned because consults can’t move forward. That also pushes cash needs up, since staff, systems, and outreach still run while cases wait.
2
Medical Billing And Documentation
Medical Billing Readiness
No clean claim flow, no clean launch. In a dental sleep practice, benefits verification, payer documentation, and claim handoff decide whether the first consult turns into cash or into delay. If coverage is unclear or the team cannot explain the billing next step, patients can hesitate and case starts can stall right after diagnosis.
The cost load is real: Year 1 planning includes 40% for medical billing and claims processing, plus a $65,000 annual medical billing manager salary. That makes billing setup a launch dependency, not a later admin task. The bottleneck risk is delayed claims or confused patients, which can slow reimbursement and squeeze opening cash.
Set the Claim Path First
Before opening, set billing roles, test forms, and map diagnosis and treatment records to the payer documentation checklist. Track reimbursement timing from the first live cases, so you know how long cash takes to come back. One owner, one checklist, and one workflow beat ad hoc follow-up.
- Assign one billing owner.
- Verify benefits before visits.
- Test claim forms with sample charts.
- Match records to payer needs.
- Track denials, resubmits, and payment lag.
3
Appliance Lab And Clinical Workflow
Appliance Lab Workflow
This launch driver matters because the practice cannot start cases on time unless the lab partner, scan or impression method, and delivery visit plan are locked before opening. If records are incomplete or the appliance workflow is vague, first cases stall, delivery dates slip, and day-one capacity drops.
The readiness signal is a documented path from consult to appliance start: confirmed records process, adjustment process, and follow-up scheduling. The cash side is real too, with disclosed Year 1 pressure from 120% custom oral appliance lab fees and 30% supplies and impression materials, so remake delays can hit both timing and working capital.
Set the lab path before marketing
Before opening, confirm the vendor onboarding, supply setup, scanner or impression protocols, operatory flow, and maintenance plan. One clean rule: no marketing push until the first appliance case can move from records to delivery without guessing.
- Write the record checklist.
- Test scan or impression handoff.
- Define remake approval steps.
- Schedule delivery and adjustment visits.
- Assign who tracks follow-up tasks.
What this hides is delay risk from unclear records. If the lab has to remake appliances, the case timeline stretches, staff rework rises, and early revenue gets pushed out. Keep the process tight so the first consult can become a real appliance start, not a file waiting on fixes.
4
Team Training And Scheduling
Day-One Team Flow
If the team can’t explain the next step, day-one readiness breaks fast. In this practice, staff must screen, coordinate records, answer benefits questions, and get patients to a consult before they leave. The main risk is simple: patients are screened but no consult gets booked, so opening day feels busy but produces weak starts.
The readiness signal is a clear workflow with 1 sleep coordinator, 1 clinical assistant, 1 hygienist, and 1 medical billing manager. Each person needs a written role, a handoff point, and a recall task. When those steps are still in people’s heads, screening-to-consult conversion slips and first-revenue timing gets pushed back.
Pre-Open Rehearsal
Build the scripts before opening. Cover the call flow, hygiene handoff, billing handoff, and the exact words used to explain records, benefits, consult scheduling, and follow-up reminders. One clean script set lowers confusion and keeps staff from making up answers at the front desk.
- Assign one owner per handoff.
- Practice benefits questions.
- Book consults before checkout.
- Log recall reminders same day.
Test the workflow in order: screening, record request, consult booking, benefits check, and recall reminder. Use a short checklist so each handoff has an owner and a timestamp. If the team cannot run that sequence without help, the launch plan still needs rehearsal before the doors open.
5
Patient Acquisition And Revenue Ramp
Patient Ramp
For a dental sleep medicine practice, opening on time is not just about the office being ready. It’s about having a measurable funnel from screening to consult to appliance start so the first patients can move through the process on day one.
That ramp depends on hygiene screening, referral education, local SEO, educational consults, case-start conversion checks, and physician outreach. The Year 1 plan assumes 35% physician outreach and marketing plus $2,500 per month for marketing and SEO maintenance. The planning math is 40 monthly treatments × 60% capacity × $4,500 = $108,000 monthly planned revenue, but volume and reimbursement are not guaranteed.
Build the Funnel First
Before launch, map who owns each step: screening, consult booking, records, benefits checks, and appliance start. Tie every lead source to a count so you can see where cases stall. If consults rise but starts lag, the issue is usually handoff quality, not demand.
Test the full path with a small batch of patients before you spend heavily on outreach. Confirm that physician referrals, local search traffic, and hygiene leads all land in the same tracking sheet or system. One clean handoff is worth more than a lot of untracked inquiries.
6
Related Products
- Dental Sleep Medicine Practice Porter's Five Forces Analysis
- Dental Sleep Medicine Practice BCG Matrix
- Dental Sleep Medicine Practice Business Model Canvas
- What Are The 5 Core KPIs For Dental Sleep Medicine Practice Business?
- Dental Sleep Medicine Practice Business Plan Template in Pre-Written Word
- How Increase Dental Sleep Medicine Practice Profits?
- What Are Operating Costs For Dental Sleep Medicine Practice?
- Dental Sleep Medicine Practice Startup Costs: $190K CAPEX Plan
- Dental Sleep Medicine Practice Financial Model Template in Excel
- How Much a Dental Sleep Medicine Practice Owner Can Make at 24 Cases/Month
- How To Write A Business Plan For Dental Sleep Medicine Practice?
- Dental Sleep Medicine Practice Marketing Mix
- Dental Sleep Medicine Practice Marketing Plan
- Dental Sleep Medicine Practice Business Proposal
- Dental Sleep Medicine Practice PESTEL Analysis
- Dental Sleep Medicine Pitch Deck Example Editable PPTX
- Dental Sleep Medicine Practice Business SWOT Analysis
- Dental Sleep Medicine Practice Value Proposition Canvas
Frequently Asked Questions
Start by building the workflow before chasing volume You need sleep medicine training, oral appliance therapy protocols, physician diagnosis coordination, appliance lab setup, medical billing readiness, and staff scripts The researched Year 1 plan uses 1 senior sleep dentist, 1 sleep coordinator, 1 clinical assistant, 1 hygienist, and 1 medical billing manager