 Owner income$78.4k/mo
Owner income$78.4k/moHow Much a Dental Sleep Medicine Practice Owner Can Make at 24 Cases/Month

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$78.4k/mo  Net margin61%-81%
Net margin61%-81% Revenue for target pay$1.54M
Revenue for target pay$1.54M Business difficultyMedium
Business difficultyMedium


You’re not comparing this to a generic dentist salary you’re asking how sleep apnea appliance collections turn into owner cash Over the five-year model period, the first-year setup shows about $139,000 in monthly revenue and $78,400 in operating profit before owner pay, reserves, debt, taxes, and unmodeled dentist compensation The income logic covers completed cases, collections, lab fees, billing friction, marketing, overhead, reserves, and owner role
Owner income$78.4k/moNet margin61%-81%Revenue for target pay$1.54MBusiness difficultyMediumWant to test your owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice. Taxes, personal expenses, denied claims, refunds, and any dentist compensation not already in payroll are excluded.
Want to pressure-test the full model?
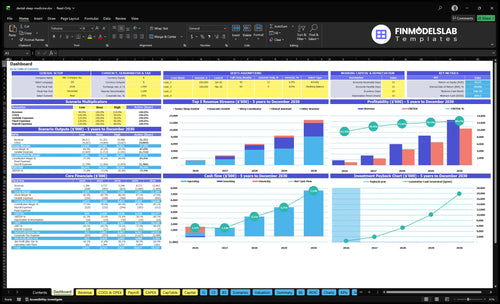
Use the Dental Sleep Medicine Practice Financial Model Template to check revenue, margin, costs, reserves, and owner take-home; charts compare $139,000, $78,400, 564%, and $118M monthly. Open the model.
Owner-income model highlights
- Dashboard to owner income
- $78.4k profit, 564% margin
- $118M mature-year revenue
How many oral appliance cases does a dental sleep medicine practice need to be profitable?
A Dental Sleep Medicine Practice needs completed, collectible cases—not just leads—to stay profitable. With $29,350 in monthly fixed overhead and admin payroll, break-even is about 9 senior-dentist cases at $4,500 each, before reserves and doctor pay. The first-year plan’s 24 completed cases per month would generate about $108,000 in appliance revenue before ancillary visits, so collection timing and payer mix matter as much as volume.
Break-even math
- $29,350 fixed overhead monthly
- About 9 cases to break even
- $4,500 per senior-dentist case
- Before reserves and doctor pay
What drives cash
- 24 completed cases per month planned
- About $108,000 appliance revenue
- Case completion changes real income
- Payer mix and collections decide cash
How much can a dental sleep medicine practice owner take home after expenses?
A Dental Sleep Medicine Practice owner can show about $78,400 in monthly operating profit before owner pay on a first-year model, but that is pre-tax owner cash potential, not guaranteed salary. For margin context, see How Increase Dental Sleep Medicine Practice Profits?; here’s the quick math: $139,000 revenue minus 22.5% variable costs minus $29,350 fixed overhead and admin payroll.
Cash Potential
- $139,000 monthly revenue
- 22.5% variable cost load
- $29,350 fixed overhead and admin payroll
- $78,400 operating profit before owner pay
What Reduces Draw
- Hold cash reserves first
- Pay debt service next
- Cover taxes and refunds
- Fund reinvestment and dentist pay
What affects dental sleep medicine practice profit margins?
Dental Sleep Medicine Practice margins move most with lab fees, supplies, medical billing, physician outreach, payer mix, claim denials, remakes, and follow-up chair time; if you’re sizing startup costs, see How Much To Start A Dental Sleep Medicine Practice?. In year one, variable cost totals 225% of revenue: 120% lab, 30% supplies, 40% billing, and 35% outreach. By a mature year, that drops to 169%, but fixed overhead is still $13,100/month, so low case volume crushes margin fast.
Biggest margin drivers
- Lab fees move margin first
- Supplies and billing add pressure
- Claim denials and remakes raise cost
- Outreach drives first cases
Year-one cost load
- 225% variable cost in year one
- 120% lab cost alone
- 169% mature-year variable cost
- $13,100 monthly fixed overhead
Want the six owner-income drivers?
1
24/moCase Volume
At 60% capacity, the senior dentist completes about 24 cases a month, and more filled slots push owner income up fast.
2
$4.5K/caseCase Price
A $4.5K first-year senior-dentist case price sets cash per case, so pricing moves flow straight into take-home.
3
50%-90%Referral Flow
Higher acceptance and referral flow keep the schedule full, which spreads fixed costs over more cases.
4
12.2%-15%Lab Cost
Lab fees and clinical supplies start near 15% of revenue, so every point down drops more profit to the owner.
5
3.2%-4.0%Billing Cost
Billing and claims run at 4.0% in year 1, and cleaner collections reduce leakage before cash hits the bank.
6
$29.4K/moFixed Burn
Rent, software, insurance, marketing, and admin payroll set the monthly base load before taxes, reserves, debt, refunds, and unmodeled dentist compensation.
Dental Sleep Medicine Practice Core Six Income Drivers
Completed Oral Appliance Cases Per Month
Completed Oral Appliance Cases
This driver is completed, delivered, collectible cases, not leads, consults, impressions, or pending claims. For the first-year senior dentist, the model shows 40 monthly treatment capacity and 24 completed cases, so volume changes show up fast in revenue and owner pay.
At $4,500 collected revenue per first-year senior case, each lost case removes about $3,487.50 of contribution before fixed overhead, using 77.5% contribution. One clean rule: if the case is not delivered and collected, it does not help the draw.
Track Delivered Cases, Not Pipeline
Measure the path from referral to consult, acceptance, delivery, and collection. The owner should forecast from completed cases because cash starts only when the appliance is delivered and collectible.
- Completed cases per month
- Delivery rate by consult
- Collection timing by payer
Watch the gap between accepted and delivered cases each month. Slow scheduling, weak follow-up, or poor case acceptance lowers revenue quality and raises marketing cost per completed appliance.
1
Average Collected Revenue Per Oral Appliance Case
Average Collected Revenue Per Oral Appliance Case
Collected revenue per case is what actually hits cash, not billed charges. In this model, a senior dentist starts at $4,500 per case in year one and reaches $5,000 in the mature year; associate pricing rises from $3,900 in year two to $4,200 mature. At the weighted mature-year level, revenue is about $4,711 per case, so a small pricing or collection gap can move owner pay fast.
This driver includes private pay, medical insurance allowed amounts, deductibles, patient balances, and collection timing. List fees do not equal owner income. If you complete 100 cases, a $100 lift per collected case adds $10,000 of revenue before lab, billing, and overhead, which is why case mix and collection discipline matter.
Track collections, not charges
Measure collected dollars by dentist, payer type, and case age. Track gross charges, allowed amount, patient responsibility, and cash collected within 30, 60, and 90 days. That shows whether higher list prices are real income or just slower cash. If collections lag, owner pay gets squeezed even when case volume looks fine.
- Track collected revenue per completed case.
- Separate private pay and insurance.
- Watch patient balance write-offs.
- Review denied claims and slow payers.
- Price for net collections, not charges.
Use the same collection rules for every case. If mature-year revenue should be $4,711 on average, but your actual net is below that, the gap usually sits in deductibles, denials, or weak follow-up. Fixing that gap lifts gross margin and cash flow without adding new patients.
2
Dental Sleep Medicine Referral Flow and Case Acceptance
Referral Flow to Delivered Cases
Referral flow only pays when it turns into completed appliance deliveries. The first-year target is 24 completed senior-dentist cases per month, so the real inputs are referrals by source, consult booking, case acceptance, and delivery completion. If documentation is weak, consults are slow, or the financial talk is unclear, accepted cases fall and the owner’s income drops even when leads look fine on paper.
Sources include sleep physicians, CPAP-intolerant patients, other dentists, local search, and coordinator follow-up. The quick math is simple: more referrals do not help unless they become delivered cases. A lost case means lost revenue, plus wasted chair time and higher marketing cost per completed appliance.
Measure Source-to-Delivery
Track the full path, not just lead count. Measure referrals, consults booked, show rate, acceptance rate, and cases delivered by source each week. That shows where the leak is, whether it is documentation, timing, follow-up, or payment presentation. The goal is to keep the pipeline full enough to support 24 completed cases without bloating marketing spend.
- Log every referral source.
- Book consults fast.
- Call no-shows within 24 hours.
- Use one clear payment script.
- Review delivered cases weekly.
If coordinator follow-up improves acceptance, the same referral flow supports more collected revenue and a steadier owner draw. If not, fixed staffing and overhead stay in place while cash coming in stays thin.
3
Oral Appliance Lab Cost and Gross Margin
Lab Cost per Case
When you deliver a custom oral appliance, lab and delivery cost set the gross profit left for the owner. The disclosed benchmark says first-year lab fees run at 120% of revenue and improve to 100% in the mature year, while clinical supplies and impression materials move from 30% to 22%. At $4,500 collected revenue, first-year lab plus supply cost is $675 per senior-dentist case under the stated model.
That means the real margin is not just the lab invoice. Remakes, scans, records, chair time, adjustments, and follow-up visits all eat into take-home pay, so a case can look profitable and still leave less cash than expected. If delivered cases slip or remake rates rise, gross profit per case falls fast, and owner draw gets squeezed before fixed overhead is even paid.
Track True Case Margin
Measure collected revenue per case, lab fee, supply cost, and remake count on every finished appliance. One clean rule helps: if the case is not delivered and collected, it does not help gross margin. A simple case sheet should capture the direct cost stack so you can see whether mature-year cost targets are actually moving toward the 100% lab-fee benchmark and 22% supply benchmark.
Watch the hidden time cost too: scans, records, adjustments, and follow-up visits. If those steps start taking more chair time per case, owner income drops even when billing stays flat. The fix is tight case review, fewer remakes, and better workflow control so each $4,500 collection keeps more of its margin for payroll, overhead, and profit draw.
4
Dental Sleep Medicine Medical Billing and Insurance Reimbursement
Billing Friction
Medical billing and claims processing can take 40% of revenue in year one, then 32% in the mature year. That cost load hi ts owner income twice: it reduces cash kept per case and slows when cash lands. In this model, a $5,000 collected case can have about $2,000 tied up in billing work in year one before rent, payroll, and doctor pay.
This driver includes prior authorizations, chart notes, denied claims, payer rules, patient balances, and payment timing. Here’s the quick math: if collections slip or denials rise, the owner does not just lose margin, they lose the cash used to cover payroll and pay themselves. No payer mix, allowed amount, or approval rate is guaranteed, so gross revenue is not the same as take-home income.
Track Net Collections Fast
Measure net collected revenue per case, denial rate, days in A/R, and prior-auth turnaround. If denials spike or authorizations lag, cash flow weakens even when case volume looks fine. The right scorecard is simple: submitted, approved, collected, and still outstanding. That shows where owner income is leaking.
Push for cleaner notes, tighter benefit checks, and same-week claim follow-up. Also track patient balances by aging bucket, because slow patient pay can delay owner draws just like a denied claim. One clean rule helps: if a case is not collectible, it is not income yet.
5
Dental Sleep Medicine Overhead and Owner Staffing Model
Fixed Overhead and Staff Load
This driver sets the floor under owner pay. Fixed overhead is $13,100 a month, and admin payroll is $16,250 in year one, rising to $20,000 from year three. That puts the monthly fixed load at $29,350 before associate, senior dentist, and owner compensation. If contribution falls short, owner draw gets squeezed fast.
Hiring coordinators, assistants, hygienists, and associates can lift capacity, but each hire must earn back its full cost. Model associate pay and owner dentist pay before setting draw. A busy schedule still fails if added payroll eats the cash that should reach the owner.
Track Cash Headroom Weekly
Watch fixed overhead, payroll, completed cases, and owner draw in one monthly model. The key test is simple: does added staff create enough case contribution to cover the new wage load and still leave cash for the owner? If not, delay the hire or reset staffing mix.
- Track cost per completed case.
- Separate fixed and variable labor.
- Model associate comp before hiring.
- Update owner draw after payroll.
6
Compare lean, base, and mature owner-income scenarios
Owner income scenarios
Owner income moves fast in this model because case volume, pricing, staffing, and overhead scale together. The same practice can look thin in launch year and very strong once chair use and referral flow build.
| Scenario | Low CaseLean launch | Base CaseModeled run-rate | High CaseUpside scale |
|---|---|---|---|
| Launch model | The lean case assumes a first-year launch with limited completed cases and tight early margin. | The base case assumes the practice reaches a steadier year-two operating run with more cases and better chair use. | The high case assumes a mature practice with strong referral flow, fuller schedules, and much higher monthly output. |
| Typical setup | Revenue is about $139,000 per month, with 24 completed senior-dentist cases, 225% variable costs, and $29,350 of fixed overhead plus admin payroll before owner pay. | Revenue is about $260,900 per month, with 475 dentist cases, 211% variable costs, and about $176,500 of operating profit before owner pay. | Revenue is about $1.18 million per month, with 2,115 dentist cases, 169% variable costs, and about $944,900 of operating profit before owner pay. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $78,400Launch year | $176,500Year-two run | $944,900Mature year |
| Best fit | Use this to stress-test the opening year when volume is still building and the owner may need to keep draws light. | Use this as the planning middle for lenders, partners, and cash flow work once the practice has a clear referral base. | Use this to test upside when the practice is well staffed, fully booked, and running at mature capacity. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Dental Sleep Medicine Practice Porter's Five Forces Analysis
- Dental Sleep Medicine Practice BCG Matrix
- Dental Sleep Medicine Practice Business Model Canvas
- What Are The 5 Core KPIs For Dental Sleep Medicine Practice Business?
- Dental Sleep Medicine Practice Business Plan Template in Pre-Written Word
- How Increase Dental Sleep Medicine Practice Profits?
- What Are Operating Costs For Dental Sleep Medicine Practice?
- Dental Sleep Medicine Practice Startup Costs: $190K CAPEX Plan
- Dental Sleep Medicine Practice Financial Model Template in Excel
- How to Open a Dental Sleep Medicine Practice in 3 to 6 Months
- How To Write A Business Plan For Dental Sleep Medicine Practice?
- Dental Sleep Medicine Practice Marketing Mix
- Dental Sleep Medicine Practice Marketing Plan
- Dental Sleep Medicine Practice Business Proposal
- Dental Sleep Medicine Practice PESTEL Analysis
- Dental Sleep Medicine Pitch Deck Example Editable PPTX
- Dental Sleep Medicine Practice Business SWOT Analysis
- Dental Sleep Medicine Practice Value Proposition Canvas
Frequently Asked Questions
The researched first-year model shows about $139,000 in monthly revenue and $78,400 in operating profit before owner pay That assumes 24 completed senior-dentist appliance cases per month at $4,500, plus coordinator, assistant, and hygiene sleep visit revenue It excludes taxes, reserves, debt service, refunds, and dentist compensation not listed in payroll