 Owner incomeUp to $80M
Owner incomeUp to $80MHow Much Does a Diagnostic Imaging Center Owner Make? $80M Year 1

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner incomeUp to $80M  Net margin673%–798%
Net margin673%–798% Revenue for target pay$119M–$560M
Revenue for target pay$119M–$560M Business difficultyHard
Business difficultyHard


A diagnostic imaging center owner can have strong income potential, but only after utilization covers staff, rent, service contracts, billing, and equipment costs In the researched base assumptions, first-year revenue is $119M with $80M of EBITDA, or a 673% EBITDA margin, before taxes, debt service, and reserves By the mature year, revenue reaches $560M and EBITDA reaches $446M if scan volume, pricing, and staffing scale as modeled These are planning outputs, not guaranteed owner pay
Owner incomeUp to $80MNet margin673%–798%Revenue for target pay$119M–$560MBusiness difficultyHardWant to test your owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate only, not guaranteed salary, tax advice, or owner distribution advice. Actual take-home depends on revenue, margin, payroll, debt, reserves, and how you structure distributions.
How does owner income show up in the model?
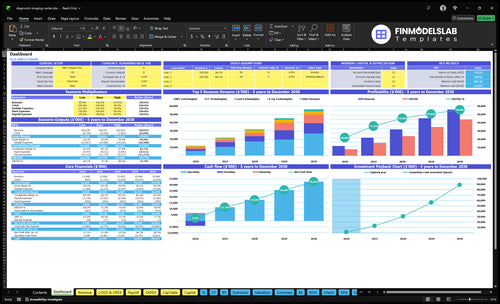
This Diagnostic Imaging Center Financial Model Template shows revenue, EBITDA, cash flow, break-even, and owner take-home assumptions—open the model.
Owner-income model highlights
- Owner pay tracks scans
- MRI, CT, X-ray lines
- Low/base/high scenarios
How much can a diagnostic imaging center owner make?
For a Diagnostic Imaging Center, the modeled owner upside is $80M of Year 1 EBITDA on $119M revenue, but that’s before taxes, debt service, reserves, and owner distributions; What Is The Most Critical Measure Of Success For Your Diagnostic Imaging Center? matters because scan volume drives the cash. This is not a guaranteed salary: owner salary runs through payroll, while distributions come only from after-cost cash.
Modeled Upside
- $119M Year 1 revenue
- $80M Year 1 EBITDA
- $560M mature-year revenue
- $446M mature-year EBITDA
Cash Drivers
- Utilization rises to 820%–880%
- Scan volume is the top lever
- Reimbursement shifts hit margin fast
- Staffing and equipment financing matter
Can a diagnostic imaging center be owner-operated or absentee-owned?
Yes—Diagnostic Imaging Center can be owner-operated or absentee-owned, but the math changes fast. If the owner is not a radiologist, the model still assumes a Medical Director at $400k a year from Year 1 and radiologist payroll starting at 10 FTE in Year 2. Owner-operated only cuts overhead if the owner can handle scheduling, referral growth, billing oversight, compliance, and vendor control; absentee ownership needs stronger reporting, so take-home usually drops.
Owner-operated fit
- Best if owner runs daily ops
- Own referral development and billing
- Track $400k Medical Director cost
- Manage compliance and vendor control
Absentee-owned fit
- Needs stronger management and reporting
- Take-home can fall with more layers
- Scale adds scanners and locations
- Fixed costs spread only if utilization holds
Which imaging services are most profitable?
If you're deciding what to offer first at a Diagnostic Imaging Center, MRI usually shows the biggest modeled revenue in Year 1, but that does not make it the only profit driver. For cost context, see How Much Does It Cost To Open A Diagnostic Imaging Center?. In the model, MRI brings $4,752k per month from 264 completed scans, CT adds $1,824k from 228 scans, and X-ray adds $910k from 455 scans. Profit still depends on reimbursement, scan time, capacity, staffing, service contracts, and downtime, and lower-price X-ray can still help fill gaps and keep referral ties warm.
Modeled volume
- MRI: $4,752k from 264 scans
- CT: $1,824k from 228 scans
- X-ray: $910k from 455 scans
- X-ray helps fill empty slots
Profit levers
- Lead technologist services: $2,063k
- Radiologist services: $341k
- Reimbursement can change ranking
- Downtime and staffing can cut margin
Want the six drivers that move owner income?
1
65%-88%Modality Utilization
Higher scan utilization spreads the $9.024M fixed overhead across more reads, but downtime or missed slots cuts cash fast.
2
$78.7KPayer Mix
Better reimbursement contracts lift revenue per scan, while prior authorization delays and denials slow cash and trim take-home.
3
$102MStaffing Costs
Payroll is the biggest swing factor here, so overtime, idle shifts, and extra reading cover hit margin first.
4
$395MEquipment Financing
The capex load makes debt or lease terms a major cash drain, so payment timing can change owner income quickly.
5
1,257/moReferral Volume
More referrals keep scanners full and lift revenue without a matching jump in fixed cost.
6
6.2%-7.0%Billing Collections
Lower billing fees and tighter reserve needs keep more cash from each scan and speed money in.
Diagnostic Imaging Center Core Six Income Drivers
Modality Utilization
Modality Utilization
Completed scan volume is the main lever here. More finished MRI, CT, X-ray, radiologist, and lead technologist work spreads fixed labor and facility costs over more revenue, so owner take-home improves faster when the schedule stays full. In Year 1, the model shows 550% utilization for lead technologist services, 650% for radiologist and X-ray lines, and 600% for MRI and CT.
Realized volume is lower than booked volume when cancellations, downtime, limited hours, and no-shows hit the calendar. Every missed MRI slot hurts cash more than a missed X-ray slot because the reimbursement is higher, so the same gap can cut profit and the owner’s draw faster on MRI-heavy days.
Track completed scans
Measure scheduled scans, completed scans, cancellation rate, no-show rate, downtime hours, and open hours by modality. Here’s the quick math: completed volume by line times allowed reimbursement drives cash, so you want the highest-value slots filled first. Track MRI and CT separately from X-ray, since the cash loss from one empty MRI slot is much larger.
Use a simple weekly dashboard: MRI, CT, and X-ray completion rate; same-day fill rate for cancels; scanner downtime; and hours used versus hours available. The mature-year model lifts MRI and CT utilization from 600% to 860%, so even small improvements in kept appointments can move gross margin and the owner’s monthly distribution.
1
Payer Mix
Payer Mix
Your take-home moves with the share of commercial insurance, Medicare, Medicaid, cash-pay, and contracted rates. Use allowed reimbursement, not billed charges, because that is what lands in cash. In this model, Year 1 prices are $1,800 MRI, $800 CT, $200 X-ray, $150 radiologist services, and $2,500 lead technologist services, but real payment still depends on geography, payer contract, and CPT code.
Here’s the quick math: average revenue per scan is payer-weighted, so a better commercial mix can lift gross margin and speed collections. A heavier Medicaid or low-rate contract mix can do the opposite, even if scan volume holds. More cash does not mean more charges; it means better allowed amounts and faster collection timing.
Track Allowed Reimbursement
Track allowed dollars per completed scan, payer mix by modality, denial rate, and days in A/R. That tells you whether MRI, CT, and X-ray are actually paying what you expect. If one payer slows payment or underpays relative to contract, owner draw drops even when the schedule is full.
Build the forecast from payer share × allowed amount × scan volume. Test one change at a time: contract rate, authorization flow, or cash-pay policy. One clean line: better payer mix raises revenue quality, not just revenue.
- Measure allowed, not billed.
- Split mix by MRI, CT, X-ray.
- Watch cash speed by payer.
- Flag underpaid CPT codes fast.
2
Staffing And Reading Costs
Payroll Load
Payroll is the first claim on gross profit, so it decides how much cash reaches the owner. The listed Year 1 labor adds to $1.02M — $400k medical director, $100k each for two MRI technologists, $95k CT, $85k X-ray, $50k each for two admin staff, $60k billing, and $80k physician liaison.
The model text says $102M, but the line items sum to $1.02M, so that figure needs a check. If payroll ramps before scan volume does, owner distributions get squeezed fast because labor stays fixed while revenue is still thin.
Track Staffing to Volume
Separate clinical labor from admin overhead. Clinical staff support scan capacity and report speed; admin and billing support scheduling, claims, and cash collection. That split shows where each dollar goes and where you can flex staffing if volume is late.
Here’s the quick test: compare monthly scan volume to payroll every month, then ask whether each added hire is earning its keep. If volume slips, delay backfills, trim overtime, and hold owner pay until staffing matches demand.
- Track scans per labor dollar
- Watch payroll monthly
- Delay hires until volume supports them
- Protect owner draw after payroll
3
Equipment Costs
Equipment Capex and Cash Drain
Equipment costs can crush cash even when the income statement looks fine. This model’s capex totals $26.45M: a $15M MRI, $750k CT, $300k digital X-ray, $200k PACS/RIS, $10M facility build-out, $80k furniture and fixtures, and $120k IT infrastructure.
That is before $25k per month in service contracts, or $300k a year. Financing, downtime, repairs, and replacement reserves can still cut owner take-home even when EBITDA looks strong. Here’s the quick math: big fixed assets mean every idle day and every extra repair dollar hits cash fast.
Track Uptime, Repairs, and Replacement Reserves
Measure each machine’s uptime, service cost, and downtime days, then tie them to scan volume and cash. The key inputs are purchase price, financing terms, annual service contracts, repair reserve, and replacement timing. If MRI or CT goes down, the lost cash is bigger than a missed X-ray slot because the asset base is much larger.
- Track uptime by modality
- Budget service at $300k yearly
- Reserve cash for repairs
- Match debt to useful life
4
Referral Volume
Referral Volume
Referrals are the top of the funnel for MRI, CT, and X-ray slots. More completed scans from physicians, urgent care clinics, specialists, employers, and attorney ties keep utilization high, which protects revenue and spreads fixed costs. The model budgets referral marketing at 40% of revenue in Year 1, easing to 32% by the mature year, so weak referral flow cuts owner pay fast.
One clean metric is completed scans by source. If referral volume slows, same-day slots stay empty and the lost revenue hits hardest on higher-dollar MRI and CT work. A physician liaison costs $80k per year, with 1 FTE in Year 1 and 2 FTE by Year 3, so volume has to rise enough to cover that fixed spend.
Track source quality, not just leads
Measure completed scans, not just inbound referrals, by source and modality. That shows which channels actually fill the schedule and improve cash flow. The quick math is simple: scans times allowed reimbursement, minus referral marketing and liaison cost, tells you whether t he channel adds profit or just activity.
- Track scans by source.
- Watch conversion to completed exams.
- Compare MRI, CT, and X-ray mix.
- Use compliant channels only.
Build volume through safe channels only: physicians, urgent care clinics, specialists, employers, and attorney relationships. Avoid improper referral incentives, and review which sources deliver booked scans, faster fills, and better payer mix. Then shift liaison time to the highest-converting paths.
5
Billing And Collections
Billing and Collections
Billed charges are not cash. Owner income depends on allowed reimbursement, clean claims, prior authorization success, denial management, coding accuracy, and how fast payers and patients pay. In this model, billing and collections run at 70% of revenue in Year 1 and improve to 62% in the mature year, so weak collection work can wipe out margin even if scan volume stays flat.
Key inputs are billed charges, payer mix, approval rates, denial rates, and days to collect. One billing specialist costs $60k a year, with 1 FTE through Year 3 and 2 FTE from Year 4. Here’s the quick math: better collections raise cash flow and owner draw without adding one more scan.
Track Clean Claims Fast
Measure clean-claim rate, prior-auth approval rate, denial rate, and days in A/R (accounts receivable, or money owed to you). If claims fail on coding or authorization, revenue turns into slow cash, not profit. Keep a tight log by payer and procedure so you can see where reimbursement leaks out.
Track this weekly:
- Allowed reimbursement, not billed charges
- Denials by payer and CPT code
- Days in A/R and cash collected
- Staff time per claim and appeal
If collections slip, margin drops before scan volume does. That is the risk.
6
Compare low, base, and high diagnostic imaging center owner income scenarios
Owner income scenario table
Owner income shifts with scan volume, payer mix, staffing, and equipment costs. The same center can look tight in ramp-up and far stronger once utilization and collections steady out.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | The low case models a ramp-up year with limited volume and heavier fixed costs. | The base case models a scaled year with steadier throughput and tighter cost control. | The high case models a mature year with high utilization and stronger margin capture. |
| Typical setup | About 1,257 scans a month, $80M EBITDA, and a 673% EBITDA margin before debt, taxes, and reserves, with staffing, equipment payments, collection rate, reserves, and payer mix still settling. | About 3,366 scans a month, $242M EBITDA, and a 760% EBITDA margin in a scaled setup with steadier staffing, collections, and equipment service. | About 5,195 scans a month, $446M EBITDA, and a 798% EBITDA margin at high utilization, with the center running close to full capacity. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $80M EBITDARamp-up | $242M EBITDAScaled | $446M EBITDAHigh utilization |
| Best fit | Use this to stress-test slow referrals, weaker collections, or a longer ramp. | Use this as the main planning case for budgeting and monthly management. | Use this to test upside when volume, utilization, and collections all run strong. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Diagnostic Imaging Center Porter's Five Forces Analysis
- Diagnostic Imaging Center BCG Matrix
- Diagnostic Imaging Center Business Model Canvas
- 7 Critical KPIs to Measure for a Diagnostic Imaging Center
- Diagnostic Imaging Center Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Diagnostic Imaging Center Profitability
- How Much Does It Cost To Run A Diagnostic Imaging Center Each Month?
- Diagnostic Imaging Center Startup Costs: $375M CAPEX Plan
- Diagnostic Imaging Center Financial Model Template in Excel
- How To Start a Diagnostic Imaging Center in 9–18 Months
- How to Write a Diagnostic Imaging Center Business Plan
- Diagnostic Imaging Center Marketing Mix
- Diagnostic Imaging Center Marketing Plan
- Diagnostic Imaging Center Business Proposal
- Diagnostic Imaging Center PESTEL Analysis
- Diagnostic Imaging Center Pitch Deck Example Editable PPTX
- Diagnostic Imaging Center Business SWOT Analysis
- Diagnostic Imaging Center Value Proposition Canvas
Frequently Asked Questions
In the researched model, the center produces $80M of Year 1 EBITDA on $119M of revenue, before taxes, debt service, and reserves By the mature year, EBITDA reaches $446M on $560M of revenue Owner take-home depends on how much cash is held back for debt, equipment replacement, and working capital