Diagnostic Imaging Center Startup Costs: $375M CAPEX Plan

Key Takeaways
- Equipment choice drives the biggest upfront imaging spend.
- Buildout costs hit before the center opens.
- PACS/RIS needs setup plus ongoing licensing.
- Payroll and overhead require heavy cash reserves.
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a diagnostic imaging center, with spend spread across Month 1 to Month 4.
CAPEX only This block covers capitalized startup assets only. It excludes working capital, inventory, payroll runway, deposits, debt service, financing fees, payer lag, and ongoing operating expenses.
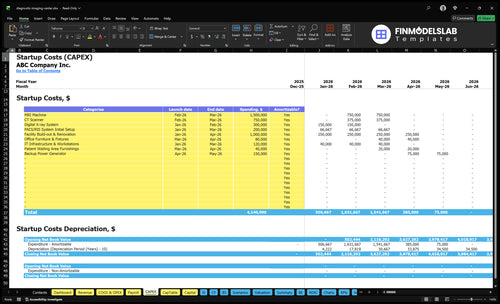
What does the CAPEX tab show?
The Diagnostic Imaging Center Financial Model Template CAPEX tab shows startup costs, timing, amounts, depreciation, and amortization; review assumptions now.
CAPEX screenshot highlights
- MRI $15M, Month 1-4
- CT $750k, X-ray $300k
- PACS $200k, buildout $10M
How do diagnostic imaging equipment costs change by modality mix?
For a Diagnostic Imaging Center, equipment cost moves mostly with modality mix: the listed figures are MRI at $15M, CT at $750k, digital X-ray at $300k, and PACS/RIS initial setup at $200k. Here’s the quick math: one added MRI room changes the plan far more than one added X-ray room, while CT sits in the middle with real buildout and shielding needs. Final cost also shifts with new vs. refurbished gear, installation, coils, injectors, tables, warranties, service contracts, shielding, and room readiness, so one quote is not the market price.
Highest cost mix
- MRI is the biggest line at $15M.
- One MRI room can reshape CAPEX.
- CT adds meaningful buildout costs.
- X-ray supports volume with lower CAPEX.
What changes final price
- New and refurbished prices differ.
- Installation and room readiness add cost.
- Coils, injectors, and tables matter.
- Warranties and service contracts matter too.
What hidden costs should a diagnostic imaging center budget include?
The hidden costs in a Diagnostic Imaging Center budget are the cash items that hit before reimbursement does: working capital, credentialing delays, payer enrollment, and launch costs that are not capital assets. That means planning for Year 1 payroll of $102M, plus $8k/month insurance, $3k/month professional fees, $30k/month rent, $65k/month utilities, and $25k/month service contracts; see How Much Does The Owner Of A Diagnostic Imaging Center Typically Make? for the owner side. Slow collections can still create a cash gap even when scan volume is booked.
Cash costs to fund
- Working capital for early payroll
- Payer collections lag after scans
- Pre-opening payroll before revenue
- Insurance binders and setup fees
Launch costs to budget
- Medical physicist surveys
- Accreditation preparation
- Legal setup and payer enrollment
- Compliance consulting and launch marketing
How much money do you need to open a diagnostic imaging center?
You need more than the equipment budget to open a Diagnostic Imaging Center: the visible startup budget starts with listed CAPEX of $375M across Month 1–Month 4, then adds pre-opening costs, working capital, and contingency; see What Is The Most Critical Measure Of Success For Your Diagnostic Imaging Center? for the operating metric that keeps that spend honest. Here’s the quick math: $752k/month fixed overhead plus about $850k/month payroll run-rate equals roughly $1.602M/month before variable costs and reimbursement delays.
Budget stack
- Start with $375M CAPEX
- Add pre-opening vendor costs
- Fund claims collection delays
- Hold contingency for payer timing
Cash pressure
- Plan $10.2M Year 1 payroll
- Cover $752k/month fixed overhead
- Expect 165% variable cost load
- Watch licensing and accreditation delays
Calculate Fuding Needs
Startup cost summary
Summary of startup equipment, build-out, systems, and opening cash needed for a diagnostic imaging center.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| MRI Machine | $1,500,000 | Equipment purchase and installation in Month 2-Month 3. | Yes |
| Facility Build-out & Renovation | $1,000,000 | Leasehold work and medical fit-out in Month 1-Month 4. | Yes |
| CT Scanner | $750,000 | Scanner purchase and setup in Month 2-Month 3. | Yes |
| Digital X-ray System | $300,000 | Digital imaging hardware in Month 1-Month 2. | Yes |
| PACS/RIS System Initial Setup | $200,000 | Software setup, integration, and IT work in Month 1-Month 3. | Yes |
| Opening Cash Buffer | $1,554,000 | Month 3 cash shortfall from payroll and fixed overhead ramp. | No |
Diagnostic Imaging Center Core Five Startup Costs
Diagnostic Imaging Equipment Startup Expense
Top Equipment Cost
Diagnostic imaging equipment is the biggest CAPEX line. Using the source figures, MRI is $15M, CT is $750k, digital X-ray is $300k, and PACS/RIS setup is $200k. Timing runs Month 1-Month 3. The real budget depends on room count, daily scan volume, referral mix, and how much contrast imaging you expect.
What the Quote Covers
Price each modality separately, not as one vendor quote. Add the extras that make the room usable: coils, injectors, patient tables, monitors, control-room gear, accessories, installation, warranties, and service contracts. Decide on purchase versus lease and new versus refurbished before you lock the capex plan, because those choices move cash needs a lot.
Right-Sizing Inputs
Model the build by room and by modality. Ask: how many rooms, daily scan volume, referral mix, contrast studies, maintenance coverage, and uptime targets. Then size capital for coils, injectors, tables, monitors, control-room gear, installation, warranties, and service contracts. That is how you avoid underbuying the first site.
Cost Control
The main way to trim cost is to match equipment to demand, not prestige. If scan volume is still unproven, leasing or refurbished gear can protect cash, but only if service coverage and uptime stay strong. The wrong cut is skipping warranties or maintenance, because one outage can erase the savings.
Facility Buildout And Imaging Suite Startup Expense
Buildout Budget
For an imaging center, the facility buildout is a separate cash need from equipment. The source figure is $10M for buildout and renovation across Month 1-Month 4, before opening. That budget covers the rooms and infrastructure needed to support MRI, CT, and X-ray work, not the scanners themselves.
What It Covers
This cost includes exam rooms, control rooms, waiting areas, patient changing areas, ADA access, flooring, plumbing, electrical upgrades, HVAC, shielding, MRI safety zoning, and equipment rigging. Plan it with site quotes and the landlord work letter, because the scope changes fast when the shell is unfinished.
Cost Drivers
The real cost drivers are site condition, modality mix, local code, ceiling height, floor loading, and utility capacity. MRI and CT rooms usually add more construction complexity than general exam space, so a simple tenant finish can land far below a site that needs structural, electrical, or shielding work.
Before Opening
Keep buildout timing separate from equipment CAPEX. This spend runs in Month 1-Month 4 and should be finished before go-live, because rooms, shielding, and rigging must be ready before scanners arrive. If opening is delayed, the cash burn stays high while revenue is still at zero.
PACS RIS And Radiology IT Startup Expense
Core setup
The $200k startup line covers Month 1–Month 3 PACS/RIS setup, not office tech. It funds the picture archiving and communication system (PACS), radiology information system (RIS), DICOM storage, scheduling, billing interfaces, electronic health record links, cybersecurity, reading workstations, reporting tools, backup, and teleradiology connectivity. DICOM is the standard format used to store and share medical images.
Budget inputs
To size this cost, ask for quotes by module and count the interfaces, workstations, and storage volume. The key inputs are user seats, sites, Months 1–3 of launch coverage, and whether backup or teleradiology links are bundled. Keep this separate from imaging equipment and buildout, because it is the IT layer, not the scanner or suite.
- Count every interface and user seat.
- Confirm storage and backup scope.
- Separate IT from equipment CAPEX.
Year 1 license
Year 1 software licensing is 20% of revenue, so the fee scales with collections. That ongoing cost should cover support, updates, cybersecurity upkeep, reporting tools, and connected workflows if the contract says so. Do the math from your revenue forecast, then check what is excluded so you do not double count backup or connectivity.
Keep scope tight
Keep the setup lean by buying only the modules needed for opening day and pushing noncritical add-ons later. The common mistake is folding recurring support into the one-time budget, which hides the true cash need. Use separate line items for setup, license, and support, and verify quotes for DICOM storage, EHR integration, and teleradiology links before signing.
Licensing Accreditation And Compliance Startup Expense
License setup
Month 1 starts the compliance clock. State licensing, radiation control registration, accreditation prep, medical physicist testing, legal setup, payer enrollment, credentialing, radiation safety policies, and privacy compliance are all separate tasks. Plan $3k/month in professional fees from Month 1 to Month 60, plus $8k/month in insurance premiums if binders are needed before reimbursement starts.
Cost drivers
No single national fee applies. Costs change by state, modality, and payer rules, so build the budget task by task. The owner should track filings, counsel should handle entity and contract work, the compliance lead should build policies, and the physicist should cover testing. Timing usually runs from Month 1 through pre-opening.
- State license and radiation registration
- Accreditation prep and physicist testing
- Payer enrollment and credentialing
How to plan it
Use the $3k/month professional-fee anchor for legal, consulting, and filing work, then hold a separate reserve for delays. State-by-state rules can stretch timing, and reimbursement can lag, so don’t underbuild cash. The practical move is to budget for setup plus at least one early operating gap, not just the filing fee.
Cash reserve
Hold enough cash to cover compliance work, insurance, and slow payer starts. A clean planning floor is $3k/month in professional fees plus $8k/month in insurance premiums until binders and enrollment clear. That reserve keeps licensing, accreditation, and credentialing moving while reimbursement is still waiting.
Staffing Insurance Supplies And Working Capital Startup Expense
Pre-open payroll
The listed Year 1 team totals $10.2M/year across 90 positions, or about $850k/month. That is the first cash bridge to fund before imaging volume and payer receipts ramp.
- 10 Medical Director at $400k
- 20 MRI Technologists at $100k each
- 10 CT Technologist at $95k
- 10 X-ray Technologist at $85k
- 20 Administrative Staff at $50k each
- 10 Billing Specialist at $60k
- 10 Physician Liaison at $80k
Monthly overhead
Fixed overhead is $752k/month, or $9.024M/year, for rent, utilities, service contracts, insurance, admin software, office supplies, and professional fees. Add contrast media, linens, disposables, training, credentialing time, billing lag, and launch marketing. These are cash needs, not equipment CAPEX.
Cash control
Use a monthly cash forecast and stage hiring to match opening dates. The common mistake is funding scanners and buildout, then running short on payroll, supplies, and payer lag. Keep inventory tight, pre-negotiate service terms, and separate one-time setup from recurring spend.
Working capital bridge
Working capital should cover the gap between launch costs and collections. For this center, the burn starts with staffing, overhead, and consumables, so the budget has to fund daily operations before fee-for-service cash comes in.
Compare 3 Startup Cost Scenarios
Startup cost scenarios
Lean, base, and full launches change capex, staffing, and working capital fast. More modalities and rooms raise upfront cash needs, while referral volume and payer mix decide how quickly the site fills.
| Scenario | Lean LaunchLower CAPEX | Base LaunchBalanced outpatient | Full LaunchMulti-modality |
|---|---|---|---|
| Launch model | Starts with one or two core modalities and a smaller room count to keep capital and staffing light. | Uses the planned outpatient mix of MRI, CT, and digital X-ray with the support team needed to run steady volume. | Adds more modalities, more rooms, more techs, deeper storage, and more cash to handle a slower ramp. |
| Typical setup | Use a smaller buildout, limited storage, and a lean front desk and billing team. | It carries the main equipment, PACS/RIS, Year 1 payroll of about $1.02M, and fixed overhead of about $75.2k per month. | This version needs a larger site, heavier staffing, and a bigger working capital reserve than the base plan. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | $2M - $3MLower cash need | $4M - $5MCore plan | $6M - $8MHigher funding |
| Best fit | Best for dense referral pockets, simpler payer mix, and markets where early demand is still being proven. | Best for stable referral volume, mixed payer contracts, and markets that can support multi-modality flow. | Best for high referral volume, strong payer mix, and markets with enough demand to fill added capacity. |
Planning note: These scenario ranges are research-based planning assumptions, not exact vendor quotes or final bid prices.
Related Products
- Diagnostic Imaging Center Porter's Five Forces Analysis
- Diagnostic Imaging Center BCG Matrix
- Diagnostic Imaging Center Business Model Canvas
- 7 Critical KPIs to Measure for a Diagnostic Imaging Center
- Diagnostic Imaging Center Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Diagnostic Imaging Center Profitability
- How Much Does It Cost To Run A Diagnostic Imaging Center Each Month?
- Diagnostic Imaging Center Financial Model Template in Excel
- How Much Does a Diagnostic Imaging Center Owner Make? $80M Year 1
- How To Start a Diagnostic Imaging Center in 9–18 Months
- How to Write a Diagnostic Imaging Center Business Plan
- Diagnostic Imaging Center Marketing Mix
- Diagnostic Imaging Center Marketing Plan
- Diagnostic Imaging Center Business Proposal
- Diagnostic Imaging Center PESTEL Analysis
- Diagnostic Imaging Center Pitch Deck Example Editable PPTX
- Diagnostic Imaging Center Business SWOT Analysis
- Diagnostic Imaging Center Value Proposition Canvas
Frequently Asked Questions
The provided plan includes $255M for major imaging equipment: $15M for MRI, $750k for CT, and $300k for digital X-ray It also includes $200k for PACS/RIS initial setup, which supports image storage, workflow, and reporting These are researched planning assumptions, not vendor quotes