 Time to Open4-9 monthsSetup window
Time to Open4-9 monthsSetup windowHow To Open A Dizziness And Balance Disorder Clinic In 4–9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open4-9 monthsSetup window  Launch Sequence8 stagesCompliance first
Launch Sequence8 stagesCompliance first Key BottleneckPayer gateApproval path
Key BottleneckPayer gateApproval path First Revenue StepPaid evalIntake ready
First Revenue StepPaid evalIntake ready


A dizziness and balance disorder clinic can usually open in about 4 to 9 months if state licensing, payer credentialing, equipment setup, EHR setup, staff hiring, and referral outreach move in parallel The researched planning assumptions include Year 1 treatment capacity of 120 monthly visits per vestibular audiologist, 140 per vestibular physical therapist, and 80 per neurotologist, before utilization is applied The biggest launch bottleneck is payer credentialing plus trained clinician and vestibular equipment readiness First revenue starts when physician referrals and direct-access patients convert into initial evaluations, diagnostic testing, and therapy visits
Time to Open4-9 monthsSetup windowLaunch Sequence8 stagesCompliance firstKey BottleneckPayer gateApproval pathFirst Revenue StepPaid evalIntake readyLaunch timeline
This is a short web summary of the launch plan; the XLSX export includes the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9
Licensing / compliance
- License map
- Policy binder
- Inspection prep
- Final approval
Lease / buildout
- Lease signed
- Floor plan
- Safety flooring
- Punch list
Equipment / IT
- Vendor quotes
- Order systems
- IT setup
- VNG install
- Balance install
- Rotary chair setup
Staffing / training
- Role plan
- Recruit clinicians
- Hire team
- Train workflows
Payer / billing
- Payer roster
- Credential packets
- Follow-up calls
- Billing tests
Referrals / opening
- Referral map
- Outreach kit
- Physician visits
- Soft opening
Why check the financial model before you pick an opening month?
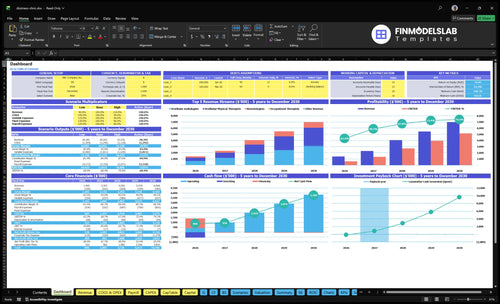
The screenshot in the Dizziness and Balance Disorder Clinic Financial Model Template shows patient ramp, assumptions, revenue, costs, cash needs, runway, and break-even logic—open the model.
Financial model highlights
- About $164.7k monthly revenue
- 185% variable cost load
- $21.7k fixed overhead
- $38.7k monthly wages
- $490k capex before IT
What licenses do you need to open a dizziness clinic?
To open a Dizziness and Balance Disorder Clinic, you need state-specific medical authority, licensed providers, compliant facility operations, malpractice coverage, payer enrollment, and signed clinical policies before seeing patients; for operating metrics after launch, see What Are The 5 Core KPIs For Dizziness And Balance Disorder Clinic?. This matters because the CDC reports 1 in 4 adults age 65+ falls each year, so clinical compliance has to come before marketing.
Core licenses
- State medical license for physicians
- Audiology, PT, and OT licenses
- Assistant credentials where required
- Facility permits based on state rules
Launch checks
- Active medical director before opening
- Malpractice insurance in force
- HIPAA and OSHA policies signed
- Payer enrollment matched to billed services
How long does payer credentialing take for a dizziness clinic?
For a Dizziness and Balance Disorder Clinic, payer credentialing usually sits inside the 4 to 9 month launch window, and it can be the step that slows opening. Start it with the lease, equipment orders, and EHR build, because cash can lag patient visits if claims are not clean. Timing still varies by payer, state, and provider roster.
What slows it down
- Incomplete provider files
- Payer enrollment backlogs
- Facility readiness delays
- Clinician hiring sequence
What to verify first
- Test claims before soft opening
- Payer IDs and fee schedules
- Referral authorizations
- Denial workflows
How do you get patients for a dizziness clinic?
Patients for a Dizziness and Balance Disorder Clinic should come first from physician referrals, then direct-access patients where allowed, primary care, otolaryngology, neurology, urgent-care follow-up, audiology, physical therapy, and local search. Start outreach before opening month, and use the service mix to decide who to call first; for KPI tracking, see What Are The 5 Core KPIs For Dizziness And Balance Disorder Clinic? The first revenue step is turning referrals into initial evaluations, then diagnostic tests and therapy visits, and the referral ramp can take longer than room readiness.
Who to call first
- Start with physician referrals.
- Call primary care offices early.
- Target otolaryngology and neurology.
- Follow urgent-care discharge cases.
What to sell first
- Lead with initial evaluations.
- Offer diagnostic testing next.
- Sell vestibular therapy visits.
- Plan 50% of Year 1 revenue for referral marketing.
Check whether the clinic is ready to schedule patient appointments
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Compliance
- State licenses confirmedCritical
Needed before any clinical work or billing starts.
- Scope of practice reviewedCritical
Keeps services inside state rules and clinician limits.
- Malpractice coverage boundCritical
Protects the clinic before patient care begins.
- HIPAA safeguards activeCritical
Patient data must be protected from day one.
- OSHA basics documentedHigh
Worksite rules and injury controls must be in place.
Facility
- Rooms fully builtCritical
Rooms must be finished before test visits start.
- Safety flooring installedCritical
Slip risk is high in balance care, so safety floors matter.
- Waiting area readyHigh
Patients need a calm, usable check-in area.
- Accessibility paths clearHigh
Clear access reduces fall risk and delays.
- Infection supplies stockedHigh
Stock controls infection risk and visit interruptions.
Equipment
- VNG suite installedCritical
Diagnostic work cannot start without the VNG suite.
- Posturography calibratedCritical
Balance results must be accurate before opening.
- Rotary chair testedHigh
The rotary chair needs a clean test run first.
- VEMP equipment verifiedHigh
VEMP testing must work before soft opening.
- Maintenance logs setMedium
Log servicing now to avoid early downtime.
Staffing
- Year 1 staffing matchedCritical
Year 1 needs 2 audiologists, 3 PTs, 1 neurotologist, 1 OT, and 2 assistants.
- Clinician credentials checkedCritical
Only credentialed staff can treat or interpret tests.
- Roles and coverage setHigh
Coverage gaps will slow intake and follow-up.
- Clinical training completedHigh
Staff need protocol training before patient volume starts.
- Escalation paths rehearsedHigh
Escalation steps matter when fall risk spikes.
Patient flow
- EHR liveCritical
EHR must be live at the model's $1,800 per month.
- Billing workflow testedCritical
Claims need a working path before first billed visit.
- Claim edits checkedHigh
Rejected claims should be caught before launch.
- Referral pipeline activeCritical
Referrals drive the first revenue step, so this must be active.
- Follow-up scheduling setHigh
Follow-up visits keep therapy plans moving.
Finance
- Fixed overhead confirmedCritical
Fixed overhead is $21,700 per month before wages.
- Cash runway reviewedCritical
Cash must cover the $614k low point in Month 2.
- First month plan readyHigh
Billing setup should support about 60% of Year 1 revenue.
- Go-live signoff completedCritical
Final signoff keeps gaps from slipping into opening.
Want to pressure-test the six launch drivers before opening?
1Clinical Lead
License gateActive medical leadership and verified licenses let the clinic open safely and avoid compliance delays.
2Billing Setup
Payer IDsPayer IDs and test claims turn first visits into collectible cash and cut claim rework.
3Room Ready
6-mo buildInstalled and calibrated vestibular rooms keep testing from stalling on layout, training, or IT.
4Team Ready
9 rolesTrained clinical coverage keeps evaluations, therapy, and follow-up moving without bottlenecks.
5Referral Flow
Pre-openA named referral list and outreach plan bring in the first evaluations and therapy plans.
6Workflow Ready
Flow testTested intake, documentation, and claim handoff reduce denials and front-desk chaos on day one.
Clinical Leadership And Licensure
Clinical Authority and Licensure
A dizziness clinic can’t open safely without clear clinical authority. The first gate is an active medical director, a verified licensed provider roster, and written rules for service scope, referral acceptance, malpractice coverage, state medical compliance, and scope-of-practice limits.
Here’s the quick math: the Year 1 model assumes 1 medical director at $240,000 plus 1 neurotologist. If authority is unclear on day one, scheduling slows, documentation gets messy, and payer or compliance delays can push back first revenue.
Lock the medical rules before booking visits
Before opening, verify each license, confirm malpractice coverage, and get signed supervision rules and approved clinical policies in place. That gives the team one playbook for who can do what, which referrals to accept, and when to escalate cases.
- Assign one medical director.
- Document scope-of-practice limits.
- Approve referral acceptance rules.
- Test compliance review before soft opening.
What this protects: safer scheduling, cleaner notes, and fewer launch-day surprises when patients start arriving. If this step slips, the clinic may have rooms ready but still not be ready to treat.
1
Payer Credentialing And Billing Setup
Payer Credentialing and Billing Setup
Insured visits only turn into cash after the clinic is enrolled, contracted, and set up to bill correctly. If payer IDs, coding rules, or authorization checks are missing, you can open your doors and still wait weeks for collectible revenue.
The model puts medical billing and revenue cycle management at 60% of Year 1 revenue, so this is a major launch item. The bottleneck is simple: seeing patients before claims can be submitted cleanly creates denials, rework, and slower first cash collection.
Get Claims Live Before Soft Opening
Before soft opening, verify provider enrollment, payer contracts, coding workflows, billing vendor handoff, and authorization rules. Run clean test claims and confirm active payer IDs for every billable provider. That is the real go/no-go test for day-one revenue.
- Assign one owner to credentialing.
- Track each payer by status.
- Log denials the first week.
- Check reimbursement timing in writing.
- Train front desk on authorizations.
2
Vestibular Equipment And Room Readiness
Vestibular Room Readiness
Equipment and room setup can make or break opening day. This clinic cannot start on time if the testing rooms are still waiting on buildout, IT, or staff training. The first-day setup should match the services offered, not a wish list: VNG at $65,000 in Month 1 to Month 2, VEMP at $25,000 in Month 1, posturography at $120,000 in Month 1 to Month 3, and fit-out plus patient safety flooring at $150,000 in Month 1 to Month 3.
The later installs matter too: rehabilitation gym equipment at $45,000 in Month 2 to Month 4 and a rotary chair system at $85,000 in Month 3 to Month 6. Readiness means the rooms are installed, calibrated, integrated, and staff-tested. If one piece is late, the clinic may open with gaps in testing capacity and weaker first-day patient flow.
Sequence the buildout
Lock the room layout before equipment delivery, because a late floor plan change can stall everything behind it. Tie each device to the service it supports, then verify power, data, safety flooring, and calibration dates before scheduling staff. One clean rule: no room is ready until the team can use it without help.
Use a simple go-live checklist for each room: installed, calibrated, integrated with IT, and staff-tested. Track vendor dates for Month 1 through Month 6, and hold back the first patient slots if training slips. The biggest risk is paying for equipment that sits idle while the room, software, or staff catch up.
- Confirm room layout before ordering
- Match devices to booked services
- Test IT before patient scheduling
- Train staff on each room
3
Staffing And Clinical Protocols
Role-Ready Staffing
A dizziness clinic cannot open on time with partial coverage. The Year 1 model needs 2 vestibular audiologists, 3 vestibular physical therapists, 1 neurotologist, 1 occupational therapist, and 2 rehabilitation assistants so evaluations, testing, therapy, and follow-up can run from day one.
The admin layer matters too: 1 clinic manager at $85,000, 1 care coordinator at $55,000, and 2 front desk receptionists at $42,000 each total $224,000. If these roles are late, equipment sits idle, visits get missed, and the opening date slips. Staffing here is about coverage, not just headcount.
Sequence the Team First
Build the schedule around who must be trained and live on day one: testing, documentation, scheduling, patient follow-up, and therapy coordination. Here’s the quick check: every role should have a named backup, a written scope, and a first-week template before equipment install finishes.
- Assign coverage for each visit type.
- Train front desk on intake and follow-up.
- Test handoffs before first patient day.
What this hides: if clinicians are hired after equipment is installed, the clinic can still open, but flow breaks fast. That means longer waits, weaker utilization, and more no-shows because patients don’t get a clean path from evaluation to treatment.
4
Referral Network And Patient Acquisition
Referral Network Readiness
If you open without referral sources lined up, the clinic may be live but underbooked in week one. In this model, 50% of Year 1 revenue is tied to physician referral marketing, so launch timing depends on referral flow, not just rooms and equipment. Building this before opening month helps pull in initial evaluations, vestibular testing, and therapy plans sooner.
The real dependency is trust. A dizziness clinic needs named contacts in primary care, otolaryngology, neurology, urgent care, audiology, physical therapy, and local search before day one. If that trust starts after opening, first revenue slips, schedules stay thin, and staff time gets burned on empty slots instead of patient care.
Pre-Open Referral Setup
Before opening, verify a named referral list, outreach calendar, education materials, intake path, and follow-up loop. Each source should know what to send, how to send it, and when they will hear back. That keeps referrals moving instead of sitting in voicemail or a generic inbox.
- Assign one owner per referral source
- Test intake before soft opening
- Send visit feedback fast
- Track every referral touchpoint
The quick test is simple: if a doctor calls on day one, can staff book, triage, and confirm the visit the same day? If not, the acquisition system is still a launch risk, and cash from new patient visits will arrive later than planned.
5
EHR, Compliance, And Operating Workflow
EHR And Day-One Workflow
If the rooms are ready but the EHR flow is not, opening turns into manual work. A dizziness clinic needs one system that handles intake, referral tracking, clinical notes, test results, billing handoff, scheduling, patient messages, privacy, and reporting on day one.
The model assumes $1,800 per month for EHR and practice management software. The readiness signal is a tested patient journey from referral to claim submission; if that path is weak, denials rise, follow-up slips, and the front desk gets swamped.
Test The Referral To Claim Path
Build the workflow in order: referral intake, authorization checks, consent forms, clinical documentation, fall-risk notes, test posting, claim handoff, and follow-up tasks. Assign one owner for each step before the first patient arrives so nothing sits in limbo.
Also verify HIPAA safeguards and OSHA basics, then run a mock day with one referral, one vestibular test, and one claim. If charting, coding, or scheduling breaks in the test, it will break harder when phones ring and patients are waiting.
- Confirm referral intake fields.
- Check authorization before visits.
- Capture consent at check-in.
- Document fall-risk notes clearly.
- Send follow-up tasks same day.
6
Related Products
- Dizziness and Balance Disorder Clinic Porter's Five Forces Analysis
- Dizziness and Balance Disorder Clinic BCG Matrix
- Dizziness and Balance Disorder Clinic Business Model Canvas
- What Are The 5 Core KPIs For Dizziness And Balance Disorder Clinic?
- Dizziness and Balance Disorder Clinic Business Plan Template in Pre-Written Word
- How Increase Dizziness And Balance Disorder Clinic Profitability?
- What Are Operating Costs For Dizziness And Balance Disorder Clinic?
- Dizziness and Balance Disorder Clinic Startup Costs: $614K Cash Need
- Dizziness and Balance Clinic Financial Model Template in Excel
- How Much a Dizziness and Balance Disorder Clinic Owner Can Make: $396k-$69M
- How To Write A Business Plan For Dizziness And Balance Disorder Clinic?
- Dizziness and Balance Disorder Clinic Marketing Mix
- Dizziness and Balance Disorder Clinic Marketing Plan
- Dizziness and Balance Disorder Clinic Business Proposal
- Dizziness and Balance Disorder Clinic PESTEL Analysis
- Dizziness And Balance Clinic Pitch Deck Example Editable PPTX
- Dizziness and Balance Disorder Clinic Business SWOT Analysis
- Dizziness and Balance Disorder Clinic Value Proposition Canvas
Frequently Asked Questions
Start by locking clinical leadership, service scope, licensing, and payer enrollment before you sign up the first patient The researched launch path assumes a 4 to 9 month window, Year 1 staffing of 2 vestibular audiologists, 3 vestibular physical therapists, and 1 neurotologist, plus therapy and rehab support Build referrals while equipment, EHR, and billing workflows are still being set up