 Owner income$396k
Owner income$396kHow Much a Dizziness and Balance Disorder Clinic Owner Can Make: $396k-$69M

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$396k  Net margin43% → 74%
Net margin43% → 74% Revenue for target pay$1.65M → $7.55M
Revenue for target pay$1.65M → $7.55M Business difficultyHard
Business difficultyHard


You’re modeling clinic ownership, not a general clinician salary Using the provided five-year assumptions, owner-income capacity ranges from about $396k in first-year cash after $490k startup capex to about $69M in mature-year operating profit before personal taxes, debt service, and reserves
Owner income$396kNet margin43% → 74%Revenue for target pay$1.65M → $7.55MBusiness difficultyHardWant to test your own clinic income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate only, not guaranteed salary, tax advice, or owner distribution advice.
How do you check owner income in this model?
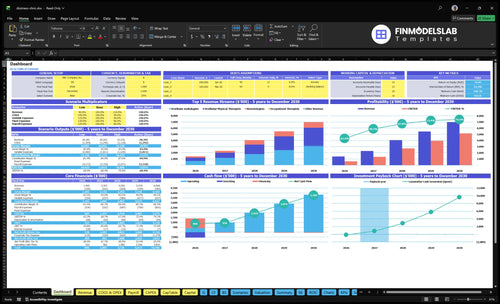
This Dizziness and Balance Disorder Clinic Financial Model Template shows dashboard, income outputs, payer mix, visit volume, testing revenue, staffing, overhead, startup capex, scenarios, reserves, and owner pay—open the model.
Owner-income model highlights
- $1,647k to $7,552k revenue
- 449% and 764% margins
- $490k startup investment
How does payer mix affect dizziness clinic owner income?
If your Dizziness and Balance Disorder Clinic takes a different payer mix, your income changes fast because collected revenue, denials, and cash timing all move together. Here’s the quick math: the supplied mix implies about $183 per billable encounter in first-year weighted revenue, and billing plus revenue cycle management can run at 60% of revenue in year one, or about 50% in a mature year.
Payer mix drives collected cash
- Commercial insurance usually pays faster
- Medicare changes the collected average
- Cash pay lifts timing, not just price
- Denials cut realized revenue, not billed revenue
Model it as a variable
- Use $183 per encounter in year one
- Plan 60% RCM cost in year one
- Plan 50% RCM cost in mature years
- Treat reimbursement as assumptions, not fixed rates
Can a dizziness clinic owner make more by hiring clinicians?
Yes—if the Dizziness and Balance Disorder Clinic keeps added clinicians busy, owner income can rise fast. In the model, provider counts scale from 2 audiologists, 3 physical therapists, 1 neurotologist, 1 occupational therapist, and 2 rehabilitation assistants in year 1 to 6, 10, 2, 3, and 6 in the mature year, and monthly revenue grows from $1,647k to $7,552k. Just keep clinical pay separate from owner return, because the supplied payroll already includes Medical Director and admin roles, so any missing treating-provider wages still need to be added before you rely on distributions.
Why hiring can lift income
- More providers can raise booked volume.
- Revenue rises from $1,647k to $7,552k.
- Owner pay improves after payroll is covered.
- Unused capacity kills the upside.
What to check first
- Add missing treating wages to payroll.
- Do not mix clinician pay with distributions.
- Fill schedules before hiring more staff.
- Track each provider’s monthly capacity.
Are vestibular tests profitable for a dizziness clinic?
Vestibular tests can be profitable for a Dizziness and Balance Disorder Clinic, but only when test volume, payer collections, and clinician utilization stay high; see What Are The 5 Core KPIs For Dizziness And Balance Disorder Clinic? for the core operating metrics. Using the supplied capacity, first-year audiology revenue is about $546k/month and neurotology revenue is about $180k/month, but diagnostic consumables still run at 30% of revenue in year one, so profit comes down to how tightly the clinic uses its equipment and staff.
Profit drivers
- Volume has to stay high.
- Collections decide cash flow.
- Utilization drives revenue per provider.
- Services should match clinical need.
Cost anchors
- VNG starts at $65k.
- Posturography starts at $120k.
- Rotary chair starts at $85k.
- VEMP starts at $25k.
Want the six income drivers?
1
$1.4M-$7.0MPatient demand
More encounter volume is the biggest income swing, because revenue grows from $1.4M in Year 1 to $7.0M in Year 5 as schedules fill.
2
6xService mix
Shifting more visits toward higher-priced services lifts blended revenue, since treatment prices run from $85 to $510.
3
50%-85%Provider utilization
Higher capacity use turns the same staff base into more income, with key specialties moving from 50%-65% at launch to 80%-85% later.
4
6%-5%Billing collections
Tighter medical billing and revenue cycle work keeps more cash, because that cost falls from 6.0% of revenue to 5.0% by Year 5.
5
$261KOverhead control
Fixed overhead runs about $261K a year, so lease, software, insurance, and admin spend hit EBITDA directly.
6
$614KCash discipline
Minimum cash dips to $614K in Month 2, so profit is not the same as cash available for owner distributions.
Dizziness and Balance Disorder Clinic Core Six Income Drivers
Patient Demand and Referrals
Referral Flow and Filled Visits
Income here comes from filled visits and tests, not website traffic alone. In year one, the model shows 898 monthly billable encounters; in a mature year it reaches 4,078. If referrals from primary care, ENT, neurology, audiology, urgent care, and local awareness slow down, the clinic leaves audiologists, therapists, and neurotologists below capacity and loses revenue right away.
That matters because the overhead keeps running. With $217k/month of fixed overhead, every empty slot lowers gross margin and owner pay. The quick test is billable encounters per referral source, plus no-show and conversion rates from consult to test. If those do not rise, profit can look fine on paper but cash for distributions shrinks.
Track Referrals That Turn Into Visits
Measure the funnel from referral to completed visit. Track referrals received, scheduled visits, and completed billable encounters by source. Keep primary care, ENT, neurology, audiology, urgent care, and local awareness separate so you can see which channel fills the calendar and which one only creates noise.
- Referrals by source
- Show rate and no-shows
- Tests per completed visit
- Filled slots by provider
Set weekly targets by provider type and watch underfill early. If audiologists, therapists, or neurotologists sit below planned capacity, push outreach to the top sources and rebook no-shows fast. Build a simple forecast from referral count × show rate × test conversion, then compare it to the 898 and 4,078 monthly volume marks.
1
Payer Mix and Collections
Payer Mix and Collections
This driver is the gap between billed charges and cash in the bank. It includes contracted rates, collection speed, denial rates, deductible balances, and the cash-pay policy, so every payer shift changes average collected revenue per encounter. In year 1, billing and revenue cycle management (RCM) runs at 60% of revenue, then 50% in a mature year.
Here’s the quick math: if the clinic shows profit but claims sit unpaid, owner draws can stall. Slow collections can block distributions even when the income statement looks healthy, because payroll, rent, and supplies still need cash. Don’t treat any reimbursement value as guaranteed; model only what you reliably collect, not what the payer says it may owe.
Track collected cash, not billed charges
Measure collected revenue per encounter, not just charge volume. Split it by payer, then track denial rate, days to collect, patient responsibility, and cash-pay share. If a payer mix change lowers net collection rate, it should flow straight into your forecast and owner pay model. One bad payer shift can shrink cash without changing visit count.
Keep a short list in review each month: payer mix, denials, deductibles, cash-pay collections, and RCM cost as a percent of revenue. Tighten front-end eligibility checks, collect patient balances at service, and rework denial follow-up fast. If collections lag, cut distributions first, not patient care.
- Track net collected revenue per encounter.
- Watch denial rate by payer.
- Collect deductibles before service.
- Review A/R aging weekly.
2
Diagnostic and Treatment Service Mix
Service Mix and Visit Pricing
This driver is the split between evaluation visits, vestibular testing, canalith repositioning, follow-ups, and therapy visits. Revenue rises when more encounters land in the higher-priced slots: $450 for neurotologists, $350 for vestibular audiologists, $175 for vestibular physical therapists, $160 for occupational therapists, and $85 for rehabilitation assistants.
Here’s the quick math: the same patient can produce very different revenue depending on test depth and visit mix. More testing usually lifts revenue per patient, but it also adds consumables and equipment wear, so gross margin can slip if the clinic overuses high-cost diagnostics. Clinical need has to drive the plan, or owner pay gets distorted by waste.
Track Revenue by Visit Type
Measure revenue per encounter by role and by service line. Use a simple dashboard with visit count, price, payer collection rate, and direct test cost. That shows whether a $450 neurotology visit is really worth more than a lower-priced follow-up once consumables, labor time, and denials are in the picture.
Then test the mix, not just volume. If higher-value testing fills the schedule, protect margins by tracking supply use, equipment downtime, and repeat-visit rates. A clean one-liner: better mix beats more visits only when the margin holds. Document when testing is medically needed, so revenue growth stays defensible and cash flow stays predictable.
- Count encounters by service type
- Track collected revenue, not charges
- Separate testing cost from visit cost
- Watch repeat visits after diagnosis
- Review equipment wear monthly
3
Staffing and Provider Utilization
Staffing Load and Fill Rate
This driver is the gap between staffed capacity and billed care. In year one, supplied capacity is 65% for vestibular audiologists, 60% for vestibular physical therapists, and 50% for neurotologists; mature year rises to 85%, 85%, and 80%. With payroll at about $464k in year one and $658k in mature year, empty schedule slots still carry labor cost and cut owner profit.
Owner pay depends on how much of that payroll turns into billable encounters. If the owner also treats patients, that wage is compensation, not pure equity profit, so take-home income is lower than the clinic’s margin suggests. More filled hours spread the same labor across more visits; low fill rate leaves you paying for idle time.
Measure Hours, Not Just Headcount
Track scheduled hours, billed hours, and paid labor by provider type each week. The key test is whether vestibular audiology, physical therapy, and neurotology are moving toward 85%, 85%, and 80% capacity, not just whether the team is fully staffed.
When utilization slips, cut open blocks, tighten referral handoffs, or shift work to the right provider. Separate owner clinical wages from ownership draw in the forecast, so cash flow, margin, and distributions stay clear.
4
Fixed Overhead and Equipment
Fixed Overhead
If your clinic can’t cover fixed costs, owner pay gets squeezed fast. This model puts monthly overhead at $217k, driven by a $125k facility lease, $18k software, $32k liability insurance, $11k utilities, $25k maintenance, and $600 supplies, plus calibration and equipment upkeep. Higher overhead raises the visit volume needed before profit becomes take-home income.
Track Fixed Cost Per Month
Measure fixed overhead as a clean monthly run rate, then compare it with billed encounters and collected revenue. The one-time $490k equipment capex also matters because it ties up cash before the clinic pays the owner. Keep lease, software, insurance, maintenance, and calibration in separate lines so you can spot cost creep early and protect distributions.
5
Cash Flow, Reserves, and Distributions
Cash Flow and Owner Draw
Cash flow here is what stays after cancellations, no-shows, and billing lag slow receipts, then payroll, debt, marketing reinvestment, and equipment replacement take their share. A clinic can show $886k of first-year operating profit and still have only about $396k of cash after the $490k startup spend, before taxes and reserves.
That means profit is not distributable cash. Owner pay should wait until payroll, claims timing, and replacement reserves are covered, or the draw can force short-term borrowing even in a profitable year.
Protect Cash Before Draws
Track cash weekly, not just monthly. Use three buckets: payroll, claims in transit, and replacement reserve. The owner can only safely draw from cash left after those buckets are covered, plus any debt payment and planned marketing spend.
- Watch cancellations and no-shows.
- Measure days from service to cash.
- Set aside equipment replacement reserves.
- Hold back draws until reserves are funded.
If collections lag or visits are canceled, cut the distribution first, not payroll or core clinical spend. That keeps the clinic stable and protects future owner income.
6
Low, base, and high owner-income scenario objective
Owner income scenarios
Owner income swings with referral flow, therapist utilization, payer mix, and staffing completeness. Even small volume gaps change how much cash is left after operating costs.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | This is the lower-earnings path at first-year scale. | This is the modeled middle path at Year 3 scale. | This is the stronger-earnings path at mature Year 5 scale. |
| Typical setup | Year 1 reaches $1.4M revenue and $605k EBITDA with 2 vestibular audiologists, 3 vestibular physical therapists, 1 neurotologist, 1 occupational therapist, and 2 rehabilitation assistants. | Year 3 reaches $4.056M revenue and $2.719M EBITDA with 4 vestibular audiologists, 6 vestibular physical therapists, 2 neurotologists, 2 occupational therapists, and 4 rehabilitation assistants. | Year 5 reaches $6.968M revenue and $5.172M EBITDA with 6 vestibular audiologists, 10 vestibular physical therapists, 2 neurotologists, 3 occupational therapists, and 6 rehabilitation assistants. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $605kConservative take-home | $2.719MCore take-home | $5.172MUpside take-home |
| Best fit | Use this to stress-test slower referral flow or a softer ramp. | Use this as the core operating case for budget planning. | Use this to test full referral density and strong clinic throughput. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distribution amounts.
Related Products
- Dizziness and Balance Disorder Clinic Porter's Five Forces Analysis
- Dizziness and Balance Disorder Clinic BCG Matrix
- Dizziness and Balance Disorder Clinic Business Model Canvas
- What Are The 5 Core KPIs For Dizziness And Balance Disorder Clinic?
- Dizziness and Balance Disorder Clinic Business Plan Template in Pre-Written Word
- How Increase Dizziness And Balance Disorder Clinic Profitability?
- What Are Operating Costs For Dizziness And Balance Disorder Clinic?
- Dizziness and Balance Disorder Clinic Startup Costs: $614K Cash Need
- Dizziness and Balance Clinic Financial Model Template in Excel
- How To Open A Dizziness And Balance Disorder Clinic In 4–9 Months
- How To Write A Business Plan For Dizziness And Balance Disorder Clinic?
- Dizziness and Balance Disorder Clinic Marketing Mix
- Dizziness and Balance Disorder Clinic Marketing Plan
- Dizziness and Balance Disorder Clinic Business Proposal
- Dizziness and Balance Disorder Clinic PESTEL Analysis
- Dizziness And Balance Clinic Pitch Deck Example Editable PPTX
- Dizziness and Balance Disorder Clinic Business SWOT Analysis
- Dizziness and Balance Disorder Clinic Value Proposition Canvas
Frequently Asked Questions
Under the supplied assumptions, first-year revenue is about $1647k per month, or about $20M annually Mature-year revenue reaches about $7552k per month, or about $91M annually Those numbers depend on provider count, treatment volume, treatment price, and capacity assumptions holding in practice