 Owner income$23.0M–$133.4M
Owner income$23.0M–$133.4MHow Much Does an Emergency Medical Service Owner Make on $281M Revenue?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$23.0M–$133.4M  Net margin8.2%–8.8%
Net margin8.2%–8.8% Revenue for target pay$281M
Revenue for target pay$281M Business difficultyHard
Business difficultyHard


An emergency medical service owner’s income is not a guaranteed salary Under the researched assumptions, the business produces $281M in first-year revenue and about $232M in operating profit before owner pay, debt service, taxes, and reserves That is an 827% pre-reserve margin, but take-home depends on collections, fleet uptime, payer mix, payroll coverage, and how much cash the owner keeps inside the business In a mature-year scenario, modeled revenue reaches $1514M with $1340M before owner pay and reserves
Owner income$23.0M–$133.4MNet margin8.2%–8.8%Revenue for target pay$281MBusiness difficultyHardWant to test your EMS owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Emergency Medical Service model?
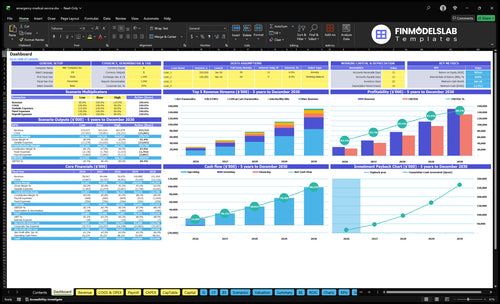
This dashboard shows revenue, margin, costs, reserves, and owner pay; open the Emergency Medical Service Financial Model Template to see staffing, reimbursement prices, capacity ramp, COGS, variable costs, fixed overhead, and wages. It lays out $281M first-year revenue, $1,514M mature-year revenue, 900% to 920% gross margin, and $232M to $1,340M EBITDA before owner pay.
Owner-income model highlights
- Owner pay scenarios
- Revenue and margin
- Overhead and reserves
How much revenue does an ambulance service need?
For an Emergency Medical Service, the revenue target is not a fixed number; start with target owner pay + reserves + debt service, then divide by the first-year operating margin. In this model, $10M collected produces about $827k before owner pay, reserves, taxes, and debt, so booked revenue is not the same as cash. Billing lag and denied claims can block distributions even when profit looks strong.
Quick math
- Start with owner pay need.
- Add reserves and debt service.
- Divide by operating margin.
- $10M collected = $827k pre-reserve.
Cash timing
- Booked revenue is not cash.
- Billing lag slows collections.
- Denied claims can block payouts.
- Distributions can wait on cash.
What profit margin can an ambulance service make?
An Emergency Medical Service can show a modeled 900% first-year gross margin after direct supplies and vehicle costs, then 827% operating profit before owner pay, debt, taxes, and reserves. For startup cost context, see How Much Does It Cost To Open And Launch Your Emergency Medical Service Business?. The big swing items are crew overtime, fuel, maintenance, insurance, billing denials, and payer reimbursement mix.
Margin math
- 900% first-year gross margin
- 827% operating profit before owner pay
- 100% direct COGS in year one
- 50% variable billing and overtime costs
Cost pressure points
- $3,564k fixed overhead
- $2,800k listed wages
- Crew overtime can cut margin fast
- Fuel, maintenance, and insurance matter
How does the EMS owner role affect income?
If you run an Emergency Medical Service business yourself, your income is higher early on because you can cover operations, dispatch oversight, payer follow-up, and fleet coordination instead of paying managers. A scaled owner usually takes lower short-term take-home to build cleaner systems, and this model already includes $900k for an Operations Manager, $750k for a Fleet and Logistics Manager, $600k for Billing and Collections, and $550k for HR and administration.
Hands-on owner
- Protects early cash flow
- Covers dispatch and ops
- Chases payer follow-up
- Coordinates fleet use
Scaled owner
- Takes lower short-term pay
- Funds manager payroll
- Builds cleaner systems
- Needs more compliance reserves
Want the six EMS income drivers?
1
395-445/moRun Volume
More billable encounters spread the fixed base fast, and the plan grows from about 395 to 445 per month across the forecast.
2
3%-2%Collections
Billing fees move from 3.0% to 2.0%, so cleaner claims keep more cash in the business.
3
2%-1%Overtime
Contracted overtime drops from 2.0% to 1.0%, which protects margin when demand spikes.
4
4%-3%Fleet Uptime
Direct fuel and maintenance cost falls from 4.0% to 3.0%, so more of each run stays as take-home.
5
$64K/moFixed Overhead
Year 1 fixed costs and base wages run near $64K a month, so weak dispatch volume will crush profit fast.
6
$1.18MCash Reserve
The model needs about $1.18M of minimum cash, so owner distributions should wait until that buffer is in place.
Emergency Medical Service Core Six Income Drivers
Transport Volume and Fleet Utilization
Billable Transports per Staffed Unit
Owner income starts when each staffed unit produces enough billable transports to cover crew time, fuel, supplies, dispatch, and vehicle downtime. The model lists first-year monthly encounters at 1,7225 and mature-year volume at 8,264, across ALS, BLS, interfacility, event, and critical care runs. More calls only help if reimbursement is actually collected.
Here’s the quick math: volume raises gross revenue, but every run also adds labor coverage and fleet use. If crews sit idle, revenue stalls; if vehicles sit down, billable capacity falls. The real owner-pay test is not “How many calls?” but “How many paid calls per staffed unit after direct variable costs and overhead?” Busy isn’t profitable; paid transport density is.
Track Fleet Uptime and Paid Run Rate
Measure billable transports per staffed unit, not dispatches alone. Pair that with collected revenue per call, crew coverage, fuel, supplies, and available vehicles so you can see which line is creating cash and which one is just activity.
- Track paid runs by service line.
- Watch vehicle downtime daily.
- Compare collections to call volume.
If volume rises but collections lag or ambulances are offline, owner income drops fast. The model shows capacity moving from 500% to 900% by service line and year, so the gain comes from tighter utilization, faster billing, and fewer missed transports. If the truck is busy but unpaid, the owner still loses.
1
Payer Mix and Billing Collections
Payer Mix and Collections
Ambulance charges do not equal cash. Here, payer mix means how much volume comes from Medicare, Medicaid, private insurance, and patient balances, plus how fast each pays. Modeled service prices run from $700 for first-year interfacility RN service to $3,400 for mature-year critical care paramedic service, but billing and collections fees still take 30% of revenue in year 1 and 20% in the mature year.
That means take-home income can change faster from denials, write-offs, and slow claims than from call volume alone. Here’s the quick math: at 30% collections cost, every $100 billed starts as about $70 before bad debt and cash lag; at 20%, it’s about $80. If payer mix shifts toward slower or lower-paying claims, owner pay can fall even when transports rise.
Track Denials and Cash Lag
Measure collections by service line, not just total revenue. Track billed charge, collected cash, denial rate, write-off rate, and days in accounts receivable (A/R, money owed but not yet collected). The key inputs are transport type, payer type, payment speed, and patient balance. Without that split, you can overstate profit and understate the cash needed to pay crews, fuel, and overhead.
Use a simple weekly dashboard: Medicare, Medicaid, private insurance, and self-pay; billed amount versus cash collected; and fees at 30% in year 1 or 20% in the mature year. If denials rise or patient balances stretch, tighten documentation, verify coverage before transport when possible, and forecast owner draws from collected cash, not charges.
- Split revenue by payer.
- Track denials every week.
- Watch days in A/R.
- Forecast on collected cash.
2
Staffing and Overtime
Staffing and Overtime
Here, the math is simple: payroll only helps owner income when staffing keeps pace with billable runs. First-year management and admin wages total $2.8M, rising to $4.0M in the mature year. Contracted overtime and per-diem costs start at 20% of revenue and fall to 10% as capacity moves from 10 ALS Paramedics and 8 BLS EMTs to 30 and 25.
If labor is short, added transports just add wage pressure and can squeeze take-home pay. If the crew mix is built ahead of demand, the business can spread payroll over more billed calls and keep more cash after labor. The key risk is simple: overtime that stays near 20% can erase the gain from growth.
Cut Overtime First
Track base pay, overtime, and per-diem by service line: ALS, BLS, interfacility, event, and critical care. Use staffed hours, call peaks, and active headcount to test whether each added transport pays for the crew needed to cover it. The core inputs are 10 to 30 ALS Paramedics, 8 to 25 BLS EMTs, and the share of labor tied to overtime.
- Watch overtime hours every week.
- Separate per-diem from base wages.
- Staff to peak demand, not averages.
- Test crew mix by call type.
When overtime falls from 20% to 10% of revenue, more cash is left for overhead, debt, and owner draws. If schedules stay thin or onboarding is slow, the model turns into a labor-heavy transport shop instead of a profit driver.
3
Fleet Costs and Uptime
Fleet Costs and Uptime
Fleet costs hit both margin and capacity. In year one, direct fuel and vehicle maintenance run at 40% of revenue; in the mature year, they still take 30%. Add fleet vehicle insurance at $30,000 per month or $360,000 per year, and the business has to keep a tight grip on every mile, repair, and vehicle payment before owner pay is safe.
Downtime cuts twice. Repairs use cash, and an out-of-service ambulance cannot complete a billable transport. Track repairs, preventive maintenance, fuel, equipment replacement, vehicle payments, and missed-call revenue together, or the true hit to cash flow will look smaller than it is. One idle unit can hurt both revenue and response speed at the same time.
Measure uptime by unit, not just by month
Use one daily log for each ambulance: miles, fuel spend, repair days, and preventive maintenance. Then compare that with completed transports and missed calls, so you can see the real cost of lost capacity. Here’s the key test: if downtime rises, owner income falls even when booked calls look fine.
- Track cost per active ambulance.
- Log repairs and service dates.
- Match downtime to lost transports.
- Watch insurance and payment timing.
Set a replacement trigger before breakdowns pile up. If one vehicle is draining cash through repairs and missed transports, it can drag gross margin below the level needed to cover fixed overhead and still leave a distributable profit.
4
Insurance, Licensing, and Overhead
Fixed EMS Overhead
Fixed overhead is the burn that has to be covered before owner pay. At $297k per month, this layer equals $3.564M per year. The listed items total $272k monthly, so $25k is left for licensing, medical director oversight, compliance systems, workers compensation, and billing admin. If collections miss plan, distributions drop fast.
This cost base includes $150k rent, $35k dispatch software, $25k liability insurance, $30k fleet insurance, $12k legal and accounting, and $20k marketing. Here’s the quick math: every $10k cut in fixed overhead adds $120k a year to cash available for debt, reserves, or owner draw. The catch is that these expenses keep running even when call volume dips.
Track Overhead Run Rate
Measure fixed overhead as a share of collected revenue, not billed charges. Build a monthly rollup for rent, software, insurance, legal, marketing, licensing, medical director oversight, compliance, workers compensation, and billing admin. If the run rate stays near $297k, owner pay depends on volume and collections, not just more ambulances on the road.
- Rent and lease resets
- Insurance renewal dates
- Licenses and medical director fees
- Billing admin headcount
- Compliance software seats
Use a 90-day budget and renewals calendar. The inputs that matter most are facility count, software seats, insurance premiums, licensing fees, medical director terms, and billing admin workload. Cut waste only where it doesn’t slow dispatch or compliance.
5
Reserves, Debt Service, and Reinvestment
Reserves and Debt Service
Accounting profit is not the same as owner take-home. The model shows $232M first-year operating profit before owner pay, but reserve percentage and debt service are not provided, so distributable cash is still unknown. In EMS, cash has to cover billing delays, unpaid claims, fleet replacement, equipment, compliance, and loan payments before any draw.
If claims lag or debt service rises, owner pay drops fast even when profit looks strong. A business with $297k in monthly fixed overhead cannot pull cash out early and stay safe. Pay yourself after payroll, insurance, repairs, and reimbursement lag are covered, not before.
Track Cash Before Owner Pay
Build the cash rule first. Set a reserve target in months of cash, not just dollars. Track monthly claims aging, denial rate, debt service, fleet replacement timing, and compliance spend. If cash cannot cover fixed outflows and delayed collections, owner distributions stop.
- Monthly loan payments
- Claims lag and denials
- Reserve target in months
- Vehicle replacement schedule
- Repair and compliance spend
Reinvest before you draw. If ambulances, equipment, or compliance systems need cash now, reinvestment protects future billing and uptime. That keeps take-home pay steadier than taking a large distribution after one strong month.
6
Compare low, base, and high EMS owner-income scenarios
Owner income scenarios
Owner take-home changes with volume, staffing, and debt service. These cases show how much cash can be left after core operating costs at low, base, and high run rates.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | This is the lower owner-income path if first-year demand comes in light. | This is the modeled owner-income path if the business tracks the Year 3 run rate. | This is the stronger owner-income path if the mature-year run rate holds. |
| Typical setup | The model stays near first-year assumptions, with $281M revenue and about $232M before owner pay before reserves and debt service. | The plan reaches $767M revenue and about $660M before owner pay as staffing, billing, and capacity follow the model. | The mature model reaches $1.514B revenue and about $1.34B before owner pay with higher capacity use and tighter collections. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $232M pre-owner payLow Case | $660M pre-owner payBase Case | $1.34B pre-owner payHigh Case |
| Best fit | Use this to stress-test a slow launch and see if reserves still support owner pay. | Use this for a steady operating plan that assumes the business scales as forecast. | Use this to test upside if demand, staffing, and collections all stay on track. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Emergency Medical Service Porter's Five Forces Analysis
- Emergency Medical Service BCG Matrix
- Emergency Medical Service Business Model Canvas
- 7 Critical KPIs for Emergency Medical Service Success
- Emergency Medical Service Business Plan Template in Pre-Written Word
- Increase Emergency Medical Service Profitability: 7 Key Strategies
- How to Budget Monthly Running Costs for an Emergency Medical Service
- Emergency Medical Service Startup Costs: $145M Before Opening
- Emergency Medical Service Financial Model Template in Excel
- How To Open An Emergency Medical Service In 6 To 18 Months
- How to Write an Emergency Medical Service Business Plan
- Emergency Medical Service Marketing Mix
- Emergency Medical Service Marketing Plan
- Emergency Medical Service Business Proposal
- Emergency Medical Service PESTEL Analysis
- Emergency Medical Service Pitch Deck Example Editable PPTX
- Emergency Medical Service Business SWOT Analysis
- Emergency Medical Service Value Proposition Canvas
Frequently Asked Questions
Under the researched assumptions, the first-year cash pool before owner pay, debt, taxes, and reserves is $232M on $281M revenue That is not guaranteed take-home The owner still needs to fund working capital, fleet replacement, debt service, compliance, and delayed collections before taking distributions