 Time to Open6-12 monthsSetup window
Time to Open6-12 monthsSetup windowHow To Open A US FUE Hair Clinic In 6 To 12 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open6-12 monthsSetup window  Launch Sequence6 stagesMedical first
Launch Sequence6 stagesMedical first Key BottleneckLicense gateState rules
Key BottleneckLicense gateState rules First Revenue StepPaid consultsBooking live
First Revenue StepPaid consultsBooking live


Key Takeaways
- Medical governance must clear before deposits or ads.
- Room readiness drives safe, compliant daily throughput.
- Equipment and trained staff must arrive together.
- Break-even is about $80,962 monthly before taxes.
Time to Open6-12 monthsSetup windowLaunch Sequence6 stagesMedical firstKey BottleneckLicense gateState rulesFirst Revenue StepPaid consultsBooking liveLaunch timeline
Short web summary of the launch plan; the XLSX export carries the detailed Gantt chart and task logic.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Governance
- License checklist
- Malpractice bound
- SOP draft
- Accreditation prep
Buildout
- Lease setup
- Floor plan
- Buildout work
- Compliance walk
- Lounge setup
Equipment
- FUE system order
- Imaging hardware
- Sterile kits stock
- Microscopes install
- Backup systems install
Staffing
- Surgeon recruiting
- Nurse hiring
- Front desk hire
- Procedure training
- Mock day drills
Marketing
- Positioning review
- Lead channels live
- Consult scripts
- Booking flow
- Follow-up sequence
Systems
- Records setup
- Consent forms
- Billing flow
- Dry run clinics
- Launch gate review
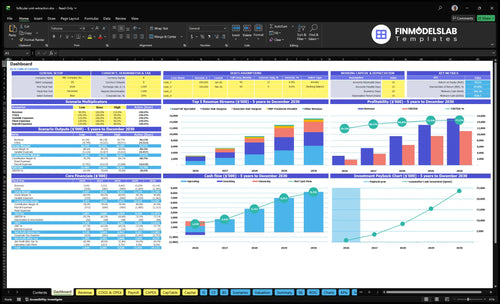
Does the launch model still break even after delays?
Yes. At Year 1 capacity, the clinic still clears break-even; delays mainly tighten runway. The screenshot shows revenue, costs, cash needs, assumptions, and break-even logic—open the Follicular Unit Extraction Hair Clinic Financial Model Template.
Financial model highlights
- $570,000 setup spend
- $253,475 monthly revenue
- 22% variable load
- $63,150 fixed overhead
What are the biggest mistakes when opening an FUE clinic?
The biggest mistakes when opening a Follicular Unit Extraction Hair Clinic are starting before graft handling is repeatable, treating compliance like paperwork, and hiring for full capacity too early. In Year 1, payroll can run about $41,250 a month plus $21,900 in fixed overhead, so weak demand or poor consult-to-procedure conversion gets expensive fast. If the first 10 patients hit process gaps, reviews and referrals can suffer before you have enough volume to recover.
Big launch mistakes
- Do not open with inconsistent graft handling.
- Do not skip patient financing workflow.
- Do not underbuild consult-to-procedure conversion.
- Do not buy capacity before trained staff.
Readiness checks
- Run live consult simulations first.
- Walk through procedure rooms in real time.
- Check sterile kits and local anesthesia supply.
- Test consent, escalation, and follow-up scripts.
How do you get first patients for an FUE hair clinic?
The first patients for a Follicular Unit Extraction Hair Clinic come from pre-opening consultations, not opening-week ads alone, so the clinic should build demand before day one; see How To Write A Business Plan For Follicular Unit Extraction Hair Clinic? for the launch order. The first revenue step is a paid consultation or deposit for a scheduled FUE procedure, but only after medical governance, consent, financing disclosures, and procedure dates are ready. In Year 1, the funnel can support $12,500 senior surgeon FUE, $7,500 lead FUE specialist procedures, $800 platelet-rich plasma, and $1,200 scalp micropigmentation, with 8% of revenue for digital marketing and lead acquisition plus 3% for financing referral commissions.
Start before launch
- Set up local search first
- Test paid search for consults
- Push financing in booking flow
- Plan ethical before-after rules
Convert booked leads
- Screen eligibility before scheduling
- Collect deposits on qualified leads
- Close only with consent complete
- Track revenue by procedure date
How long does it take to open a hair transplant clinic?
A Follicular Unit Extraction Hair Clinic usually takes 6 to 12 months to open, and the pace depends on lease choice, medical governance, room buildout, equipment delivery, training, malpractice coverage, inspections, and testing. Here’s the quick math: the schedule often runs from Month 1 to Month 10 for key build items, so a late permit or physician sign-off can push launch past the planned window.
Main timing drivers
- Lease and room design set the pace
- Physician sign-off can delay launch
- Permits and inspections add weeks
- Equipment lead times often run months
Go-live sequence
- Lock medical governance first
- Confirm state rules before spending
- Hire core staff, then test workflow
- Soft open after sterile flow works
Build a go/no-go checklist for opening an FUE clinic
Launch readiness checklist
Use this go-live approval checklist before opening the hair clinic.
Clinical governance
- Licensed physician oversight in placeCritical
A licensed overseer is needed before any transplant work starts.
- State board rules reviewedCritical
State medical rules drive who can perform each step.
- Corporate practice review completeCritical
This helps avoid ownership and control issues before launch.
- Malpractice coverage activeCritical
Coverage should be bound before any patient touchpoint.
Patient flow
- HIPAA safeguards configuredCritical
Protected patient data needs controls before consults begin.
- Procedure room infection control clearedCritical
Sterile room flow lowers infection risk during surgery.
- Photography and recovery rooms readyHigh
Images and recovery space support consults and post-op care.
- Patient flow and storage mappedHigh
Clear movement keeps patients, supplies, and staff from crossing paths.
Equipment
- FUE device ordered and testedCritical
The extraction system is the core tool for the main service.
- Surgical microscopes and lights readyHigh
Good visibility matters for graft handling and precision.
- Autoclave and fridge approvedCritical
Sterile tools and cold storage must work before the first case.
- Sterile kit reorder process setHigh
Low stock can stop procedures and delay booked patients.
Staffing
- Year one surgeon roster confirmedCritical
The model assumes one senior surgeon and one associate in Year 1.
- Lead FUE and nursing coverage setCritical
The Year 1 plan needs two FUE specialists and two nurses.
- Patient coordinator and front desk hiredHigh
These roles keep consults, calls, and follow-up moving.
- Clinical team training completedCritical
Staff need a shared process for graft handling and post-op care.
Demand
- Local search pages liveHigh
Search visibility is the first lead source for this clinic.
- Consult booking liveCritical
Prospects need a simple path from interest to consult.
- Deposits and follow-up scripts readyHigh
Scripts help convert consults and reduce no-shows.
Finance
- Year one cash runway checkedCritical
Minimum cash is $835k, with Month 1 as the tightest point.
- Model covers monthly overheadCritical
Year 1 monthly revenue capacity is about $253,475 before costs.
- Go-live signoff completedCritical
No launch should start without compliance, staff, and cash signoff.
Which six drivers decide launch readiness?
1Medical Governance
License gateSigned governance docs, a named supervising physician, malpractice coverage, and scope rules must be in place before ads, deposits, or procedure booking can start.
2Facility Readiness
Month 1-10The procedure room, sanitation flow, recovery space, photography area, and waste setup have to work inside the Month 1 to Month 10 buildout window or throughput slips.
3FUE Equipment
$335KInstalled extraction, imaging, sterilization, and storage gear keeps procedure capacity aligned with the booking calendar, but vendors and maintenance must land on time.
4Clinical Team
Trained teamThe Year 1 team has to run intake, graft handling, sterile turnover, and handoffs without confusion, or cancellations and first-review quality drop.
5Patient Funnel
$253K/moLive consult pages, financing, deposit flow, and lead tracking must turn the modeled Year 1 monthly revenue capacity into booked procedures before opening.
6Operating Systems
$81KEMR, consent, inventory, and follow-up systems have to match about $63.15K in monthly wages plus $21.9K in fixed overhead, with break-even near $80.96K before financing and taxes.
Medical Governance
Medical Governance
For an FUE hair clinic, medical governance is the gate that decides whether you can open on time. You need a named supervising physician, active malpractice coverage, signed scope-of-practice rules, and documented escalation steps before you take deposits or book procedures.
If a non-doctor founder signs the lease and starts ads first, the launch can stall when counsel or the state medical board flags the structure. This work also covers healthcare counsel review, state board checks, ownership setup, provider credential files, informed consent, privacy policies, and OSHA training.
Launch Checklist
Start with the legal order, then move to marketing. Do not publish clinical claims, collect deposits, or schedule procedures until the governance packet is signed and the supervising physician is on file. That keeps the opening from slipping because of a late compliance fix.
Here’s the quick sequence: counsel review, state medical board check, ownership structure, credential files, consent forms, privacy policies, malpractice policy, OSHA training, and a documented clinical escalation process. One clean one-liner: if the paperwork is late, the opening date slips.
- Named supervising physician confirmed
- Malpractice policy active
- Scope rules reviewed
- Consent forms ready
- OSHA training complete
1
Facility And Procedure Room Readiness
Procedure Room Ready
A FUE clinic cannot open on time if the procedure room is not ready for sanitation, lighting, sterile supply storage, recovery space, photography, and clinical waste disposal. This room drives patient safety and how fast the team can move from consult to procedure, so it is a day-one operating issue, not just a construction task.
The buildout runs from Month 1 to Month 5, while the patient lounge starts in Month 4 to Month 10. That means the clinic must lock lease terms, permits, contractor timing, equipment dimensions, and sterilization placement early. A beautiful room that misses infection control or flow rules can still delay opening and create first-day bottlenecks.
Mock the Workflow
Map the room before furniture arrives. Verify the room layout, lighting plan, storage map, emergency supplies, and recovery chair path against the actual equipment footprint, then confirm the waste vendor and sterilization workflow before any install is final.
- Place photography station before final wiring.
- Test clean-to-dirty patient flow.
- Run a mock procedure walk-through.
- Fix waste pickup before first case.
A mock procedure walk-through should prove that staff can move a patient, instruments, photos, recovery, and waste without crossing paths. If the room works on paper but not in motion, opening-day schedule slips, turnover slows, and the first procedures take longer than planned.
2
FUE Equipment And Supplies
FUE Equipment Readiness
For an FUE hair clinic, equipment is a launch gate, not a nice-to-have. The business cannot open on time or serve the booking calendar from day one unless the FUE extraction system, microscopes or graft handling tools, operating lights, sterilization process, medical fridges, local anesthesia supplies, sterile kits, and digital imaging are installed and working.
Here’s the quick math: core capex is about $335,000, made up of a $250,000 surgical system, $45,000 for microscopes and operating lights, $25,000 for an autoclave and fridges, and $15,000 for imaging hardware. Year 1 also carries 65% of revenue for consumables and sterile kits plus 45% for technology royalty and maintenance fees, so supply timing directly affects cash needs.
Lock the install before booking volume
Verify vendor delivery dates, maintenance agreements, and sterile supply availability before you open consult slots. If equipment arrives before protocols or staff competency, the clinic looks ready on paper but still misses procedures in practice. The real readiness signal is a tested setup with a reorder system, not just boxes in the room.
- Confirm delivery and installation dates.
- Test sterilization before first patient.
- Train staff on each device.
- Document reorders for sterile kits.
- Check local anesthesia inventory levels.
Do a full mock procedure after setup. That tells you whether the lights, imaging, storage, and turnover flow support the day-one schedule, or whether the calendar is ahead of the clinic’s true capacity.
3
Trained Clinical Team
Trained Clinical Team
This clinic can’t open on time if the team is still learning on the job. FUE depends on graft survival workflow, patient safety, and fast room turnover, so weak training slows every procedure and can damage first reviews. The Year 1 provider plan needs 1 senior hair surgeon, 2 lead FUE specialists, 1 platelet-rich plasma provider, and 1 scalp micropigmentation technician.
The readiness signal is a crew that can handle intake, hairline planning support, extraction setup, graft handling, implantation support, sterile turnover, recovery, and follow-up without confusion. If hiring stops at resumes and never reaches drills, day-one capacity drops, cancellations rise, and consult conversion suffers. That also creates uneven post-op care, which is hard to fix once patients start comparing outcomes.
Train the workflow before the first booking
Hire for repeatable roles, then test the handoff chain. The Year 1 staff plan needs 1 clinic director, 1 senior patient coordinator, 2 registered nurses, 1 front desk receptionist, and 1 marketing manager. Before opening, run competency checks, mock procedures, and documentation drills so each person knows the next step, the escalation path, and the patient script.
Use one launch test: can the team move one patient from consult to recovery with no confusion? Review emergency protocol, sterile turnover, and patient handoff scripts before the first booking. If training slips by even a few days, opening may still happen, but safe, steady day-one throughput gets shaky fast.
4
Consultation And Patient Acquisition Funnel
Consultation Funnel Readiness
If the consultation funnel is weak, the clinic can still open on paper but miss first revenue and day-one utilization. This driver covers local SEO, paid search tests, booking flow, financing, deposits, reviews, and approved before-and-after content, so it has to be live before soft opening.
Here’s the quick math: marketing and lead acquisition are assumed at 8% of Year 1 revenue, plus 3% for medical financing referral commissions. That spend only works if the clinic can accept consults, screen eligibility, collect deposits, and move approved patients into the procedure calendar without delays.
Build The Booking Path First
Start with the pieces that turn interest into booked consults: landing pages, call scripts, eligibility checks, photography consent, financing disclosures, deposit workflow, and no-show follow-up. One clean path matters more than more ad spend.
- Test local SEO before ads.
- Set deposit rules in writing.
- Train staff on financing handoffs.
- Approve before-and-after use upfront.
The bottleneck is buying leads before the clinical calendar and financing path are ready. That creates wasted spend, slow conversion, and a weak opening signal even if demand is there.
5
Operating Systems And Financial Ramp Validation
Operating Systems And Ramp Validation
If bookings, records, staffing, cash, and procedure capacity are not in sync, you can open late or open underbooked. This launch driver is the day-one check that the clinic can take consults, track deposits, confirm financing, and run procedures without gaps in the schedule or the charting process.
Here’s the quick math: fixed monthly overhead is $21,900 before payroll, and Year 1 payroll adds about $41,250 per month, so total fixed cost is about $63,150. With a 22% variable load, break-even revenue is roughly $80,962 per month, while modeled revenue at stated capacity is about $253,475. The risk is simple: if consult conversion is weak, procedure days stay open and cash gets tight.
Launch Readiness Checks
Before opening, verify the operating stack is live: EMR (electronic medical records), patient relationship management software, consent templates, photography workflow, deposit tracking, financing status, procedure schedule, inventory log, and post-op follow-up tasks. If any one of these is manual or missing, day-one throughput slows and patient handoffs get messy.
Set the ramp plan against the calendar, not hope. Confirm how many consults must convert to fill procedure days, then test it against the $80,962 break-even point and the 78% contribution margin. Assign one owner to reconcile deposits, financing approvals, and schedule fill each day so you know whether the clinic is truly ready to start earning on time.
- Test EMR and charting before deposits.
- Lock consent and photo workflows.
- Reconcile schedule, inventory, and follow-ups daily.
- Track consult-to-procedure conversion weekly.
- Compare booked revenue to $80,962 break-even.
6
Related Products
- Follicular Unit Extraction Hair Clinic Porter's Five Forces Analysis
- Follicular Unit Extraction Hair Clinic BCG Matrix
- Follicular Unit Extraction Hair Clinic Business Model Canvas
- What Are The 5 KPIs For Follicular Unit Extraction Hair Clinic Business?
- Follicular Unit Extraction Hair Clinic Business Plan Template in Pre-Written Word
- How Increase Profits For Follicular Unit Extraction Hair Clinic?
- What Are Operating Costs For Follicular Unit Extraction Hair Clinic?
- FUE Hair Clinic Startup Costs: $835K First-Month Cash Plan
- Follicular Unit Extraction Hair Clinic Financial Model Template in Excel
- How Much Can a FUE Hair Clinic Owner Make at $253K/Month?
- How To Write A Business Plan For Follicular Unit Extraction Hair Clinic?
- Follicular Unit Extraction Hair Clinic Marketing Mix
- Follicular Unit Extraction Hair Clinic Marketing Plan
- Follicular Unit Extraction Hair Clinic Business Proposal
- Follicular Unit Extraction Hair Clinic PESTEL Analysis
- Follicular Unit Extraction Hair Clinic Pitch Deck Example Editable PPTX
- Follicular Unit Extraction Hair Clinic Business SWOT Analysis
- Follicular Unit Extraction Hair Clinic Value Proposition Canvas
Frequently Asked Questions
Start with medical governance before signing long-term commitments Confirm state ownership rules, physician oversight, malpractice coverage, and delegation limits first Then sequence the 6 to 12 month plan across lease, buildout, equipment, hiring, training, marketing, and soft opening In the researched model, Year 1 depends on 1 senior hair surgeon, 2 lead FUE specialists, and 2 registered nurses