 Owner income$1.94M-$11.21M
Owner income$1.94M-$11.21MHow Much Can a FUE Hair Clinic Owner Make at $253K/Month?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$1.94M-$11.21M  Net margin59%-73%
Net margin59%-73% Revenue for target pay$3.04M-$15.14M
Revenue for target pay$3.04M-$15.14M Business difficultyHard
Business difficultyHard


You’re estimating owner take-home from a Follicular Unit Extraction (FUE) hair clinic, not a guaranteed medical salary These researched planning assumptions show $253,475 in first-year monthly revenue, listed operating costs, payroll, marketing, reserves to plan for, and owner cash flow before personal taxes Adjust the numbers for your local market, surgeon model, financing, and clinic maturity
Owner income$1.94M-$11.21MNet margin59%-73%Revenue for target pay$3.04M-$15.14MBusiness difficultyHardWant to test your FUE clinic profit?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income depends on volume, pricing, staffing, debt, taxes, and reserve policy.
Want to see the FUE clinic model?
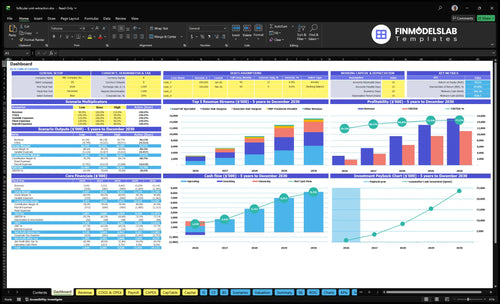
Open the Follicular Unit Extraction Hair Clinic Financial Model Template to see the dashboard, capacity, pricing, staffing, costs, debt, and owner pay.
Owner-income model highlights
- Revenue: $253,475 to $1,261,950
- EBITDA, payroll, fixed costs
- Scenario testing and reserves
Can a FUE clinic owner make money without being the surgeon?
Yes, a Follicular Unit Extraction Hair Clinic owner can make money without being the surgeon, but hired clinical labor cuts owner profit unless procedure price, volume, or utilization rises enough to cover it; see How Much To Launch A Follicular Unit Extraction Hair Clinic? for launch cost context. The model starts with 1 Senior Hair Surgeon in Year 1, adds Associate Hair Surgeons from Year 2, and reaches 2 Senior Hair Surgeons by mature year.
Profit pressure
- Pay surgeon compensation
- Add medical director fees
- Cover clinical supervision cost
- Protect per-procedure margin
Owner levers
- Raise utilization per practitioner
- Price for hired talent
- Know state licensing rules
- Serve adults aged 30 to 60
What is the profit margin of a FUE hair transplant clinic?
A Follicular Unit Extraction Hair Clinic should be planned with margins, not universal claims: the model points to a 780% first-year gross contribution after COGS and variable selling costs, and an EBITDA-style operating margin of about 531% after $21,900 monthly fixed overhead and $495,000 annual payroll. If you’re building the plan, start with How To Write A Business Plan For Follicular Unit Extraction Hair Clinic? so the pricing and capacity assumptions stay tied to the math. Margin can drop fast if surgeon pay, medical director fees, rework, low graft yield, ad waste, or debt service run higher than modeled.
Year 1 margin
- 780% gross contribution
- 65% consumables
- 45% FUE technology fees
- 80% digital marketing
Mature-year margin
- 818% contribution margin
- 734% EBITDA-style margin
- 30% financing commissions
- Higher costs can cut margin
How many FUE procedures per month pay the owner?
Follicular Unit Extraction Hair Clinic pays the owner at about 9 FUE procedures per month on first-year numbers, before debt, taxes, reserves, and any extra owner pay. Here’s the quick math: $63,150 in monthly fixed overhead plus payroll, and about $9,518 per case, gets you to roughly $80,962 in monthly break-even revenue. If the owner wants a salary or distributions on top, you need more than that.
Break-even math
- 9 FUE cases gets close to break-even.
- $80,962 monthly revenue covers fixed costs.
- $63,150 is first-year overhead plus payroll.
- $9,518 is average revenue per case.
What changes it
- Owner pay needs more volume or higher pricing.
- Cancelations raise the break-even point.
- Low consult conversion cuts monthly cases.
- Underused surgical days leave owner pay uncovered.
Want the six FUE clinic income drivers?
1
65%-85%Surgical Utilization
Moving senior surgeon capacity from 65% to 85% adds more billable cases without adding much fixed cost.
2
$12.5K-$14.5KCase Value
Raising case price from $12.5K to $14.5K, with Lead FUE Specialist pricing at $7.5K to $8.5K, lifts revenue on every procedure.
3
EditableConsult Conversion
This is the volume gate: more consults that turn into booked procedures drive revenue without new room count.
4
Owner-ledClinical Labor
An owner-surgeon model keeps more of each case in-house than a heavier hired-surgeon mix.
5
80%-60%Acquisition Cost
Marketing at 80% of revenue in year 1 and 60% in a mature year makes acquisition efficiency a direct cash driver.
6
$21.9K/moOverhead Reserve
Fixed overhead of $21.9K a month, plus payroll and reserves, can wipe out take-home before taxes and distributions.
Follicular Unit Extraction Hair Clinic Core Six Income Drivers
FUE procedure volume and surgical utilization
FUE Surgical Utilization
When most fixed costs are already committed, every extra booked case drops faster to profit. In year one, the model shows 15 treatments/month for the senior surgeon and 24 treatments/month for Lead FUE Specialists, so the real question is not demand alone, but how many consults turn into clean, on-time surgeries.
Here’s the quick math: mature volume rises to 255 booked cases/month for the senior surgeon and 612 booked cases/month for Lead FUE Specialists. That only helps owner income if the clinic can keep the consult pipeline, surgeon time, technician support, room slots, and cancellations in sync. Overbooking can lift short-term revenue, but it can also hurt outcomes, reviews, and rework.
Track Booked Cases, Not Just Leads
Use utilization as booked cases divided by available treatment slots. Track consults, show-rate, booked surgeries, cancellations, and rework by surgeon each month. If one step slips, cash flow slips too. One clean case is worth more than two rushed ones.
- Match bookings to surgeon hours
- Watch technician and room capacity
- Log cancellations by reason
- Hold quality before filling slots
For owner pay, the main lever is stable volume with low rework. If surgeon time is full but patient outcomes weaken, refunds, make-goods, and bad reviews can erase the margin from higher throughput. Keep the schedule tight, but leave room for proper pre-op review and post-op care.
1
Average FUE case value and pricing
Average FUE Case Value
Average FUE case value is the blended price per surgery. With senior surgeon pricing at $12,500 in Year 1, Lead FUE Specialist at $7,500, and Associate Hair Surgeon starting at $9,500 in Year 2, a richer case mix lifts revenue fast. That only helps owner income if consult conversion and utilization hold.
By the mature year, prices rise to $14,500, $8,500, and $11,000. Here’s the quick math: higher ticket size improves gross profit per booked case, but a softer close rate or fewer booked surgeries can wipe out the gain. Average case value should track surgeon type, graft count, and collected price.
Track Price Realization
Measure average selling price by surgeon and by graft band, plus booked versus collected revenue. The key inputs are consult conversion, utilization, financing approval, and case mix. If a higher price slows bookings, the revenue lift can disappear before it reaches owner pay.
- Track conversion by consult source.
- Watch booked cases by surgeon.
- Compare quoted price to collected price.
- Segment by graft-count bands.
- Monitor no-shows and reschedules.
Use price ladders for complexity and reputation, not blanket discounts. Mature pricing of $14,500 for senior surgeons, $8,500 for leads, and $11,000 for associates can support margin, but only after variable costs, payroll, and $21,900 in monthly fixed overhead are covered.
2
FUE consultation conversion rate
Consult-to-book rate
Consultation conversion is the share of qualified consultations that turn into booked FUE procedures. It matters because better conversion lifts revenue without the same ad spend increase, so more of each lead dollar turns into surgery cash. Model it from qualified leads, show-rate, consult close rate, and average case value.
Here’s the quick math: booked surgeries = qualified leads × show-rate × consult conversion. If onboarding or pre-op scheduling drags, booked cases slip, cash comes in later, and owner pay gets squeezed even when the pipeline looks full. What this hides is case fit: not every consult should close, and that’s fine.
Track the full funnel
Measure lead cost, consult cost, booked surgery cost, and show-rate by source. That shows whether better conversion is truly lowering acquisition cost per surgery or just moving volume around. With fixed overhead at $21,900/month, each extra booked case helps cover rent, malpractice, and staff before owner distributions.
- Track consult-to-book by source.
- Use before-and-after proof.
- Offer financing early.
- Follow up fast after consults.
- Keep plans clear and patient-led.
Improve conversion with simple surgical planning, strong patient education, and fast response time. Watch the gap between consult date, deposit date, and surgery date. If that lag grows, conversion quality falls and cash flow weakens, even if consult volume stays steady.
3
Surgeon, technician, and clinical labor economics
Clinical Labor Load
This driver is very high-impact because FUE needs skilled extraction, implantation support, physician oversight, and nursing care. The model grows from 1 Senior Hair Surgeon in year one to 2 in mature year, with Lead FUE Specialists rising from 2 to 6 and Registered Nurses from 2 to 6 FTE. Add the $140,000/year Clinic Director and owner income falls fast if booked cases do not keep pace.
The key inputs are booked procedures, surgeon mix, technician FTE, nurse FTE, and whether surgeon pay sits inside payroll. If you are the surgeon-owner, your labor is part of the margin; if you use a contracted or employed surgeon, that cash must be included before estimating distributions. One clean rule: no payout until clinical staffing is covered at the case level.
Track Labor Cost Per Case
Measure labor cost per booked FUE case and tie it to utilization, not headcount alone. Here’s the quick math: more surgeons, specialists, and nurses only help if consults convert and rooms stay full. If staffing rises from 1 to 2 surgeons and 2 to 6 support staff each, but case volume stalls, gross margin gets squeezed and owner take-home pay drops.
Track these weekly: booked cases, show rate, cancellations, FTE by role, and surgeon comp in payroll. Keep one model for owner-surgeon, one for employed surgeon, and one for non-surgeon owner. If surgeon compensation is excluded from payroll, add it back first; otherwise distributions will look stronger than they really are.
- Booked cases by surgeon
- FTE by role
- Compensation by labor class
- Show rate and cancellations
4
Marketing efficiency and patient acquisition cost
Marketing efficiency and patient acquisition cost
Elective hair surgery needs steady paid and organic demand. Patient acquisition cost is the spend needed to get a booked surgery, not just a lead. In year 1, digital marketing and lead acquisition at 80% of revenue leaves only 20% before surgeon pay, labor, rent, and admin. In the mature year, that drops to 60%, which helps margin but still needs tight conversion to protect owner draw.
Here’s the quick math: if reviews slip or follow-up is slow, lead volume can look fine while consults and booked cases lag. Medical financing referral commissions at 30% add another drag on cash, so a strong topline can still squeeze free cash if lead cost, consult cost, and booked-procedure cost are not tracked separately.
Track cost per booked case
Measure lead cost, consultation cost, and booked-procedure cost as separate lines. The owner needs to know how many leads become consults, how many consults become surgeries, and what each booked case costs after ad spend and referral fees. That shows whether growth is buying profit or just busy calendars.
Track leads, consults, booked cases, average case value, the 80% to 60% marketing share, and the 30% financing commission load every month. Speed up follow-up, clean up reviews, and test financing scripts, because better conversion lowers acquisition cost per surgery and leaves more cash for owner pay.
- Watch speed-to-lead daily
- Separate lead and surgery costs
- Track consult show rate weekly
- Audit referral commission impact
5
FUE overhead, equipment, financing, and reserves
Overhead, payroll, and reserves
Fixed overhead of $21,900/month has to be covered before owner pay is safe, which equals $262,800/year before payroll. That includes the $12,000 lease, $4,500 malpractice insurance, $1,800 utilities and waste disposal, $1,200 PRM software and IT, $900 office supplies, and $1,500 licensing fees. If these costs run ahead of case volume, distributions need to wait.
Payroll is the bigger swing factor: it starts at $495,000/year and reaches $101 million/year in the mature case. Add the $250,000 FUE surgical robotic system to capex, then keep reserves for payroll, refunds, downtime, device repair, and reinvestment. Reserves are planning cash, not leftover cash, so underfunding them can make profit look fine while owner withdrawals turn risky.
Track cash before owner draws
Use a simple reserve test: cash on hand should cover the next payroll cycle, fixed overhead, and known repair risk before any owner draw. Track monthly overhead, payroll as a share of revenue, and days cash on hand. If payroll climbs faster than bookings, the clinic can be profitable on paper and still short on cash.
For planning, list every fixed item and update it monthly. The key inputs are rent, insurance, software, licensing, supplies, payroll, and equipment repair. If the robotic system needs downtime or service, hold extra buffer so one broken device does not cut owner income. One clean rule: no reserve, no draw.
- $21,900/month fixed overhead
- $250,000 robotic system capex
- Cover payroll before distributions
- Keep refund and downtime cash
6
Compare low, base, and high FUE clinic owner income scenarios
Owner income scenario table
Owner income shifts with chair utilization, pricing, and marketing spend. Early ramp needs more cash support, while a fuller clinic with more providers lifts profit fast.
| Scenario | Low CaseStartup ramp | Base CaseScaling clinic | High CaseMature clinic |
|---|---|---|---|
| Launch model | The clinic stays in a startup ramp with slower chair fill, first-year pricing, and heavier marketing drag. | The clinic runs on the model case with planned utilization, standard pricing, and the core staffing build. | The clinic scales into a multi-provider setup with stronger utilization, higher pricing, and tighter overhead per case. |
| Typical setup | Revenue is uneven, owner pay stays cautious, and reserves or debt help cover the opening-month cash gap. | Revenue follows the first-year plan, with steady surgeon capacity, fixed overhead, and payroll at the forecast run rate. | Revenue reaches mature volume, more providers share the workload, and fixed costs are spread across more procedures. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $1.1M - $1.5MLow case range | $1.8M - $3.7MBase case range | $9.4M - $11.1MHigh case range |
| Best fit | Use this to stress-test a slower opening and tighter surgeon pay. | Use this for lender talks, hiring plans, and day-to-day owner draw planning. | Use this to test upside, but keep an eye on reserves, debt, and surgeon pay. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Follicular Unit Extraction Hair Clinic Porter's Five Forces Analysis
- Follicular Unit Extraction Hair Clinic BCG Matrix
- Follicular Unit Extraction Hair Clinic Business Model Canvas
- What Are The 5 KPIs For Follicular Unit Extraction Hair Clinic Business?
- Follicular Unit Extraction Hair Clinic Business Plan Template in Pre-Written Word
- How Increase Profits For Follicular Unit Extraction Hair Clinic?
- What Are Operating Costs For Follicular Unit Extraction Hair Clinic?
- FUE Hair Clinic Startup Costs: $835K First-Month Cash Plan
- Follicular Unit Extraction Hair Clinic Financial Model Template in Excel
- How To Open A US FUE Hair Clinic In 6 To 12 Months
- How To Write A Business Plan For Follicular Unit Extraction Hair Clinic?
- Follicular Unit Extraction Hair Clinic Marketing Mix
- Follicular Unit Extraction Hair Clinic Marketing Plan
- Follicular Unit Extraction Hair Clinic Business Proposal
- Follicular Unit Extraction Hair Clinic PESTEL Analysis
- Follicular Unit Extraction Hair Clinic Pitch Deck Example Editable PPTX
- Follicular Unit Extraction Hair Clinic Business SWOT Analysis
- Follicular Unit Extraction Hair Clinic Value Proposition Canvas
Frequently Asked Questions
A FUE clinic owner’s pay depends on salary, distributions, debt, taxes, reserves, and surgeon compensation In the researched first-year case, the Clinic Director salary is $140,000, while EBITDA-style profit is about $161 million before debt, taxes, reserves, and extra clinical owner decisions Revenue is $253,475/month in the first-year assumptions