 Owner income$238K to $3.7M
Owner income$238K to $3.7MHow Much Does a Functional Medicine Practice Owner Make: $238K-$37M

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$238K to $3.7M  Net margin38.2% to 72.5%
Net margin38.2% to 72.5% Revenue for target pay$623K to $5.1M
Revenue for target pay$623K to $5.1M Business difficultyMedium
Business difficultyMedium
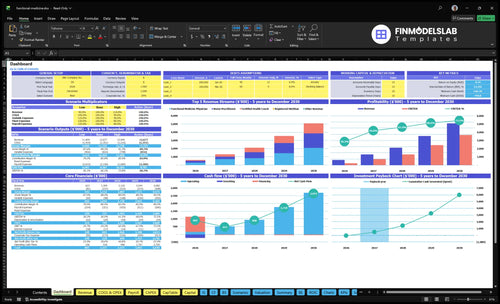


You’re looking at owner take-home, not a generic physician salary In this five-year model, functional medicine practice revenue grows from $623K in Year 1 to $5082M in Year 5, with EBITDA from $238K to $3684M before taxes, debt service, and owner reserve decisions
Owner income$238K to $3.7MNet margin38.2% to 72.5%Revenue for target pay$623K to $5.1MBusiness difficultyMediumWant to calculate owner take-home?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Can you check owner income and the full forecast?
The owner pay view comes first, then the Functional Medicine Practice Financial Model Template tests revenue, margin, costs, reserves, and scenario assumptions. Open the model to see the full plan.
Model highlights
- Owner pay logic
- Revenue and margin
- Scenario and staffing tests
What expenses reduce functional medicine practice owner income?
If you’re asking what cuts owner pay in a Functional Medicine Practice, start with the operating costs: How Much To Launch Functional Medicine Practice? shows the big buckets are direct costs, variable costs, fixed overhead, and payroll. Here’s the quick math: lab test wholesale kits run 8% of revenue in Year 1 and fall to 6% by Year 5, while supplement inventory moves from 5% to 4%.
Direct costs
- Lab kits: 8% to 6%
- Supplements: 5% to 4%
- These hit revenue first
- Less volume, less owner cash
Overhead and payroll
- Marketing and SEO: 6% to 4%
- Medical supplies: 2%
- Fixed overhead: $17,550/month
- Payroll roles total $220K/year
How much revenue does a functional medicine practice need to pay the owner?
A Functional Medicine Practice needs enough collections to cover payroll, overhead, direct costs, taxes, debt service, reserves, and reinvestment before the owner takes cash. In the researched model, $623K in Year 1 collections supports $238K of EBITDA; for launch cost context, see How Much To Launch Functional Medicine Practice?. Here’s the quick math: $238K / $623K = 38.2%, so each $100K of collections creates about $38K of pre-tax income capacity.
Owner Pay Math
- Year 1 collections: $623K
- Year 1 EBITDA: $238K
- EBITDA margin: 38.2%
- Not all EBITDA is distributable
What Changes Pay
- Payroll load and practitioner capacity
- Overhead and direct treatment costs
- Debt service and cash reserves
- Separate pay for owner clinical work
Is a cash-pay functional medicine practice profitable?
Yes—a cash-pay Functional Medicine Practice can be profitable if pricing and utilization stay on target. Using Year 1 rates of $450 per physician treatment, $325 per nurse practitioner treatment, and $150 per health coach treatment, at 65%, 60%, and 50% utilization, the model produces about $623K revenue and $238K EBITDA. Memberships can help smooth cash flow, but no membership revenue is supplied in the source data.
Year 1 math
- $450 physician treatment rate
- $325 nurse practitioner rate
- $150 health coach rate
- $623K revenue at stated utilization
Profit drivers
- $238K EBITDA in Year 1
- Retention keeps visits full
- Compliance supports repeat care
- Capacity and delivery cost decide margin
Want the six income drivers?
1
50%-85%Patient Utilization
More filled schedules lift revenue with little extra cost, so take-home improves as provider use rises from 50% to 85%.
2
$150-$510Visit Price
Higher visit prices raise cash per patient, and the model runs from $150 to $510 per treatment.
3
$623K-$5.1MRecurring Care
Repeat visits and memberships turn retention into the model's $623K to $5.1M revenue path.
4
$220K-$450KPayroll Load
Clinician and support hiring expands capacity, but payroll can climb from about $220K to $450K a year.
5
13% to 10%Lab Margin
Lab kits and supplements fall from 13% of revenue to 10%, so each point saved drops straight to EBITDA.
6
$745KReserve Buffer
Clinic overhead runs $17.6K a month, and the $745K cash floor plus debt service can reduce distributions.
Functional Medicine Practice Core Six Income Drivers
Patient Volume and Provider Utilization
Booked Visits and Provider Utilization
Booked visits are the top-line engine here. In Year 1, the model uses 80 monthly physician treatments at 65% utilization, 100 nurse practitioner treatments at 60%, and 120 health coach treatments at 50%. By Year 5, that grows to 100, 120, and 140 monthly treatments at 85% utilization, so more of the clinic’s hours turn into collected revenue.
Utilization means the share of available clinical time that gets booked and completed. That matters because fixed overhead is already sitting at $17,550 per month. So when fill rate rises, revenue can grow faster than costs, which lifts profit and owner take-home. The main leak is empty capacity from no-shows, slow onboarding, weak referral flow, and too many open clinical hours.
Fill Open Clinical Hours
Track booked visits, completed visits, and no-show rate by provider each month. Also track open hours by role, because a slot that stays empty is lost revenue you never get back. Here’s the quick math: if utilization moves from 50% to 85%, the same staff time produces much more collected revenue without a matching jump in fixed cost.
Manage this with a tight referral pipeline, fast new-patient onboarding, and reminder systems that reduce missed visits. Tie staffing to demand, not hope. If the clinic adds hours faster than bookings rise, margin gets diluted. If booking quality holds while capacity fills, the owner gets more profit from the same overhead base.
1
Average Revenue per Patient
Average Revenue per Patient
If visits are full but cash is still tight, average revenue per active patient is the fastest revenue lever. It moves when physician pricing rises from $450 to $510, nurse practitioner pricing from $325 to $365, and health coach pricing from $150 to $170. Those gains hit every visit, so they can lift collections before you add more staff.
Here’s the quick math: this metric depends on visit mix, care plan attach rate, testing review visits, and follow-up cadence. If the scope is unclear or local demand is price-sensitive, consult-to-care conversion drops, and the higher rate never turns into cash. That cuts gross margin and owner pay.
How to Raise It
Track revenue by provider type, not just total visits. Separate new consults, ongoing care plans, and follow-ups, then compare monthly conversion from consult to ongoing care. If patients see clear value, price rises hold better; if not, the clinic loses bookings.
- Measure revenue per active patient monthly.
- Test price by provider type.
- Watch consult-to-care conversion.
- Track follow-up and plan attach rates.
Use price changes only after the service scope is clear in writing. A $60 lift on physician visits, $40 on nurse practitioner visits, and $20 on coach visits compounds across thousands of annual visits, but only if demand holds and the team can explain the value fast.
2
Recurring Care and Membership Revenue
Recurring Care Revenue
Recurring care includes memberships, structured follow-up visits, and ongoing access after the first consult. In this model, no membership dollars are included, so adding a recurring plan would raise revenue without relying as much on new-patient volume. The main inputs are active members, retention rate, churn, and delivery cost per follow-up.
One clean rule: if the follow-up plan is valuable and compliant, recurring revenue makes owner income steadier. If access is underpriced or cancellations climb, it can add work faster than cash, and that can squeeze take-home pay.
Improve Retention and Follow-Up Cadence
Track renewal rate, monthly churn, and net revenue per active patient. With fixed overhead at $17,550 per month, recurring care can help cover the base cost even when new consult demand dips. Set a clear follow-up cadence, define what each plan includes, and keep the scope tight so renewals do not create hidden labor.
Test pricing against real support time, not just patient interest. Watch cancellation rates, refund requests, and billing rules closely. The goal is simple: stable cash in, controlled delivery cost out.
3
Clinician and Support Payroll
Clinician and Support Payroll
Payroll can build scale or wipe out owner pay. This clinic model grows from 1 to 4 physicians, 1 to 4 nurse practitioners, and 1 to 5 health coaches, plus support staff. Support payroll includes a $85K practice manager, $50K patient coordinators, $45K medical assistants, and $40K receptionists, so every added full-time equivalent (FTE) has to earn its keep.
Owner clinical hours are not the same as business profit. If the owner is still seeing patients, that can hide weak delegation or low utilization. The risk is hiring ahead of demand, which raises cash burn before visits fill. The payoff is simple: when provider time is booked and support is tight, payroll turns into capacity; when it isn’t, it cuts directly into take-home income.
Track FTEs Against Filled Visits
Measure visits per paid provider hour, revenue per clinician FTE, and support staff load before adding headcount. Payroll should rise only when booked visits and delegated tasks justify it. One clean rule: if a new hire does not increase filled capacity, it probably lowers owner cash.
- Separate owner clinic time from profit.
- Test staffing before hiring full-time.
- Watch utilization, no-shows, delegation.
Use the mix deliberately: more physicians and nurse practitioners lift capacity, while health coaches and support staff protect delivery. But if low utilization leaves open hours on the calendar, the added $85K, $50K, $45K, and $40K roles can erase margin fast.
4
Lab and Supplement Margin
Lab and Supplement Margin
Lab kits and supplements add revenue, but they are not pure profit. In Year 1, lab wholesale kits cost 8% of revenue and supplement inventory costs 5%, so gross margin after these direct costs is about 87%. By Year 5, those costs fall to 6% and 4%, lifting gross margin to 90%.
The owner only keeps what is left after refunds, waste, compliance work, and any pass-through pricing. So $100 of ancillary sales is not $100 of owner income. The key question is whether the product mix is truly needed and turns fast enough to protect cash.
Track SKU Margin, Not Just Sales
Measure each item by revenue, direct cost, refund rate, and expired inventory. If a supplement or kit has weak patient need, it can turn a high-margin sale into dead stock fast. Reorder from actual use, not gut feel.
- Price by item margin
- Limit pass-through discounts
- Document patient need
- Count inventory monthly
What this estimate hides: compliance issues and waste can quietly eat the 87% to 90% gross margin range. Tight controls add contribution, but gross sales should still be treated as business revenue, not owner pay.
5
Fixed Overhead, Marketing, and Reserves
Fixed Overhead and Reserves
Fixed Overhead and Reserves set the ceiling on safe owner pay. Monthly fixed overhead is $17,550, driven by $12,000 rent, $2,500 liability insurance, and $1,200 software, so that cost lands before the owner sees profit. Marketing adds 6% of Year 1 revenue, then falls to 4% by Year 5.
Here’s the quick math: if collections dip, those costs still hit cash. With $235K of upfront capex and a $745K minimum cash need in Month 2, reserves protect payroll and slow months, and they keep owner distributions from draining the clinic too early.
Protect Cash, Then Pay Yourself
Use a monthly cash test: revenue minus $17,550 fixed overhead, minus marketing at 6% in Year 1. Set owner draws only after that math still leaves cash above the $745K Month 2 floor. That keeps pay tied to real collections, not booked visits.
- Track overhead as revenue moves.
- Track marketing from 6% to 4%.
- Hold cash above $745K.
- Pause draws in weak months.
6
Compare lean, base, and high-growth owner-income scenarios
Owner income scenarios
Owner income rises with provider count, utilization, pricing, and cost control. Early years carry more fixed overhead per visit, while later years spread rent and staff across more volume.
| Scenario | Low CaseLaunch | Base CaseScaling | High CaseMature |
|---|---|---|---|
| Launch model | This is the lean launch case with lower owner income in the first operating year. | This is the modeled mid-case with stronger owner income after demand is proven. | This is the stronger earnings path with the highest modeled owner income. |
| Typical setup | Year 1 shows $623K revenue, $238K EBITDA, 38.2% margin, 1 physician, 1 nurse practitioner, 1 health coach, and 50% to 65% utilization. | Year 3 shows $2.12M revenue, $1.303M EBITDA, 61.5% margin, 2 physicians, 2 nurse practitioners, 3 health coaches, and 75% to 80% utilization. | Year 5 shows $5.082M revenue, $3.684M EBITDA, 72.5% margin, 4 physicians, 4 nurse practitioners, 5 health coaches, and 85% utilization. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $238KLaunch case | $1.3MProven demand | $3.7MScale case |
| Best fit | Use this to stress-test opening month demand and how fast visits fill. | Use this as the core planning case for a clinic with repeat patient flow and a stable team. | Use this to test what multi-provider scale could produce once the practice is mature. |
Planning note: These figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions; reserves, debt service, taxes, and owner salary policy can lower take-home cash.
Related Products
- Functional Medicine Practice Porter's Five Forces Analysis
- Functional Medicine Practice BCG Matrix
- Functional Medicine Practice Business Model Canvas
- How Increase Functional Medicine Practice Profitability?
- Functional Medicine Practice Business Plan Template in Pre-Written Word
- How Increase Profitability Functional Medicine Practice?
- What Are The Operating Costs Of A Functional Medicine Practice?
- Functional Medicine Practice Startup Costs: $745K Funding Plan
- Functional Medicine Practice Financial Model Template in Excel
- How To Open A Functional Medicine Practice In 3–6 Months
- How To Write Functional Medicine Practice Business Plan?
- Functional Medicine Practice Marketing Mix
- Functional Medicine Practice Marketing Plan
- Functional Medicine Practice Business Proposal
- Functional Medicine Practice PESTEL Analysis
- Functional Medicine Practice Pitch Deck Example Editable PPTX
- Functional Medicine Practice Business SWOT Analysis
- Functional Medicine Practice Value Proposition Canvas
Frequently Asked Questions
The researched model shows pre-tax owner income capacity of $238K in Year 1 and $3684M by Year 5, using EBITDA before taxes, debt service, reserves, and distribution policy Revenue grows from $623K to $5082M Treat this as planning math, not a guaranteed owner salary