 Owner income$1.58M
Owner income$1.58MHow Much Does a Hair Restoration Clinic Owner Make? $0–$27M Range

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$1.58M  Net margin70%
Net margin70% Revenue for target pay$2.27M
Revenue for target pay$2.27M Business difficultyHard
Business difficultyHard


Key Takeaways
- More completed cases spread fixed overhead and lift margin.
- Price and add-ons drive revenue before labor costs.
- Conversion quality matters when consult flow misses targets.
- Heavy overhead makes reserve planning non-negotiable.
Owner income$1.58MNet margin70%Revenue for target pay$2.27MBusiness difficultyHardWant to test your owner income target?
Owner income calculator
Estimate owner take-home and the target-pay gap from monthly revenue, gross margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only, not guaranteed salary, tax advice, or owner distribution advice. Actual take-home depends on revenue, margin, payroll, reserves, and financing.
Want to check owner income in the Hair Restoration Clinic forecast?
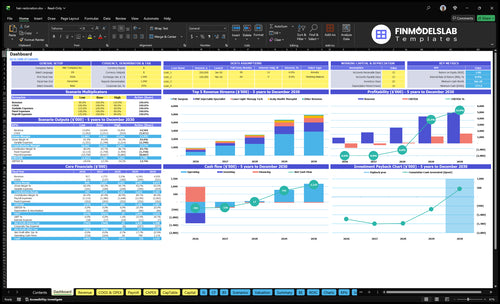
This Hair Restoration Clinic Financial Model Template shows dashboard metrics, revenue, margin, costs, reserves, and owner take-home; open the model.
Owner-income model highlights
- Owner take-home and salary
- Revenue $765k to $4.1M
- Test volume, price, staffing
What costs most affect hair restoration clinic margins?
The biggest margin drag is clinical labor, not supplies. Listed wages run $770k in Year 1, $970k in Year 2, and $144M by Year 5, while fixed overhead sits at $293k a month, led by the $20k clinical facility lease; for setup context, see How Much Does It Cost To Open And Launch Your Hair Restoration Clinic?
COGS stay lower at 80% in Year 1 and 65% in Year 5, so payroll, utilization, and booked procedures matter more than supplies. Marketing and commissions also hit hard at 110% of revenue in Year 1 and 85% in Year 5, so every weak pipeline leaves surgeon time and rooms underused.
Labor and overhead
- $770k wages in Year 1
- $970k wages in Year 2
- $293k monthly fixed overhead
- $20k clinical facility lease
Demand and fees
- 80% COGS in Year 1
- 65% COGS in Year 5
- 110% of revenue in Year 1
- 85% of revenue in Year 5
What revenue is needed to pay a hair restoration clinic owner?
To pay the owner $300k in Year 2, a Hair Restoration Clinic needs about $198M in annual revenue, or $165k per month, before reserves and financing. Using the listed payroll and fixed overhead, break-even revenue is about $161M per year, and revenue does not automatically become owner pay. Year 2 contribution margin after COGS, marketing, and commissions is about 81.9%.
Owner pay math
- $198M supports $300k owner pay
- $161M is break-even revenue
- $165k monthly before reserves
- Revenue is not take-home pay
Key margin drivers
- Year 2 margin is about 81.9%
- COGS cuts owner capacity fast
- Marketing and commissions reduce cash
- Debt service lowers pay too
How much profit can a hair restoration clinic make?
A Hair Restoration Clinic can lose about $379k in Year 1, then turn positive at about $131k operating profit in Year 2 and reach about $2.4M by Year 5 if utilization grows as modeled; track demand early with What Is The Current Growth Rate Of Patient Consultations At Your Hair Restoration Clinic?. The issue isn’t price alone: payroll starts before treatment slots fill.
Profit path
- Year 1 revenue: about $917k
- Year 1 operating profit: about -$379k
- Year 2 revenue: about $1.77M
- Year 2 operating profit: about $131k
Owner cash
- Listed wages: about $770k
- Fixed overhead: about $351.6k
- Year 5 profit: about $2.4M
- Surgeon-owner salary: modeled at $300k
What drives owner income most?
1
$384K-$2.4MProcedure Volume
More FUE cases move owner take-home the most because this is the highest-ticket line and it scales fastest.
2
$8K-$9.5KAverage Case Price
Each price step lifts revenue without adding the same labor load, so margin improves fast.
3
EditableConsult Conversion
No source conversion rate is provided, so booked consults stay a direct lever on owner income.
4
60%-95%Labor Efficiency
Higher utilization across clinical staff spreads payroll over more treatments and protects EBITDA.
5
8%-6%Marketing Cost
Lower ad spend per booked patient keeps more cash in the clinic while demand is still building.
6
$29.3K/moOverhead Discipline
Tight fixed costs matter because the clinic carries rent, insurance, software, and admin costs from month one.
Hair Restoration Clinic Core Six Income Drivers
Procedure Volume
Procedure Volume
Procedure volume is the count of completed hair transplant cases, mainly FUE. It drives income because the clinic’s $293k monthly fixed overhead gets spread across more revenue as case count rises. Here’s the quick math: at 48 cases per month, overhead is about $6,104 per case; at 255, it falls to about $1,149 per case. That only helps if consult flow, physician time, technicians, rooms, and patient experience keep the schedule full.
Measure Fill, Not Just Demand
Track completed cases, booked consults, and fill rate by surgeon and room. If utilization climbs without enough consults or staff coverage, cancellations and wait times will eat margin and hurt owner pay. The useful target is not just more bookings; it’s more completed procedures with stable quality. Measure no-shows, case time, and technician hours per case so the team can forecast capacity before adding demand.
1
Average Case Price
Average Case Price
Average case price is the revenue per patient before labor and overhead. In this model, FUE rises from $8,000 in Year 1 to $9,500 in Year 5, a 18.75% increase. PRP moves from $750 to $850, laser from $200 to $250, and scalp health from $150 to $180. Mix matters, because more add-ons can lift cash per visit without adding consult volume.
Owner pay moves with this number because each extra dollar lands before fixed overhead. Here’s the quick math: if case count stays flat, a higher weighted average price raises gross profit and helps cover the $293k monthly overhead base. The main risks are discounting, weak financing approval, and lower graft-count assumptions, all of which can pull realized price down fast.
Price by case mix, not by guesswork
Track average realized price per completed patient, not just list price. Break it out by FUE, PRP, laser, and scalp health, plus financing approval rate, graft count, and add-on attach rate. That tells you whether the clinic is earning the price it quotes or leaking revenue through discounts and weak closes.
Test pricing by service line and keep a simple rule: if a higher price lowers close rate more than it raises revenue per booked case, owner income falls. Also watch cash timing; slower approvals can delay collections even when booked revenue looks fine.
- Weighted average price drives revenue per patient.
- FUE is the main price anchor.
- Add-ons lift ticket without extra consults.
- Track realized price after discounts.
- Test pricing by graft count and financing.
2
Consult Conversion
Consult Conversion Rate
Hair restoration clinics make money when inquiries turn into booked consults and then booked procedures. The model gives treatment volume, but not a conversion rate, so owners need to track all three steps. Weak follow-up, low trust, or slow financing approval can leave FUE capacity idle, which cuts revenue and keeps fixed overhead from being spread across enough cases.
Here’s the quick math: if a clinic gets many leads but few completed procedures, cost per completed patient rises even when cost per lead looks fine. That hurts gross margin and cash flow, because the owner pays staff and overhead before the procedure revenue shows up. Better inquiry quality can lift take-home pay without adding another provider.
Track Consult-to-Procedure Flow
Measure inquiries → booked consults → booked procedures every week, not just lead volume. The key control is the close rate at each step, plus financing approval speed and no-show rate. If consults are booking but procedures are not, the leak is usually trust, pricing fit, or payment friction.
Use a simple dashboard with cost per completed patient, not just marketing cost per lead. Then test better pre-screening, faster follow-up, and clearer financing steps so more qualified patients move through the same clinical capacity. That raises revenue quality and protects owner draw without raising headcount.
3
Clinical Labor Efficiency
Clinical Labor Efficiency
Clinical labor efficiency is the margin lever that decides how much of each paid case stays after payroll. In this model, wages rise from $770k in Year 1 to $144M in Year 5, so small waste in physician time, technician hours, or canceled cases can cut owner take-home fast. More booked procedures only help if staff time matches the schedule.
What it includes: surgeon time, technician labor, PRP and laser staffing, scalp therapy coverage, overtime, and contractor premiums. The key inputs are booked cases, case length, cancellation rate, and labor hours per procedure. If long cases or training gaps push hours up, gross margin falls even when revenue looks strong.
Track labor hours per case
Measure labor cost per completed procedure, physician hours per case, tech hours per case, and cancellation rate by service line. Match schedules to booked cases, not to a fixed calendar. If demand shifts between FUE, PRP, laser, and scalp care, cross-train staff so one slow line does not force overtime or contractor use.
- Booked cases by service line
- Hours per completed case
- Cancellation and no-show rate
- Overtime and contractor mix
- Training time before full productivity
Here’s the quick math: if payroll rises but case volume and room flow do not keep pace, owner draw shrinks because gross margin gets squeezed first. The fastest fix is tighter scheduling and faster staff ramp-up, not cutting clinical quality.
4
Marketing Cost Per Patient
Marketing Cost Per Patient
For a hair restoration clinic, this is the cost to acquire one booked and one completed patient, not just a lead. In the model, marketing starts at 80% of revenue and falls to 60% by Year 5; at Year 2 revenue of $177M, marketing is about $133k before sales commissions. If acquisition cost rises faster than case price or close rate, owner cash flow gets squeezed fast.
Here’s the quick math: track inquiries, booked consults, booked procedures, and completed procedures. A higher cost per completed case hits gross margin before fixed overhead and owner pay. Expensive leads hurt less when average case price and consult co nversion are strong, but weak follow-up can leave surgery slots empty.
Track Cost Per Completed Case
Measure cost per booked procedure and cost per completed procedure by channel: search, referrals, reviews, social proof, and local competition. One clean rule: if spend grows but booked cases do not, cut or fix that channel before adding more budget. Strong reviews and referral flow usually lower acquisition cost more than broad lead buying.
Build a weekly funnel report with spend, inquiries, consults booked, procedures booked, and procedures completed. That shows where cash is leaking. If finance approval, trust, or follow-up is weak, paid traffic turns into expensive noise, and the owner feels it first in lower profit and a smaller draw.
- Track cost per completed case.
- Compare channels every week.
- Watch close rate by source.
- Protect margin before scaling spend.
5
Fixed Overhead And Reserves
Heavy Fixed Overhead
Before the first procedure is sold, this clinic already carries $293k per month in fixed overhead. The named costs total $65.3k for lease, insurance, utilities, cleaning, software, security, and office supplies, so the rest sits in other fixed items not listed here. If monthly operating profit does not clear that base, there is no room for owner pay.
What matters is the gap between procedure revenue and fixed cost coverage. To estimate real take-home income, track monthly cases, average case price, variable clinical labor, debt service, and a reserve target. Operating profit is not the same as cash you can spend; owner draws, personal taxes, and reinvestment reserves come after that.
Protect Cash First
Set a monthly cash floor before paying yourself. With $293k in fixed overhead, the owner should watch cash on hand, case volume, and how fast consulting demand turns into booked procedures. If procedure flow slows, overhead keeps running and take-home pay drops fast.
Track fixed cost coverage, reserve funding, and debt payments separately. Build the forecast with procedure count, average case price, and monthly fixed spend, then hold back cash for equipment financing and buildout loans that are not in the listed overhead. Never mix operating profit with owner distributions.
6
Compare lean, base, and high-performing owner income scenarios
Owner income table
Owner income changes fast here because treatment volume, staffing, and fixed clinic overhead all move together. The low, base, and high cases show how much take-home can change as capacity fills.
| Scenario | Low CaseDownside case | Base CaseCore case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the slower ramp case, where early revenue stays light and owner income is squeezed by fixed clinic overhead. | This is the modeled case, where the clinic reaches steadier volume and owner income turns positive. | This is the stronger earnings case, where the clinic uses more capacity and owner income rises sharply. |
| Typical setup | Year 1 uses about $765k monthly revenue, one FUE surgeon, one PRP specialist, one laser tech, one scalp therapist, one care coordinator, and $293k monthly fixed overhead. | Year 2 assumes about $1.478M monthly revenue, 9 FUE, 45 PRP, 85 laser, 65 scalp, and 22 care-coordinator treatments, with two FUE surgeons and stable support staffing. | Year 5 assumes about $4.112M monthly revenue, 10 FUE, 60 PRP, 100 laser, 80 scalp, and 30 care-coordinator treatments, with expanded staffing across all service lines. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | ($379k)Loss case | $131kPositive profit | $24MUpside case |
| Best fit | Use this to stress-test the launch if patient flow is weak or ramp-up takes longer than planned. | Use this as the planning baseline for a clinic that fills its schedule but is still building scale. | Use this to test upside if referrals, conversions, and room utilization all run ahead of plan. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. Owner take-home can be split between salary and distributions, and reserves stay editable because no source pay rates were provided.
Related Products
- Hair Restoration Clinic Porter's Five Forces Analysis
- Hair Restoration Clinic BCG Matrix
- Hair Restoration Clinic Business Model Canvas
- Tracking 7 Essential KPIs for Hair Restoration Clinic Success
- Hair Restoration Clinic Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Hair Restoration Clinic Profitability Now
- Managing Monthly Running Costs for a Hair Restoration Clinic
- Hair Restoration Clinic Startup Costs: $605K+ CAPEX Plan
- Hair Restoration Clinic Financial Model Template in Excel
- How To Open A Hair Restoration Clinic In 4 To 9 Months
- How to Write a Hair Restoration Clinic Business Plan in 7 Steps
- Hair Restoration Clinic Marketing Mix
- Hair Restoration Clinic Marketing Plan
- Hair Restoration Clinic Business Proposal
- Hair Restoration Clinic PESTEL Analysis
- Hair Restoration Clinic Pitch Deck Example Editable PPTX
- Hair Restoration Clinic Business SWOT Analysis
- Hair Restoration Clinic Value Proposition Canvas
Frequently Asked Questions
In this model, a non-physician investor owner may take no distribution in Year 1 because operating profit is about -$379k By Year 2, operating profit is about $131k before taxes, reserves, and debt A physician-owner who also fills the Medical Director Lead Surgeon role may include the modeled $300k salary, bringing Year 2 pre-tax owner income near $431k