 Owner income$80.5k/mo
Owner income$80.5k/moHow Much Does A Healthcare Clinic Owner Make? $805K/Month Model

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$80.5k/mo  Net margin57.8%
Net margin57.8% Revenue for target pay$139.3k/mo
Revenue for target pay$139.3k/mo Business difficultyMedium
Business difficultyMedium


You’re trying to separate clinic owner income from employee physician pay, and that matters In this researched first-year model, the clinic shows $139,295 in monthly revenue and $80,524 in monthly operating cash flow before clinician compensation, debt, taxes, reserves, and owner distributions This is a planning estimate for a US outpatient clinic, not tax advice, medical advice, or a guaranteed salary
Owner income$80.5k/moNet margin57.8%Revenue for target pay$139.3k/moBusiness difficultyMediumWant to test your own clinic owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the clinic financial model?
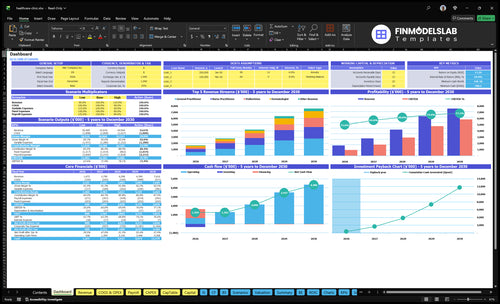
The dashboard in the Healthcare Clinic Financial Model Template shows revenue, visits, costs, cash flow, and owner take-home—open it.
Owner-income model highlights
- Owner take-home output
- Revenue and margin
- Low, base, high cases
What is a good profit margin for a healthcare clinic?
A good profit margin for a Healthcare Clinic is scenario-based, not a fixed benchmark: the first-year operating margin can look like 578% before clinician compensation, debt, taxes, and reserves, but the real margin drops once provider pay is in. For setup cost context, see How Much Does It Cost To Open And Launch Your Healthcare Clinic Business? so you can pair margin with startup cash needs. Payroll, not revenue, usually decides how much profit stays in the clinic.
Margin drivers
- Payer mix changes cash collected.
- Collection rate moves margin fast.
- Denials cut realized revenue.
- Specialty mix affects service margin.
Cost pressure points
- 6% medical supplies.
- 3% pharmaceuticals.
- 4% EHR and billing software fees.
- 3% outsourced diagnostics, plus $10,000 rent and $2,500 malpractice insurance.
How much revenue does a healthcare clinic need to pay the owner?
A Healthcare Clinic does not pay the owner from top-line revenue alone; owner pay is a planning output, and at about $83.19 contribution per paid visit after 16% variable and supply costs, the clinic needs about 439 paid visits a month to cover $36,483 in fixed overhead plus support payroll before provider compensation. If the goal is $20,000 a month for the owner, add that to provider payroll, debt service, and reserves, so the required visit count rises above break-even. That’s the quick math.
Base break-even
- $36,483 fixed overhead + support payroll
- 16% variable and supply costs
- 439 paid visits monthly
- $83.19 contribution per visit
Owner pay plan
- $20,000 monthly owner pay target
- Add provider payroll first
- Add debt service next
- Keep reserves in the model
Does a healthcare clinic owner make more if they work as a provider?
Yes, often—if the owner is licensed and fills billable provider time, they can earn clinical pay plus profit distributions. In a Healthcare Clinic model, monthly revenue grows from $139,295 with 7 providers in Year 1 to $532,541 with 14 providers by Year 4, but that’s before unlisted clinician payroll, and proper scope rules are non-negotiable.
Owner-as-provider
- Earns clinical pay plus distributions.
- Must be licensed to bill.
- Only works if capacity is filled.
- Clinical scope cannot be stretched.
Owner-manager
- Relies on profit after payroll.
- Scale adds payroll and compliance load.
- Scheduling and billing get harder.
- More providers can lift total profit.
Want the six biggest clinic income drivers?
1
1.4K/moPatient Volume
More visits spread the $36.5K fixed base and lift take-home because revenue runs about $99 a visit.
2
$80-$170Service Mix
A richer mix of higher-priced visits pushes weighted revenue up, since visit prices range from $80 to $170.
3
180-450Provider Productivity
Higher visits per clinician raise revenue without adding rent or admin costs at the same pace.
4
$36.5K/moLabor Control
Keeping support payroll near plan protects the $80.5K pre-clinician cash flow from wage creep.
5
84%Collections
If the clinic keeps 84% after supplies, software, and outsourced tests, more billed revenue reaches owner cash.
6
$15.9K/moOverhead Discipline
Lease, utilities, insurance, IT, and office costs set the break-even floor, so reserve discipline matters.
Healthcare Clinic Core Six Income Drivers
Patient Volume And Capacity
Patient Volume Ceiling
Visit count sets the revenue ceiling. Year 1 capacity is modeled at 50% to 65% across services, so empty slots matter fast. The clinic only gets paid when visits are completed and collected, so no-shows, room limits, and provider hours can cut realized revenue even if demand looks strong.
Here’s the quick math: 480 monthly modeled visits from general practitioners produce $48,000 in revenue, or about $100 per visit. More filled slots lift owner income only if staffing, rooms, and billing can absorb the extra volume without pushing up overtime or denials.
Fill The Right Slots
Measure booked visits, completed visits, no-show rate, and collection rate by provider and service. If utilization rises but cash does not, the bottleneck is usually staffing, room capacity, or billing lag, not demand.
- Track booked versus completed visits.
- Watch no-shows by service.
- Match schedules to provider hours.
- Review collections within 30 days.
Use the schedule to protect margin. If volume rises before labor and collections keep pace, the owner sees more revenue on paper but not much more cash to pay themselves.
1
Payer Mix And Collections
Payer Mix and Collections
Collected revenue is what pays the owner, not billed charges. With $80 to $150 Year 1 visit prices, the real driver is the payer mix—commercial insurance, Medicare, Medicaid, and self-pay—plus denial rate and collection rate. A $150 dermatology visit only helps take-home income when it is paid, so slow claims can make a strong month feel cash-poor.
Tighten Claims Follow-Up
Track paid claims by payer, days to collect, and denial reasons every week. Here’s the quick math: collected revenue = billed visits × collection rate, then payer adjustments decide what lands in cash for payroll, reserves, and distributions. Faster billing follow-up matters because even small delays can choke owner pay when visit volume stays steady.
2
Provider Productivity And Staffing Model
Provider Mix And Payroll Drag
Provider productivity is the mix of doctors, therapists, and nurse practitioners that creates billable visits. In Year 1, the clinic runs with 2 general practitioners, 1 pediatrician, 1 dermatologist, 1 physiotherapist, and 2 nurse practitioners. More provider hours can raise revenue, but each added provider also adds payroll before the owner gets paid.
By Year 4, the mix grows to 5 general practitioners, 2 pediatricians, 2 dermatologists, 2 physiotherapists, and 4 nurse practitioners. That only helps income if schedules stay full and the clinic can support licensing, supervision, and care quality. Empty hours are lost revenue, but overstaffing is profit drag.
Track Capacity Per Licensed Provider
Measure visits per provider, utilization rate, and payroll per collected visit. Here’s the quick math: if a provider adds more visits, revenue rises only when those slots are filled and collected. If schedule gaps, no-shows, or supervision rules block slots, owner take-home falls even when headcount looks strong.
Forecast by provider type, not one blended number. A dermatology visit at $150 does not help if access, payer rules, or staffing limits cut volume. Build schedules around real working hours, then check whether the extra payroll still leaves enough gross profit to cover overhead and the owner draw.
3
Service Mix And Ancillary Revenue
Service Mix
Service mix is the share of primary care, pediatric, dermatology, physiotherapy, diagnostics, labs, vaccines, wellness, and follow-up visits. In Year 1, treatment prices run from $80 for nurse practitioner visits to $150 for dermatology visits, so mix drives average revenue per encounter. More high-value visits lift collected revenue fast.
The catch is margin. Higher-value services often need more supplies, equipment, and compliance work, so owner pay only improves when added gross profit beats those costs. More revenue per visit does not help if licensing, payer rules, or clinical scope block the service or add too much overhead.
Track Margin By Visit Type
Measure revenue per encounter by service line, not just total visits. Here’s the quick math: blend the $80 to $150 price range by visit mix, then subtract direct supplies, lab fees, and staff time. With fixed overhead at $16,900/month, small mix shifts can decide whether there is cash left for the owner draw.
Before adding ancillaries, test the service-level margin and billing path. Track five inputs:
- Visits by service type
- Collected price per service
- Supply and lab cost per visit
- Payer rules and denials
- Staff minutes per encounter
4
Labor Cost Control
Labor Cost Control
Payroll gets paid before owner distributions, so this driver sets how much cash is left to pay yourself. In Year 1, support payroll is about $19,583/month for the clinic manager, medical assistants, receptionist, billing specialist, and janitorial staff. If visit volume is soft but staffing stays fixed, labor eats margin fast and owner draws shrink.
By Year 4, support payroll rises to about $37,917/month, so staffing has to move with visit volume. Overtime, front desk coverage, billing backlog, benefits, and contracted labor can squeeze cash flow even when revenue looks fine on paper. One clean rule: if labor grows faster than collected revenue, owner pay gets squeezed.
Match Staff to Visits
Track labor as a share of collected revenue, not just headcount. Watch overtime hours, billable visits per staff hour, denial backlog, and contractor use for coverage. If those numbers rise while visit volume is flat, payroll is running ahead of demand and take-home income will fall.
Use staffing plans tied to visit volume, then test schedule changes before adding permanent labor. The goal is simple: keep front desk, billing, and clinical support tight enough to protect cash, but not so lean that care quality drops. Better scheduling and clean billing protect owner income because payroll stays aligned with collections.
- Compare payroll to collected revenue monthly.
- Flag overtime before it becomes routine.
- Clear billing backlogs fast.
- Use contractors only for spikes.
5
Overhead, Reserves, And Reinvestment
Overhead, Reserves, and Reinvestment
When the clinic carries $16,900/month in fixed overhead, owner pay is whatever is left after rent, utilities, malpractice insurance, maintenance, licensing, IT support, and office supplies. That means a strong month can still produce thin distributions if collections are uneven or variable overhead from software and diagnostics creeps up.
- $10,000 lease
- $1,500 utilities
- $2,500 malpractice insurance
- $800 maintenance
- $500 licensing
- $1,200 IT support
- $400 office supplies
Here’s the quick math: fixed costs do not flex with patient volume, so every slow pay cycle or empty schedule slot hits cash twice. Distributable income falls, but reserves matter because they keep payroll, compliance, and equipment spending funded during payer delays. The owner’s draw stays safer when cash planning is treated as part of profit.
Track cash, not just profit
Build the monthly model from collected revenue, $16,900 fixed overhead, EHR and billing software fees, outsourced diagnostics, payer delay days, and a reserve target. If cash on hand cannot cover the next payroll cycle and overhead, distributions are too high. That is the real control point.
- Track days cash on hand.
- Separate reserves from operating cash.
- Review software and diagnostic fees monthly.
- Set a draw rule after reserves.
What this estimate hides is timing. A clinic can show profit and still feel tight if insurers pay late or a compliance bill lands at the wrong time. Keep reinvestment tied to items that protect capacity or collections, so each dollar spent supports future owner income instead of draining it.
6
Compare low, base, and high clinic owner income scenarios
Owner income scenarios
Owner income here shifts with visit volume, pricing, and support payroll. The clinic scales fast, but clinician pay and fixed overhead can change take-home cash a lot.
| Scenario | Lean CaseLean case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | Lower owner-income path with Year 1 ramp and partial capacity use. | Modeled mid-case with Year 3 scale and stronger throughput. | Stronger upside path with Year 4 scale and higher visit density. |
| Typical setup | Year 1 volume is 14,065 visits a month, with $139,295 in monthly revenue, 16% variable and supply costs, and $36,483 fixed plus support payroll. | Year 3 volume is 32,358 visits a month, with $350,685 in monthly revenue, about 14.2% variable and supply costs, and about $49,400 fixed plus support payroll. | Year 4 volume reaches 46,455 visits a month, with $532,541 in monthly revenue, about 13.2% variable and supply costs, and about $54,817 fixed plus support payroll. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $80,524/moLean income | $251,488/moBase income | $407,428/moHigh income |
| Best fit | Use this for early ramp-up planning and to test cash flow before the clinic is fully staffed. | Use this as the main planning case for steady operations and scaled outpatient demand. | Use this to test upside if the clinic fills capacity faster and keeps support costs in line. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. They exclude unlisted clinician compensation, debt, taxes, reserves, and guaranteed distributions.
Related Products
- Healthcare Clinic Porter's Five Forces Analysis
- Healthcare Clinic BCG Matrix
- Healthcare Clinic Business Model Canvas
- 7 Critical KPIs to Scale Your Healthcare Clinic
- Healthcare Clinic Business Plan Template in Pre-Written Word
- How to Increase Healthcare Clinic Profitability: 7 Actionable Strategies
- How to Run a Healthcare Clinic: Analyzing Core Monthly Operating Costs
- Healthcare Clinic Startup Costs: $365k CAPEX And $788k Cash Need
- Healthcare Clinic Financial Model Template in Excel
- How To Open A Healthcare Clinic: 3-9 Month Launch Roadmap
- How to Write a Healthcare Clinic Business Plan in 7 Steps
- Healthcare Clinic Marketing Mix
- Healthcare Clinic Marketing Plan
- Healthcare Clinic Business Proposal
- Healthcare Clinic PESTEL Analysis
- Healthcare Clinic Pitch Deck Example Editable PPTX
- Healthcare Clinic Business SWOT Analysis
- Healthcare Clinic Value Proposition Canvas
Frequently Asked Questions
In the researched first-year model, the clinic produces $139,295 in monthly revenue and $80,524 in operating cash flow before clinician compensation, debt, taxes, reserves, and owner distributions That equals about $966,287 annualized before those items Actual owner take-home depends on provider payroll, payer collections, debt service, reinvestment, and whether the owner works clinically