 Time to Open6 monthsLaunch runway
Time to Open6 monthsLaunch runwayHow to Open a Home Infusion Therapy Service in 4–9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6 monthsLaunch runway  Launch Sequence3 stagesCompliance first
Launch Sequence3 stagesCompliance first Key BottleneckLicense gateState rules
Key BottleneckLicense gateState rules First Revenue StepScheduled episodeReferral to booking
First Revenue StepScheduled episodeReferral to booking


To start a home infusion therapy business, choose your service scope, confirm state requirements, secure clinical leadership, set pharmacy and supply relationships, recruit qualified infusion nurses, and activate payer and referral channels before accepting patients A realistic researched planning assumption is a 4 to 9 month launch window because licensing, accreditation, payer setup, and nurse hiring vary by state and service model In the model, Year 1 pricing ranges from $350 to $750 per treatment, with 40 to 60 monthly treatments per clinician and 45% to 70% utilization depending on specialty First revenue comes when a hospital, physician, discharge planner, specialty clinic, or case manager referral converts into a scheduled and documented home infusion episode
Time to Open6 monthsLaunch runwayLaunch Sequence3 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepScheduled episodeReferral to bookingLaunch timeline
This is a short web summary of the home infusion launch timeline, and the XLSX export holds the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10
Licensing / compliance
- State rule review
- Scope approval
- Policy pack draft
- License filing
- Audit prep
Payer contracting
- Payer target list
- Credential packets
- Contract review
- Benefit rules
- Denial workflow
Pharmacy / supplies
- Pharmacy shortlist
- Supply quotes
- Cold chain setup
- Kit standards
- Reorder triggers
Staffing / training
- Role profiles
- Candidate outreach
- Skills checks
- Onboarding steps
- Coverage roster
Systems / billing
- Intake design
- EHR setup
- Care protocols
- Billing rules
- Emergency tree
Referral / launch
- Referral list
- Outreach launch
- Scheduling drill
- First patient
- Launch review
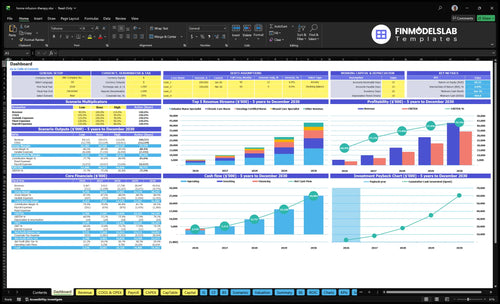
Why model the first-patient ramp before launch?
Screenshot shows revenue, costs, cash needs, assumptions, and break-even logic—open the Home Infusion Therapy Service Financial Model Template now.
Key launch inputs
- 29 staff, five roles
- $350-$750 pricing
- 40-60 treatments
- 45%-70% utilization
- $45k-$56k revenue
- 21% variable costs
- Payer lag hits cash
What licenses are needed to start a home infusion therapy service?
A Home Infusion Therapy Service usually needs state health care provider clearance, nursing supervision authority, pharmacy or pharmacy-partner permissions, and payer credentialing before it takes referrals; check What Are The Operating Costs Of Home Infusion Therapy Service? while building the license budget. This is not legal advice: review all 50 state rules first, then define service scope, pharmacy model, clinical leadership, accreditation path, payer enrollment, and operating policies.
Core permissions
- Verify state healthcare provider rules
- Confirm nursing supervision requirements
- Set pharmacy license or partner model
- Check infusion-specific or home health permissions
Readiness checks
- Prepare 100% written clinical protocols
- Keep nurse competency files current
- Build emergency escalation and documentation standards
- Start Medicare workstream; CMS benefit began January 1, 2021
How do you get referrals for a home infusion therapy service?
Get referrals by making the Home Infusion Therapy Service easy to trust and easy to use: hospitals, discharge planners, infectious disease, oncology, gastroenterology, specialty clinics, specialty pharmacies, case managers, and payer networks want clear fit, fast intake, and clean paperwork. If you're mapping the launch, How To Write A Business Plan To Launch Home Infusion Therapy Service? shows how to package that readiness. The first dollar comes only after benefit verification, authorization if needed, pharmacy coordination, nurse scheduling, the home visit, and billable documentation.
What sources want
- Exact therapies accepted
- Service area and nurse coverage
- Intake steps and payer workflow
- Escalation and document turnaround
What converts interest
- Fast benefit checks
- Authorization before scheduling
- Pharmacy and nurse coordination
- Capacity for $350 to $750 visits
How long does it take to open a home infusion therapy service?
Home Infusion Therapy Service usually takes 4 to 9 months to open. The timeline depends on state licensing, any needed accreditation, payer enrollment, referral readiness, pharmacy coordination, and how fast you hire qualified infusion nurses. A fast launch keeps the service narrow; if onboarding, contracting, or pharmacy workflows slip, first revenue slips too.
Fast launch path
- Use partner pharmacy arrangements.
- Start with limited therapies.
- Keep payer setup tight.
- Hire to referral volume, not guesses.
Year 1 staffing mix
- 12 infusion nurse specialists.
- 4 oncology certified nurses.
- 2 pediatric infusion nurses.
- 8 chronic care nurses and 3 wound care specialists.
Confirm whether the home infusion service is ready to open safely
Launch readiness checklist
Use this go-live approval checklist to confirm the home infusion service is ready before opening.
Compliance
- Entity setup filedCritical
The service needs a legal entity before contracts, payers, and vendors move forward.
- State license reviewCritical
Home infusion rules vary by state, so license gaps can block launch.
- Accreditation path setHigh
If accreditation is required, the path must be clear before patient start.
- Service scope approvedHigh
Infusion, oncology, pediatric, chronic care, and wound care must match approved scope.
Clinical
- Clinical policies approvedCritical
Care steps need written rules before nurses treat patients at home.
- Emergency escalation readyCritical
Clear escalation helps staff respond fast to adverse reactions or line issues.
- Patient safety procedures testedHigh
Safety checks reduce home-care errors during the first treatments.
- Supervision coverage assignedHigh
Nurses need a named clinical lead for oversight and case review.
Pharmacy
- Pharmacy relationship signedCritical
Drug access is core to service delivery, so pharmacy terms must be locked.
- Sterile compounding process setHigh
Sterile prep coordination protects medication quality and patient safety.
- IV kits and pumps stockedCritical
Treatment starts fail fast if kits, pumps, or disposables are short.
- Cold chain storage verifiedCritical
Temperature control protects medication integrity before and after delivery.
Staffing
- Nurse hiring completeCritical
You need enough qualified nurses before booking first patients.
- Infusion competency signedCritical
Competency proof keeps infusion tasks within trained hands.
- Specialty coverage matchedHigh
Oncology, pediatric, chronic care, and wound care need the right mix.
- On-call roster setHigh
After-hours coverage prevents service gaps and late patient escalations.
Revenue
- Intake workflow liveCritical
Referrals stall without a clear intake path from order to first visit.
- Benefit checks workingCritical
Benefit checks help confirm coverage before costly home care starts.
- Prior auth workflow readyHigh
Prior authorization delays can block treatment and cash collection.
- Claims submission testedHigh
Claims need to pass before launch so revenue does not sit unbilled.
- Referral sources activatedMedium
Hospitals, physicians, and specialty clinics drive the first patient flow.
Finance
- Pricing within rangeHigh
Year 1 prices should stay within the $350-$750 model range.
- Variable cost load checkedHigh
Year 1 variable costs should stay near 21% of revenue.
- Cash runway fundedCritical
Minimum cash is $905k in Month 1, so funding must be ready before opening.
- Go-live signoff completeCritical
Do not open until compliance, staffing, pharmacy, and payer flow all say ready.
Which launch drivers decide if the service can open safely?
1Licensing Path
4-9 moNo volume fixes a missing license, so this gate controls go-live timing.
2Pharmacy Supply
21% loadA tested medication-to-home flow cuts missed deliveries, temperature issues, and canceled starts.
3Clinical Staffing
40-60/moMatched nurse skill to therapy type keeps specialty referrals safe and controlled.
4Payer Billing
$350-$750Credentialing and prior auth must work first, or cash collection slows fast.
5Referral Activation
45-70%Named referral contacts help convert openings into scheduled care faster.
6Intake Ops
Dry runA dry run from intake to claim protects safety and keeps visits on track.
Licensing and Accreditation Pathway
Licensing and Accreditation First
Compliance is the gate, not volume. In home infusion therapy, you cannot serve patients on day one unless the legal and clinical permission path is in place. State rules can change based on service scope, pharmacy involvement, nursing model, and payer strategy, so the launch plan has to confirm entity structure, healthcare licensing, supervision rules, pharmacy duties, accreditation, and any Medicare or payer supplier requirements before you book demand.
One clean rule: no referrals before the paperwork path is documented. If you push hospitals, physicians, or case managers too early, you risk a delay where demand exists but you still cannot treat, bill, or show credibility. The readiness signal is a written, approved pathway plus clinical and billing policies that match the exact operating model.
Map the Permission Path
Start with a state-by-state checklist for the exact service model you plan to run. Confirm who owns the entity, who supervises nurses, whether a pharmacy partner is required, and what accreditation or payer enrollment must happen before first treatment. That sequence keeps launch timing real and avoids expensive rework.
Build the file before the pipeline. Keep copies of licenses, policies, supervision rules, pharmacy agreements, accreditation steps, and payer forms in one launch folder. Then test whether a referral can move from intake to scheduled care without hitting a missing approval. If that dry run fails, opening on time will slip.
- Confirm service scope first
- Match rules to each state
- Lock pharmacy obligations early
- Finish payer steps before outreach
- Document policies before first case
1
Pharmacy and Supply Chain Readiness
Pharmacy and Supply Chain Readiness
Home infusion can launch through a partnership model or an integrated model, so the key is clear pharmacy accountability, not ownership for its own sake. Before first treatment, you need a tested medication-to-home path: sourcing, sterile compounding coordination where needed, IV kits, pumps, supplies, cold-chain control, delivery timing, storage, and inventory steps.
This driver also shapes cash and timing. Year 1 assumptions put medical consumables and IV kits at 85% of revenue, with specialty pharmacy procurement fees at 45%. If any handoff breaks, the first visit slips or gets canceled. Missed delivery, temperature failure, or missing supplies can stop day-one care even when nursing is ready.
Test the home-delivery chain before opening
Run one dry case from order to bedside before the first paid visit. Verify who orders meds, who owns storage, who tracks cold chain, and who signs off on delivery timing. That one-page handoff should show the exact pharmacy partner, backup contact, kit contents, and escalation steps.
- Confirm pharmacy accountability in writing.
- Track cold chain at every transfer.
- Match kits to each therapy type.
- Set delivery windows before scheduling.
- Keep backup supplies on hand.
Do not open with a vague vendor plan. A missed shipment or unclear ownership can turn a scheduled treatment into a lost visit. The readiness signal is simple: a tested medication-to-home workflow that works before the first patient is booked.
2
Clinical Staffing and Nurse Competency
Clinical Staffing and Nurse Competency
Safe launch capacity depends on matched nurse skill, not just referral demand. For day one, the staffing plan needs infusion-trained registered nurses, validated vascular access skills, competency checklists, clinical protocols, and supervision rules in place. The Year 1 model calls for 12 infusion nurse specialists, 4 oncology certified nurses, 2 pediatric infusion nurses, 8 chronic care nurses, and 3 wound care specialists.
Monthly capacity also has to fit the therapy mix: the model assumes 40 oncology treatments to 60 infusion nurse specialist treatments per clinician. If the team accepts specialty referrals without trained coverage, the launch slows, visits get delayed, and safety misses rise. One clean rule: no matched nurse, no booked visit.
Map skill to therapy before opening
Before launch, assign each nurse to a therapy lane, then test the route, supervision, on-call coverage, and patient education scripts. The readiness check should show who can handle oncology, pediatrics, chronic care, and wound care, plus who backs up each shift. That keeps the opening volume controlled instead of forcing risky last-minute coverage.
- Match nurse credentials to therapy type.
- Document vascular access competency.
- Train escalation and patient scripts.
- Build on-call coverage before first visit.
- Limit referrals to covered services.
If specialty demand comes in faster than staffing readiness, hold volume back. That protects day-one care quality and avoids launching with gaps that create callbacks, reschedules, and avoidable clinical risk.
3
Payer Credentialing and Billing Workflow
Payer Setup Before First Claim
Payer enrollment, credentialing, contracts, and prior authorization rules can delay opening even when nurses and equipment are ready. For home infusion, you cannot count on clean first revenue until the referral can move through benefit verification, coding, documentation, claims submission, and collections without a gap.
The cash impact is real: Year 1 billing and claims processing fees are modeled at 3% of revenue, while service prices range from $350 for wound care to $750 for oncology. If you treat before authorization or charting is complete, you create avoidable denials and slow cash collection on day one.
Test the Referral-to-Claim Path
Before opening, run one complete case from referral to claim. Confirm the payer list, required documents, coding rules, authorization steps, and who owns denial follow-up and collections. The readiness signal is simple: a tested workflow that works before care starts, not after the first patient is booked.
Set a hard go-live rule: no visit until benefit verification, prior authorization, and documentation standards are complete. Keep a checklist for enrollment status, contract terms, claim forms, and posting rules. That protects opening timing and avoids the cash squeeze that comes from rework, delayed billing, and missed reimbursement.
- Verify payer enrollment status first.
- Test prior auth before scheduling.
- Assign denial tracking on day one.
- Document coding rules by therapy type.
4
Referral Source Activation
Referral Source Activation
Referral sources need to be live before opening, not built after the license arrives. For home infusion, the real launch gate is whether hospitals, discharge planners, physicians, case managers, specialty pharmacy partners, and payer networks already know who to call and how to send a complete referral. If that’s missing, the business can be licensed and still sit idle.
This driver also shapes day-one care. A referral only turns into revenue after it becomes scheduled care, pharmacy coordination, a completed visit, and billable documentation. The risk is broad outreach without enough nurse coverage, intake speed, or payer setup. That creates wasted marketing, slow starts, and frustrated referral partners.
Build the referral path first
Lock down the launch rules before outreach: accepted therapies, service radius, payer list, nurse coverage, intake turnaround, the documentation packet, and the escalation process. Then test the handoff with named contacts at target hospitals, oncology and gastroenterology practices, infectious disease groups, specialty clinics, and payer teams.
Use a simple readiness check: can a referral source send the right packet, and can your team convert it into a scheduled visit without back-and-forth? If the answer is no, opening date risk goes up. The launch win is fewer dead-end referrals and faster early ramp.
5
Intake, Scheduling, Documentation, and Safety Operations
Referral-to-Claim Control
This driver decides whether referrals turn into safe first visits or sit in a queue. Home infusion needs referral intake, benefit checks, prior authorization handoff, care plan documentation, nurse dispatch, delivery timing, route scheduling, escalation, and recordkeeping to work in one chain. If any step is weak, the launch slows fast and canceled starts rise.
The capacity check is simple: Year 1 utilization is 45% to 70%, and each clinician is expected to handle 40 to 60 monthly treatments. So the workflow has to match nurse capacity, not just referral demand. One clean rule: don’t accept more referrals than intake, pharmacy, and scheduling can move the same day.
Dry Run the First Case
Before opening, run a sample case from referral to claim and time each handoff. Use one real-looking patient file, one treatment order, one nurse route, and one documentation packet so you can see where the delay shows up. That test should prove the team can coordinate eligibility, scheduling, delivery, visit notes, and claim-ready records without guesswork.
- Check referral data at intake.
- Verify payer and benefit details.
- Hand off prior authorization fast.
- Confirm nurse, delivery, and route.
- Test escalation for adverse events.
- Review documentation before claim.
If the dry run breaks at any point, fix that step before launch. Weak intake or slow scheduling can trigger avoidable cancellations, which hurts first-day revenue and patient trust at the same time.
6
Related Products
- Home Infusion Therapy Service Porter's Five Forces Analysis
- Home Infusion Therapy Service BCG Matrix
- Home Infusion Therapy Service Business Model Canvas
- What Five KPI Metrics Should Home Infusion Therapy Service Business Track?
- Home Infusion Therapy Business Plan Template in Pre-Written Word
- How Increase Profits Home Infusion Therapy Service?
- What Are The Operating Costs Of Home Infusion Therapy Service?
- Home Infusion Therapy Startup Costs: $905K Opening Cash Plan
- Home Infusion Therapy Financial Model Template in Excel
- How Much Home Infusion Therapy Owners Make at $55M Revenue
- How To Write A Business Plan To Launch Home Infusion Therapy Service?
- Home Infusion Therapy Service Marketing Mix
- Home Infusion Therapy Service Marketing Plan
- Home Infusion Therapy Service Business Proposal
- Home Infusion Therapy Service PESTEL Analysis
- Home Infusion Therapy Pitch Deck Example Editable PPTX
- Home Infusion Therapy Service Business SWOT Analysis
- Home Infusion Therapy Service Value Proposition Canvas
Frequently Asked Questions
Start with service scope, state requirements, clinical leadership, pharmacy coordination, payer setup, and referral workflow The researched launch window is 4 to 9 months In the model, Year 1 treatments are priced from $350 to $750, with 40 to 60 monthly treatments per clinician once staffing and utilization are in place