 Owner income$3.8M–$34.1M
Owner income$3.8M–$34.1MHow Much Home Infusion Therapy Owners Make at $55M Revenue

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$3.8M–$34.1M  Net margin69%–79%
Net margin69%–79% Revenue for target pay$5.5M–$43.0M
Revenue for target pay$5.5M–$43.0M Business difficultyMedium
Business difficultyMedium


Key Takeaways
- Higher census matters only after fixed costs are covered.
- Billing speed and denials drive cash, not just revenue.
- Drug and supply control protects margin across therapies.
- Routing and scheduling turn visits into real profit.
Owner income$3.8M–$34.1MNet margin69%–79%Revenue for target pay$5.5M–$43.0MBusiness difficultyMediumWant to test your owner take-home?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate only, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income depends on revenue, margins, payroll, taxes, debt, and reinvestment.
Want to check owner income in the Home Infusion Therapy Service model?
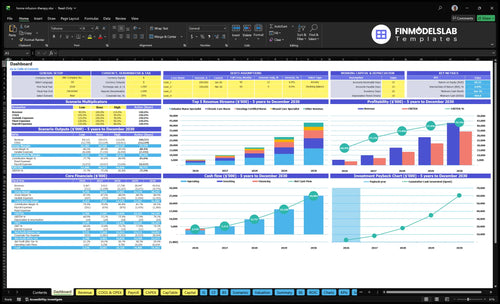
Open the Home Infusion Therapy Service Financial Model Template dashboard first; it shows revenue, margin, overhead, payroll, cash need, and owner pay.
Owner-income model highlights
- Owner pay scenarios
- Therapy-line revenue outputs
- Cash need and reserves
What costs reduce home infusion therapy profit?
Home Infusion Therapy Service gets squeezed hardest by medication procurement, IV kits, travel, billing, denials, waste, and nurse time; for the planning side, see How To Write A Business Plan To Launch Home Infusion Therapy Service?. In Year 1, listed direct costs add up to 210% of revenue, with 85% consumables and IV kits, 45% specialty pharmacy procurement fees, 50% nurse travel and mileage, and 30% billing and claims fees. By Year 5, they still total 175%, so profit only improves if safety, procurement discipline, documentation, and scheduling all hold up.
Main cost drains
- 85% consumables and IV kits
- 45% specialty pharmacy procurement fees
- 50% nurse travel and mileage
- 30% billing and claims fees
What protects margin
- Keep safety steps tight
- Buy only what each case needs
- Document every dose and visit cleanly
- Pack routes to cut idle drive time
How many home infusion patients are needed to pay the owner?
Home Infusion Therapy Service needs about 160 monthly infusion treatments to cover Year 1 fixed overhead before owner pay; use episodes, not one patient count, because one active patient may need multiple visits. For the cost base behind that math, see What Are The Operating Costs Of Home Infusion Therapy Service?: the model shows 995 monthly treatments, $4.556 million in monthly revenue, and about $579k in fixed overhead plus listed payroll.
Break-Even Math
- Use monthly treatments, not patients
- Revenue per treatment: about $4,579
- Contribution after listed direct costs: 79.0%
- Break-even: $579k ÷ $3,617 = 160
Owner Pay Impact
- Add 28 treatments per $10k owner pay
- $10k/month owner pay needs about 188 treatments
- Therapy mix can move the answer
- More visits per patient lower patient count needed
How much revenue does a home infusion therapy service make per patient?
A Home Infusion Therapy Service does not earn one fixed amount per patient; it earns per treatment or episode, so the real number depends on the therapy mix and payer rules. In the model, Year 1 prices range from $350 for wound care specialist services to $750 for oncology certified nurse services, with weighted revenue around $458 per monthly treatment and about $539 by Year 5.
What moves revenue
- Medication type changes the price.
- Episode length changes total revenue.
- Nursing visits add billable value.
- Supplies can raise the ticket.
What to check first
- Check payer contracts before pricing.
- Verify authorization rules first.
- Watch collection rate and denials.
- Confirm local payer rules by market.
Want the six drivers that move owner income most?
1
$456K/moReferral Flow
More referrals and active patients push Year 1 revenue to about $456K a month, so census is the fastest path to owner cash.
2
$350-$850Therapy Mix
Higher-acuity therapies pay more, with prices from $350 to $850, so mix shifts can lift income without many more visits.
3
3.0%-2.2%Collections
Billing friction cuts take-home; claims fees start at 3.0% and only drop to 2.2%, so cleaner payer work matters.
4
13.0%-11.1%Supply Margin
Consumables and pharmacy fees begin at 13.0% of sales and improve to 11.1%, so buying and waste control protect gross profit.
5
45%-85%Nurse Utilization
Nurse schedules and drive time decide how much capacity turns into paid work, while travel reimbursement still runs 5.0% to 4.2% of sales.
6
$58K/moOverhead Scale
About $58K a month of fixed costs, plus $905K minimum cash in Month 1, means scale has to arrive early for owner pay to grow.
Home Infusion Therapy Service Core Six Income Drivers
Active patient census
Active patient census
Active patient census is the count of patients getting monthly infusion treatments. It matters because more treatments spread fixed overhead across more visits, so owner pay improves only after volume clears the 160 monthly treatments break-even point before owner pay in Year 1. The model scales from about 995 monthly treatments in Year 1 to 6,658 by Year 5.
Here’s the quick math: if census rises but case complexity, collections, or staffing lag, margin gets thinner, not better. Referral gaps, long intake cycles, uneven nurse routing, and delayed authorizations are the main risks. More volume helps only when those parts move together.
Track census quality
Measure active patients, monthly treatments, referral-to-start time, authorization lag, denial rate, and nurse visits per route. Those inputs show whether volume is turning into cash, not just chart count. If starts slow down, the census number can look strong while owner income stalls.
Push density in the same zip codes, review routing weekly, and keep a floor above 160 monthly treatments before drawing owner pay. A simple rule: more patients only helps when collections and staffing rise with them.
1
Therapy and medication mix
Therapy Mix
Therapy mix changes both revenue and cash. Year 1 modeled prices range from $350 for wound care to $750 for oncology certified nurse visits, with $450 infusion nurse specialist, $600 pediatric infusion nurse, and $400 chronic care nurse cases in between. Two clinics with the same visit count can still have very different owner pay.
No therapy is automatically profitable. Owner income depends on collected reimbursement minus drug cost, supplies, nurse time, travel, documentation, and waste. A higher-priced case can still hurt cash if procurement cost is high or denial risk delays payment. The real metric is net cash per completed visit, not charge per visit.
Track Net Cash by Case Type
Measure each therapy by cases, charge, collected reimbursement, drug and supply cost, nurse time, travel miles, and denials. Use one report to compare whether a $750 oncology case really out-earns a $350 wound care visit after all direct costs.
- Track net cash per therapy.
- Separate drug cost from labor.
- Watch denials and waste fast.
- Route long trips to protect margin.
If a therapy type needs expensive procurement, long travel, or frequent rework, change pricing, staffing, or case mix before it drains owner pay.
2
Payer mix and collections
Payer Mix and Collections
For home infusion, owner income is tied to cash collected, not just claims sent. If services are authorized, billed cleanly, and matched to viable payer contracts, the model assumes billing and claims processing fees of 30% of revenue in Year 1, improving to 22% by Year 5. That spread matters because every point kept in collections flows through to profit and the owner’s draw.
Here’s the catch: denials can shrink cash even when accounting revenue looks fine. Track authorization rate, days to collect, denial rate, write-offs, and net collection rate. One clean claim can pay better than three messy ones. If claims lag or denials stack up, payroll, drug buys, and owner pay all feel the squeeze fast.
Track Cash, Not Just Charges
Measure each step of the revenue cycle so you can fix the leak, not guess at it. Start with authorization before treatment, then watch claim lag, denial causes, and write-off patterns by payer. The goal is simple: fewer rework loops and faster cash in the bank.
- Track authorization rate weekly
- Watch days to collect monthly
- Split denials by reason code
- Review net collection rate by payer
- Compare billed charges to cash received
If collections slip, owner income falls twice: first in delayed cash, then in higher billing cost. Faster collection improves working capital, which helps fund supplies, nurses, and the owner’s take-home pay without adding more volume.
3
Drug and supply margin
Drug and Supply Margin
If drug and supply buying gets sloppy, margin disappears fast even when visit volume holds. In this model, Year 1 direct costs run 85% for medical consumables and IV kits plus 45% for specialty pharmacy procurement fees; by Year 5, those fall to 74% and 37%. The owner’s take-home rises only when more of each billed treatment stays after direct supply cost.
This driver includes drug acquisition, IV kits, consumables, waste, and unreimbursed items. The key inputs are treatment count, purchase price, reimbursement, denial rate, unusable inventory, and procurement terms. One bad batch or loose stock control can turn a high-revenue case into weak cash flow, because gross margin funds nurse pay, overhead, and owner draw.
Control Buy Cost and Waste
Track unit cost per treatment, waste rate, and unreimbursed supply rate every month. Tie each case to the ordered drug, kit, and pump use, so you can spot shrink fast. Barcoding, inventory checks, pump tracking, and vendor contract review protect margin; shortcuts usually just create more write-offs.
Use the same test on every therapy line: collected revenue minus direct supply cost. If a therapy needs high-cost kits or has frequent unusable items, renegotiate terms or tighten usage rules. Here’s the quick math: if direct supply cost falls, more of each treatment can cover fixed overhead and leave profit for the owner.
4
Nursing labor utilization
Nursing Labor Utilization
This driver is about how many billable visits each nurse can complete after you account for travel time, after-hours coverage, and schedule gaps. In Year 1, the model uses 29 revenue-producing clinicians across five service lines, with capacity rates of 450% to 700% by line. If routing is weak, paid labor turns into mileage, overtime, and lost owner draw.
By Year 5, clinicians rise to 130 and capacity reaches 800% to 850% by line, so margin depends on keeping each visit productive. Here’s the quick math: more completed visits per paid hour lifts gross margin; more unplanned drive time does the opposite. What this hides is clinical safety, licensure, and service quality, which still have to hold.
Track Visits per Paid Hour
Measure billable visits per clinician day, travel minutes per visit, ove rtime hours, and after-hours fill rate. If one nurse can cover more visits without raising overtime or burnout, owner income improves because labor cost stays closer to collected revenue. If routing pushes nurses into long drives or late calls, cash flow tightens fast.
Use daily dispatch rules, zip-code clustering, and shift caps to protect margin. Track: scheduled visits, completed visits, overtime, and miles per visit. Keep licensure and care quality first, but cut dead time hard. One clean rule: fewer empty miles means more money left after payroll.
5
Fixed overhead scale
Fixed overhead scale
Fixed overhead includes rent, liability insurance, software, marketing, compliance audits, telecom, dispatch, and payroll that do not move much with each visit. In Year 1, that base is $181k per month, plus $477k of payroll in Year 1. At $4.556M monthly revenue, overhead is about 4.0% of sales; by Year 5 at $359M, it falls to about 0.05%.
That drop matters because owner pay comes after fixed bills are covered. The risk is simple: if volume, collections, or staffing slip, these costs still hit the bank account. Keep cash reserves for compliance, cash timing, and growth, or the business can look profitable on paper but still strain owner draws.
Watch the overhead ratio
Track fixed overhead as a percent of revenue every month, plus rent, insurance, software, marketing, audits, and dispatch payroll by line item. Here’s the quick math: fixed cost dollars stay mostly flat, so the owner keeps more profit as monthly revenue rises. If revenue stalls, the same $181k base eats a bigger share of income fast.
Test whether each fixed spend earns its keep. Marketing should support referral flow, software should cut admin time, and compliance should stay current without overspend. Build a reserve before expanding headcount or space, because the payback on overhead only works when volume and collections stay ahead of the fixed bill.
6
Scenario objective for home infusion therapy income scenarios
Owner income table
Owner income shifts with treatment volume, case mix, and nurse capacity. Fixed overhead stays meaningful, so the same service can swing a lot by Year 1, Year 3, and Year 5.
| Scenario | Low CaseEarly scale | Base CaseScaled operations | High CaseHigh-volume network |
|---|---|---|---|
| Launch model | This is the early-scale case built from Year 1 assumptions. | This is the modeled middle case built from Year 3 assumptions. | This is the upside case built from Year 5 assumptions. |
| Typical setup | About 995 monthly treatments, $4.56M monthly revenue, 79.0% gross margin, and about $579k monthly overhead define the launch case. | About 2,962 monthly treatments, $1.48M monthly revenue, 80.8% gross margin, and about $77.6k monthly overhead define the core case. | About 6,659 monthly treatments, $3.59M monthly revenue, 82.5% gross margin, and about $105k monthly overhead define the scale case. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $3.8M/yrLaunch case | $13.5M/yrCore case | $34.1M/yrUpside case |
| Best fit | Use this to test launch-month staffing and referral flow. | Use this as the steady-state plan after the first growth push. | Use this to test a larger network with strong utilization. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Home Infusion Therapy Service Porter's Five Forces Analysis
- Home Infusion Therapy Service BCG Matrix
- Home Infusion Therapy Service Business Model Canvas
- What Five KPI Metrics Should Home Infusion Therapy Service Business Track?
- Home Infusion Therapy Business Plan Template in Pre-Written Word
- How Increase Profits Home Infusion Therapy Service?
- What Are The Operating Costs Of Home Infusion Therapy Service?
- Home Infusion Therapy Startup Costs: $905K Opening Cash Plan
- Home Infusion Therapy Financial Model Template in Excel
- How to Open a Home Infusion Therapy Service in 4–9 Months
- How To Write A Business Plan To Launch Home Infusion Therapy Service?
- Home Infusion Therapy Service Marketing Mix
- Home Infusion Therapy Service Marketing Plan
- Home Infusion Therapy Service Business Proposal
- Home Infusion Therapy Service PESTEL Analysis
- Home Infusion Therapy Pitch Deck Example Editable PPTX
- Home Infusion Therapy Service Business SWOT Analysis
- Home Infusion Therapy Service Value Proposition Canvas
Frequently Asked Questions
The model shows about $362M in Year 1 operating profit before owner taxes, reserves, debt service, and reinvestment That comes from $547M in revenue, 210% listed direct costs, and $6942k in annual fixed overhead plus payroll Actual take-home depends on distributions, cash reserves, payer collections, and owner role