 Owner income≈$1.0M–$10.9M
Owner income≈$1.0M–$10.9MHow Much Can a Hospice Care Owner Make at $199M Year 1 Revenue

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income≈$1.0M–$10.9M  Net margin0.5%–0.8%
Net margin0.5%–0.8% Revenue for target pay≈$199M
Revenue for target pay≈$199M Business difficultyMedium
Business difficultyMedium
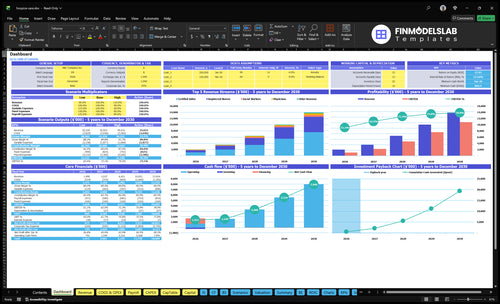


You’re trying to see whether hospice ownership can support real take-home pay after care costs, payroll, compliance, and cash reserves In the provided five-year model, revenue grows from $199 million in Year 1 to $1392 million in Year 5, before any owner distributions This excludes tax advice, guaranteed pay, nonprofit compensation, and reimbursement eligibility guidance
Owner income≈$1.0M–$10.9MNet margin0.5%–0.8%Revenue for target pay≈$199MBusiness difficultyMediumWant to test your hospice owner take-home?
Owner income calculator
This calculator estimates owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Need a cleaner hospice income model?
This Hospice Care Financial Model Template shows revenue, margin, costs, reserves, and owner take-home assumptions—open it.
Owner-income model highlights
- Owner-pay line test
- Revenue, margin, cash flow
- 3 RNs to 15
- 5 aides to 25
- 70% supplies, $150k salary
How do hospice businesses make money?
Hospice Care makes money from reimbursed care days and service mix, not a single universal rate. Routine home care, continuous care, inpatient care, and respite care all add billable activity, and payer mix plus Medicare hospice reimbursement shape how much cash is actually collected. In the model, monthly revenue is about $1,658k in Year 1 and $116M in Year 5, but denied claims, delayed claims, caps, documentation gaps, and geographic rules can cut that cash.
How cash comes in
- Routine home care drives daily billing.
- Continuous care covers crisis hours.
- Inpatient care adds higher-acuity revenue.
- Respite care fills short-term stays.
What hits collections
- $1,658k monthly in Year 1.
- $116M monthly in Year 5.
- Medicare and payer mix affect cash.
- Claims issues can slow or cut payment.
How many patients does a hospice need to be profitable?
Hospice Care can’t be tied to an exact profitable patient count from the supplied data because average daily census and patient days are missing. For What Is The Most Important Indicator Of Success For Hospice Care?, the practical floor is revenue: with $43,125 in monthly fixed/admin costs and 17% variable costs, break-even before unprovided clinical payroll is about $52,000/month ($43,125 ÷ 83%).
What’s missing
- Average daily census count
- Total monthly patient days
- Clinical payroll by role
- Revenue per patient day
What drives profit
- Grow recurring census revenue
- Keep staff utilization high
- Protect referral stability
- Match growth with care quality
What is the profit margin for a hospice business?
There isn’t one clean profit margin for Hospice Care. The model says direct nonlabor costs are 170% of revenue in Year 1 and 150% in Year 5, with fixed overhead at $165k a year, and the supplied operating margin before reserves, taxes, debt, and unprovided clinical payroll is about 570% in Year 1 and 805% in Year 5; for the startup cost side, see What Is The Estimated Cost To Open And Launch Your Hospice Care Business?.
Gross margin
- Direct nonlabor costs hit 170% in Year 1.
- Direct nonlabor costs fall to 150% in Year 5.
- Fixed overhead stays at $165k per year.
- Admin payroll rises from $3,525k to $4,575k.
Operating margin
- Model shows 570% in Year 1.
- Model shows 805% in Year 5.
- Excludes reserves, taxes, and debt.
- Real margin swings with clinical and billing costs.
What drives hospice owner income most?
1
$199M-$1.39BAverage Daily Census
More patient-day volume is the biggest income lever, and the model scales from $199M in Year 1 to $1.392B in Year 5.
2
HighNet Reimbursement
Better payer mix and cleaner collections lift cash per patient day, so the same census pays more.
3
60%-90%Clinical Staffing Efficiency
Tighter caseloads and visit planning spread labor over more billable care, but overtime can eat the gain.
4
$1.38M/moBilling Quality
Fewer denials and faster claims keep cash moving against about $1.375M of fixed overhead each month.
5
10%-11%Pharmacy and DME
Tighter drug and equipment buys protect margin because direct supply costs start near 11% of revenue and ease toward 10%.
6
$884KReserve Policy
Keeping more cash on hand can cut owner draw now, but it lowers payroll and care risk when collections lag.
Hospice Care Core Six Income Drivers
Average Daily Census
Average Daily Census
Hospice average daily census is the number of patients active each day, and it drives patient-day revenue. Higher ADC spreads leadership, billing, rent, insurance, and electronic health record costs across more care days, which usually lifts margin and owner take-home. The source data does not provide ADC, so treat it as an input, not a fixed fact.
Here’s the pressure point: growth only helps if admissions stay compliant and staff can cover it. The model’s capacity rises from 700% in Year 1 to 880% in Year 5 for registered nurses, and from 750% to 900% for certified aides. If ADC outruns staffing or referral quality, cash flow can look strong on paper but break in operations.
Track ADC Against Care Capacity
Measure ADC next to RN caseloads, aide coverage, referral reliability, and compliance limits. The clean test is simple: if census rises but staffing ratios, documentation, or visit timing slip, you lose margin and risk billing delay. One good census number is not enough; it has to be staffed, documented, and paid correctly.
Use ADC in the forecast as a monthly driver, then tie it to patient-day revenue and fixed-cost absorption. Watch admissions quality, denials, and response time each week. If census growth is ahead of nurse and aide capacity, slow intake or add coverage before service quality drops and owner draw gets squeezed.
1
Net Revenue Per Patient Day
Net Revenue Per Patient Day
Net revenue per patient day is the cash you keep per covered day of care after payer mix, care-level mix, geographic wage index, billing accuracy, caps, denials, and collection timing. Source data does not provide a per-day reimbursement rate, so treat it as an editable assumption and a current-source validation item, not a fixed promise.
If patient days stay constant, a 1% swing in net yield moves revenue by about $1.99M in Year 1 and $13.92M in Year 5, based on supplied revenue of $199M and $1,392M. That flows straight into owner income because payroll, billing, and compliance costs do not fall at the same pace.
Track Net Yield by Payer and Day
Build the model from patient days, then test net rate by payer, service level, and market. Use routine versus more complex days, then compare billed amounts to cash collected. One clean number matters: net revenue per patient day.
- Track net rate by payer mix.
- Split routine and complex days.
- Watch denial and appeal rates.
- Test wage index by service area.
- Measure days from claim to cash.
Use the average against $199M in Year 1 and $1,392M in Year 5, then compare it with operating profit of $113M and $1,121M. Even a small drop in net rate can trim the owner draw, because fixed admin and compliance costs still get paid.
2
Clinical Staffing Efficiency
Clinical Staffing Efficiency
Hospice staffing is a direct profit lever because pay for registered nurses, certified aides, social workers, spiritual counselors, physicians, benefits, overtime, and on-call shifts comes out before owner pay. In the supplied model, staffing rises from 3 registered nurses and 5 certified aides in Year 1 to 15 registered nurses and 25 certified aides in Year 5, so labor discipline matters more as census grows.
Here’s the quick math: if caseloads drift low or overtime fills gaps, labor eats margin fast; if scheduling stays compliant and coverage is tight, more of each patient day drops to profit. The risk is not understaffing care. The risk is paying for unused capacity, especially on-call time and benefits, while reimbursement lands later.
Track Caseloads, Not Just Headcount
Track patients per RN, aide visits per shift, overtime hours, and on-call call-outs every week. Use those numbers to set hiring timing, because a new hire should lift capacity before the schedule breaks. The goal is compliant coverage at the lowest workable labor cost, not the smallest team.
- RN caseloads by daily census
- Aide utilization by visit volume
- Overtime and on-call hours
- Benefits as a payroll percent
- Coverage for social and spiritual care
Also watch physician oversight and other covered hours that do not fall cleanly with visits. If those costs rise faster than patient days, gross margin drops and the owner has less cash for reserves, hiring, and profit draw.
3
Pharmacy And Durable Medical Equipment Costs
Pharmacy and DME Cost Control
Pharmacy, oxygen, durable medical equipment (DME), medical supplies, and mileage sit close to the line between profit and owner pay. In this model, Medical Supplies & Drugs fall from 70% of revenue in Year 1 to 65% in Year 5, DME falls from 40% to 35%, and transportation falls from 40% to 35%. That means a 5-point swing can move cash fast, so vendor pricing and authorization rules directly affect take-home.
The quick math is simple: if revenue holds at $1,000,000, a 5-point cost drop saves $50,000. What this hides is leakage from rushed orders, missing documentation, and noncompliant substitutions. In hospice, the fix is not cheaper care; it is tighter care-plan discipline, clean approvals, and vendor terms that match the actual mix of meds, oxygen, and equipment used.
Track orders, mileage, and approvals
Measure spend by bucket: drugs, DME, oxygen, medical supplies, and transportation. Tie each order to an approved care plan, then compare actual use to patient-day volume and admission mix. If same-day delivery or rush orders rise, margin usually falls before you see it in payroll. That is the one-liner: buy only what the care plan justifies.
- Track cost as % of revenue.
- Review vendor discounts and terms.
- Log mileage by patient and zone.
- Approve substitutions before dispensing.
Test whether tighter authorization cuts waste without delaying care. Document who can order, when refill rules apply, and which items need pre-approval. If vendor terms slip or mileage spikes, owner pay gets squeezed even when census is stable. Keep the forecast editable, because these costs move with patient acuity and supplier contracts, not just with revenue.
4
Compliance, Billing, And Administration
Compliance and Billing Burn
Compliance and billing hit owner pay before cash shows up as profit. This driver includes documentation, eligibility checks, audit prep, survey readiness, billing timing, accreditation work, admin labor, and EHR workflows. Here’s the quick math: fixed monthly spend is $3,400 from $400 compliance fees, $1,800 EHR licensing, and $1,200 professional services, before billing labor.
Billing payroll also rises from 0.5 FTE to 1.5 FTE at a $65,000 salary base, or about $32,500 to $97,500 a year. That means about $2,708 to $8,125 per month in payroll. If claims lag or documentation fails, cash flow tightens fast, and owner draws get pushed back even when care volume is strong.
Track Billing Quality First
Measure the inputs that move cash: claim count, days to bill, denied claims, eligibility pass rate, audit findings, and time spent on chart cleanup. If documentation is late, billing slows, and that delay lands straight in working capital. Compliance spend is not optional here; it is a required operating cost, so the real win is reducing avoidable rework.
- Track bill lag by payer.
- Review denials weekly.
- Close charts same day.
- Test eligibility before start.
- Keep survey files audit-ready.
Use the EHR to cut manual touches, then staff billing to match claim flow, not guesswork. If one billing FTE can’t keep up, claims age and cash comes in late. If documentation quality stays high, the same fixed cost base supports faster collections and protects owner income.
5
Operating Reserves And Reinvestment
Operating Reserves Before Owner Pay
When cash is tight, the owner does not get paid first. Operating reserves cover delayed reimbursement, payroll, compliance response, hiring ahead of growth, equipment needs, quality work, debt service, and surprises, so distributions only happen after care is funded. The model shows $113M operating profit before reserves in Year 1 and $1,121M in Year 5, but the reserve rate is not supplied, so it should stay editable.
Set a Reserve Rule Before Distributions
Track reserve days, not just profit. Use a simple rule tied to payroll timing, billing lag, and growth spend, then hold back enough cash for compliance, overtime, equipment, and debt service before any owner draw. If reimbursement slows or census grows fast, reserves protect patient care and keep the business from paying out cash it needs next week.
6
Compare hospice owner income scenarios without promising pay
Owner income scenarios
Income changes fast here because staffing, utilization, and fixed overhead do not scale at the same pace. These cases show how owner pay shifts from a lean launch to a larger, steadier operation.
| Scenario | Low CaseOwner-operated | Base CaseManager-led | High CaseManager-led upside |
|---|---|---|---|
| Launch model | This is the lower-income path if Year 1 stays small and the owner is still covering day-to-day work. | This is the modeled middle path where the care team is steadier and the owner is less tied to daily delivery. | This is the stronger earnings path if the business reaches the Year 5 scale and keeps utilization high. |
| Typical setup | Year 1 scale with 1 physician, 3 registered nurses, 5 certified aides, 1 social worker, and 1 spiritual counselor, plus fixed rent, insurance, and software. | Year 3 scale with 2 physicians, 8 registered nurses, 13 certified aides, 3 social workers, and 2 spiritual counselors, plus higher payroll and utilization. | Year 5 scale with 3 physicians, 15 registered nurses, 25 certified aides, 5 social workers, and 3 spiritual counselors, with larger payroll and service volume. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $1.0M - $1.1MReserve risk | $4.5M - $4.6MStable base | $10.8M - $11.2MUpside case |
| Best fit | Use this to stress-test an owner-operated launch with thin reserve coverage and slower staffing ramp. | Use this for a manager-led plan that assumes a more mature census and tighter operating rhythm. | Use this to test upside under a manager-led model with strong volume and controlled overhead. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions; actual owner pay depends on reserves and unmodeled clinical payroll.
Related Products
- Hospice Care Porter's Five Forces Analysis
- Hospice Care BCG Matrix
- Hospice Care Business Model Canvas
- 7 Critical KPIs for Scaling Hospice Care Operations
- Hospice Care Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Hospice Care Profitability and Margins
- Analyzing the Monthly Running Costs to Operate a Hospice Care Program
- How Much Does It Cost To Start Hospice Care? $884K Plan
- Hospice Care Financial Model Template in Excel
- How To Open A Hospice Care Business In 6–12+ Months
- How to Write a Hospice Care Business Plan: 7 Essential Steps
- Hospice Care Marketing Mix
- Hospice Care Marketing Plan
- Hospice Care Business Proposal
- Hospice Care PESTEL Analysis
- Hospice Care Pitch Deck Example Editable PPTX
- Hospice Care Business SWOT Analysis
- Hospice Care Value Proposition Canvas
Frequently Asked Questions
A hospice owner’s take-home depends on profit after reserves, not revenue In the supplied model, Year 1 revenue is $199 million and modeled operating profit is about $113 million before reserves, taxes, debt, and unprovided clinical payroll If the owner also serves as Executive Director, the model includes a $150,000 salary line for that role