 Time to Open3-6 monthsSetup window
Time to Open3-6 monthsSetup windowHow To Start A House Call Doctor Service In 90 To 180 Days

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open3-6 monthsSetup window  Launch Sequence7 stagesCompliance first
Launch Sequence7 stagesCompliance first Key BottleneckCredentialing gateBilling approval
Key BottleneckCredentialing gateBilling approval First Revenue StepPaid home visitsBooking live
First Revenue StepPaid home visitsBooking live


Key Takeaways
- Get licensure, insurance, and compliance ready before bookings.
- Match staffing and coverage to visit demand by role.
- Keep service area tight to protect visit productivity.
- Set up EHR, supplies, and referral flow first.
Time to Open3-6 monthsSetup windowLaunch Sequence7 stagesCompliance firstKey BottleneckCredentialing gateBilling approvalFirst Revenue StepPaid home visitsBooking liveLaunch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12Week 13Week 14
Legal / compliance
- Form entity
- Licensure review
- Place malpractice coverage
- Set HIPAA policies
- Review prescribing rules
Clinical operations
- Define visit types
- Build triage flow
- Write care protocols
- Set escalation rules
- Test documentation
Technology
- Select EHR
- Set scheduling
- Enable mobile charting
- Configure payments
- Test billing handoff
Staffing / training
- Hire Medical Director
- Recruit clinicians
- Hire coordinators
- Train staff
- Confirm coverage
Vendors / equipment
- Order supplies
- Secure diagnostics
- Customize vehicle
- Install refrigeration
- Set telecoms
Referral / launch
- Payer credentialing
- Build referral list
- Meet discharge planners
- Soft launch outreach
- Opening review
Why test the House Call Doctor Service model before launch?
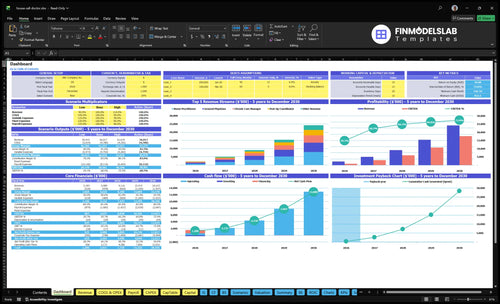
Before launch, House Call Doctor Service Financial Model Template checks visit volume, staffing, cash, and break-even. Open it.
Financial model highlights
- Month 1-60 dashboard
- 11 to 73 clinical roles
- $181,880 monthly revenue
- 20% direct costs
- $36,700 fixed monthly
- $150-$300 visit pricing
- Credentialing delay risk
- Travel time drag
- Underfilled route warning
How long does it take to start a house call doctor service?
A House Call Doctor Service usually takes 90 to 180 days to start. A private-pay pilot is the faster path because it needs licensed providers, malpractice coverage, EHR, scheduling, supplies, payment capture, and local referrals; insurance-heavy launches take longer because credentialing, claims setup, and contracting can delay the first reimbursed visits. The Year 1 model assumes 11 clinical roles and about 916 monthly visits at capacity, so launch timing has to match staffed routes, not just signed paperwork.
Fast launch path
- 90 to 180 days is practical
- Private-pay pilot starts faster
- Need licensed providers first
- Set up payment capture early
Slow launch blockers
- Insurance credentialing slows visits
- Claims rules add setup time
- Malpractice underwriting can delay opening
- 916 monthly visits need staffed routes
What are the biggest house call doctor launch mistakes?
The biggest launch mistakes in a House Call Doctor Service are a fuzzy service area, weak triage, thin malpractice coverage, poor EHR charting, no backup provider, and no referral pipeline. If the team cannot confirm who goes, where they go, what they treat, how they chart, how they escalate, and how payment is captured, the practice is not ready. Year 1 capacity is already capped at 65% for general physicians, 60% for nurse practitioners, 50% for geriatric specialists, 70% for chronic care managers, and 55% for post-op coordinators, so missed scheduling discipline slows the ramp fast.
Launch risks
- Unclear service area
- Travel time undercounted
- Triage rules too weak
- Malpractice coverage incomplete
Readiness checks
- EHR workflow works
- Backup provider is set
- Referral pipeline exists
- Payment capture is clear
What are the requirements to start a house call doctor service?
To start a House Call Doctor Service, clear state launch gates first: entity registration, licensed physicians or approved advanced practice providers, home-visit malpractice coverage, HIPAA-compliant workflows, prescribing rules, consent forms, documentation standards, billing setup, and payer enrollment if taking insurance; see How Increase House Call Doctor Service Profits? for the profit side. Do not book first visits until triage, EHR access, mobile documentation, malpractice coverage, and emergency escalation are live, because the model carries 10 FTE at $280,000/year each, or about $233,333/month in clinician cost from Month 1.
Launch Gates
- Register the medical business entity
- Confirm state medical practice rules
- Secure home-visit malpractice insurance
- Set HIPAA-compliant patient workflows
Care Controls
- Use licensed physicians or approved APPs
- Verify prescribing and controlled-substance rules
- Prepare consent and clinical documentation
- Complete billing and payer enrollment
Confirm readiness before the first home visit is booked
Launch readiness checklist
Use this go-live approval checklist to confirm the house call doctor service is ready before opening.
Compliance
- Business registration filedCritical
The practice needs a legal entity before contracts, banking, and billing can start.
- State medical licenses verifiedCritical
Physicians and clinicians must be licensed for the states where home visits happen.
- Malpractice bound for home visitsCritical
Home visit care should not start without coverage sized for mobile medical work.
Clinical rules
- Consent forms approvedHigh
Patients need clear consent before in-home exams, treatment, and data use.
- HIPAA policy activeCritical
Protected health data must stay secure in the field, in chat, and in records.
- Triage rules approvedCritical
Clear triage keeps urgent cases out of the wrong care path.
- Prescribing rules reviewedHigh
Prescribing steps must match state law and the service's scope of care.
- Documentation standards setHigh
Consistent notes support billing, follow-up care, and legal defense.
Digital flow
- EHR configured for mobile chartingCritical
Clinicians need chart access in the field or visits will slow down.
- Scheduling and intake testedCritical
The intake path must capture patient details before the first house call.
- Payment and claims flow testedHigh
Payment capture and claim steps must work before revenue starts.
Vendors
- Medical supplies vendor confirmedHigh
Core supplies must arrive on time or visits will get delayed.
- Diagnostic partner contract activeHigh
Lab and imaging handoffs need a live partner before launch.
- Vehicle fleet readyCritical
Reliable vehicles are the service line, so downtime hurts visit volume fast.
- Waste di sposal pickup setHigh
Medical waste handling must be set before the first procedure visit.
Team
- Medical Director appointedCritical
The model assumes one Medical Director with full-year coverage.
- Clinician roster matches forecastCritical
The mix must support the Year 1 visit plan and service lines.
- Backup coverage confirmedCritical
Launch is not ready if sick-day and after-hours coverage is weak.
Demand and cash
- Senior referral channels readyHigh
Senior living, home health, and discharge teams can drive the first bookings.
- Direct booking path liveHigh
Patients need a simple way to request a house call without delay.
- Volume plan hits 916 visitsCritical
Year 1 capacity should align to about 916 visits per month.
- Cash runway covers Month 2Critical
The plan should absorb the Month 2 cash trough before launch stress rises.
Want the six house call doctor launch drivers?
1Regulatory Readiness
Day-1 gateDay-one licensure, malpractice, HIPAA, and consent rules cut denial risk and prevent stop-start delays.
2Clinical Coverage
11 cliniciansYear 1 staffing of 3 physicians, 4 nurse practitioners, and support roles keeps coverage steady.
3Service Routing
65% to 70%At 65% to 70% utilization, routing stays realistic and avoids wide-area drag.
4EHR Workflows
$4K/moWith $4K monthly software and IT, live scheduling and billing handoff speed cleaner claims.
5Field Ops
Field readyStandard kits, restocking, and vehicle support cut missing-supply risk in the field.
6Referral Channels
$4.5K/moA focused referral list and $4.5K monthly outreach fill live slots faster.
Regulatory And Insurance Readiness
Day-One Compliance Gate
A house call doctor service cannot safely open until state medical licensure, malpractice coverage for home visits, HIPAA rules, consent forms, prescribing rules, and documentation standards are all live. If you book visits before those pieces are set, you raise denial risk, expose the practice to unsafe care, and create stop-start delays on day one.
For a mobile practice, the launch gate is simple: prove the provider can legally treat in the state, show coverage is bound, and confirm the medical record and privacy rules are ready. If insurance is accepted, payer enrollment must also be in motion, because claims can’t run cleanly without it. One missing approval can block first revenue.
Lock Coverage Before Booking
Before opening the schedule, confirm provider scope, bind malpractice coverage, and test the patient intake path for HIPAA and consent. That means privacy workflows, signed forms, prescribing checks, and a clear rule for what goes into the medical record.
The launch setup already carries fixed tools like $2,200 per month for EHR and scheduling software plus $1,800 per month for telecom and IT support, so don’t spend on live ops until the compliance side is ready. A clean start lowers claim denials and keeps visits legal from the first house call.
1
Clinical Staffing And Coverage
Safe Coverage Plan
House call staffing is a coverage problem first. The Year 1 plan uses 3 general physicians, 4 nurse practitioners, 1 geriatric specialist, 2 chronic care managers, and 1 post-op coordinator, plus a Medical Director at $280,000 a year. If the visit mix is not matched to these roles before launch, you get open slots, missed calls, and cancelled home visits on day one.
The readiness test is simple: defined visit types, backup coverage, triage rules, escalation paths, and schedule blocks matched to demand. Provider availability is the bottleneck, especially if one clinician is loaded with too many urgent visits. When that happens, the business can still be “open” on paper but unable to keep appointments in the field.
Map Backup Before Opening
Before the first patient books, verify who handles routine, urgent, chronic care, and post-op visits, and who steps in after hours. The launch plan should lock credential checks, onboarding, route assignment, visit protocols, and after-hours coverage decisions before the schedule goes live. One clean rule set is better than a full calendar with no safe backup.
- Match visit types to each clinician.
- Document escalation and handoff rules.
- Block time for urgent overflow.
- Confirm after-hours coverage ownership.
Test the schedule against real demand before opening. If the team cannot absorb one clinician’s sick day or a spike in urgent calls, first-day service slips fast. The goal is not just staffing on paper; it is reliable appointments and fewer cancelled home visits from the first week.
2
Service Area And Routing
Service Area and Routing
This launch driver decides whether the practice can open on time and make visits work from day one. A defined territory, travel buffers, and clear appointment windows keep late arrivals down and protect patient experience. If the service area is too wide, providers spend more time driving than seeing patients, and the first-month revenue ramp slows because fewer visits get completed.
Here’s the quick math: Year 1 utilization is assumed at 65% for general physicians, 60% for nurse practitioners, 50% for geriatric specialists, 70% for chronic care managers, and 55% for post-op coordinators. That means routing has to match real daily capacity by role, not just demand. One-line rule: if the map is too big, the schedule breaks.
Set the Route Before the Calendar
Before opening, map zip codes, cluster referrals, and set a minimum route density so each drive creates enough completed visits. Build separate rules for urgent versus scheduled visits, then block admin time so dispatch, charting, and patient calls do not eat the day. The launch test is simple: can each role hit its planned visit load without forcing late starts?
- Draw the launch territory by zip code.
- Group patients by drive time.
- Reserve buffers between visits.
- Block admin time every day.
- Test urgent visit rerouting rules.
What this setup hides is the cost of overreach. If routing is loose, providers miss windows, finish fewer visits, and spend more time in transit. Tight service-area planning gives cleaner first-week execution and a stronger signal that the business can serve patients reliably from day one.
3
EHR And Mobile Workflows
Mobile EHR Workflow
A house call doctor service cannot open on time if the EHR still needs patching. Day-one workflow has to cover live scheduling, intake forms, mobile chart access, phone or telehealth triage, payment capture, billing handoff, secure messaging, and documentation templates, or clinicians end up charting after the visit and billing from incomplete records.
Here’s the quick math: the fixed source cost is $2,200 per month for EHR and scheduling software plus $1,800 per month for telecommunications and IT support, or $4,000 per month before visit revenue. If field access testing or claims handoff slips, cash burns while claims slow, and launch delays can turn into billing denials and shaky patient handoffs.
Launch Setup
Build the workflow before the first appointment is booked. Set visit templates, consent capture, coding rules, claims handoff, and field access testing in that order, then make one clinician and one biller run a real visit from phone intake to closed note. If any step fails, fix it before go-live; after-the-fact documentation is the main bottleneck.
- Test charting on phone and tablet.
- Confirm consent before each visit.
- Match codes to note templates.
- Send one clean claim end-to-end.
- Verify secure messaging in the field.
4
Supplies, Vendors, And Field Operations
Field Supplies Ready
If the bag is not packed, the practice is not open. House call visits depend on a ready field kit: medical bag, PPE, diagnostic tools, a specimen handling plan, a medication policy, a waste disposal process, a vehicle plan, a restocking workflow, and vendor contacts. Miss one piece and a booked visit can turn into a delay, a reschedule, or a safety issue on day one.
Here’s the quick math: Year 1 medical supplies and disposables are 45% of revenue, lab and diagnostic fees are 55%, fuel and maintenance are 6%, and the vehicle fleet lease is $8,500 per month. That means field operations can burn cash fast, so the launch plan needs tight control before the first patient.
Pack, Restock, Test
Before opening, set supply par levels, assign a restock owner, and test specimen pickup while the schedule is still soft. The goal is simple: every clinician leaves with the same kit and the same replenishment rules. One clean handoff beats one emergency store run.
Verify these inputs before go-live:
- Packed bag by visit type
- Vendor contacts and order timing
- Medication and waste rules
- Vehicle and fuel workflow
- Specimen pickup backup
If specimen pickup or restocking is weak, visits slow down, supplies run out in the field, and first-day capacity falls below plan.
5
Referral And First-Revenue Channels
Referral Channels
This driver decides whether the first visits turn into cash or just lead lists. A house call doctor service should only market into live schedule slots and a defined service area, because demand outside the route map or provider coverage creates cancellations, wasted calls, and slow first revenue. One booked visit is better than ten unbookable inquiries.
The source figure sets $4,500 per month for marketing and patient outreach, so the spend only works if partner scripts, referral forms, service menus, response-time rules, and a private-pay booking flow are ready before outreach starts. If those pieces lag, staff spend time answering requests that cannot be served that day.
Book Only What You Can Cover
Before opening, match outreach to the number of visits the clinicians can actually cover that week. Confirm route map, visit windows, and who can take urgent versus scheduled calls, then limit outreach to the partner types that fit the map: senior living communities, home health agencies, discharge planners, concierge practices, local employers, and direct-to-patient campaigns.
Build a simple intake path: source, eligibility, private-pay quote, same-day slot, and follow-up. Test response times before launch; if a lead cannot be answered and booked into a live slot, it is not a launch-ready channel. One clean referral flow beats five half-open channels.
- Confirm service area by zip code.
- Set response-time rules before outreach.
- Use one referral form format.
- Train staff on booking steps.
- Test private-pay payment flow.
6
Related Products
- House Call Doctor Service Porter's Five Forces Analysis
- House Call Doctor Service BCG Matrix
- House Call Doctor Service Business Model Canvas
- What Are The 5 KPI Metrics For House Call Doctor Service Business?
- House Call Doctor Service Business Plan Template in Pre-Written Word
- How Increase House Call Doctor Service Profits?
- What Are Operating Costs For House Call Doctor Service?
- House Call Doctor Service Startup Costs: $85K CAPEX Plus Runway
- House Call Doctor Service Financial Model Template in Excel
- How Much House Call Doctor Owners Make: $103M Year 1 Profit
- How Do I Write A Business Plan For House Call Doctor Service?
- House Call Doctor Service Marketing Mix
- House Call Doctor Service Marketing Plan
- House Call Doctor Service Business Proposal
- House Call Doctor Service PESTEL Analysis
- House Call Doctor Service Pitch Deck Example Editable PPTX
- House Call Doctor Service Business SWOT Analysis
- House Call Doctor Service Value Proposition Canvas
Frequently Asked Questions
Yes, one licensed physician can start a smaller pilot if malpractice coverage, HIPAA workflows, documentation, supplies, and backup coverage are ready The planning case is larger, with 11 Year 1 clinical roles and a 10 FTE Medical Director A solo launch should use a tighter service area and fewer visit types