 Owner income≈$1.13M
Owner income≈$1.13MHyperbaric Oxygen Therapy Clinic Owner Income: $1128M Year 1 EBITDA

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income≈$1.13M  Net margin49.6%
Net margin49.6% Revenue for target pay≈$2.27M
Revenue for target pay≈$2.27M Business difficultyHard
Business difficultyHard


Key Takeaways
- Higher chamber utilization drives the fastest EBITDA gains.
- Net revenue per session compounds across monthly volume.
- Underused chambers turn equipment capex into cash drag.
- Payroll and overhead set the break-even floor.
Owner income≈$1.13MNet margin49.6%Revenue for target pay≈$2.27MBusiness difficultyHardWant to estimate your HBOT clinic owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Actual owner income depends on revenue, margins, payroll, reserves, debt, and owner pay choices. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to stress-test owner income in the Hyperbaric Oxygen Therapy Clinic financial model?
Capacity, pricing, payroll, fixed costs, fees, reserves, and take-home assumptions in Hyperbaric Oxygen Therapy Clinic Financial Model Template; open it.
Owner-income model highlights
- Owner take-home first
- Revenue, staffing, capex tabs
- Opex, cash flow, scenarios
- Two $350k chambers
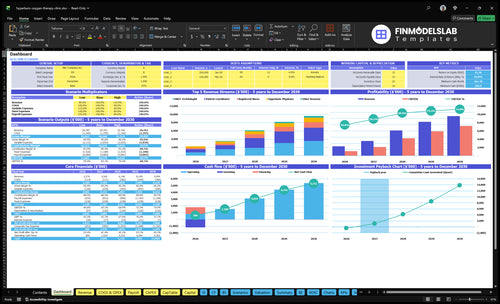
- 16-month payback, $12M capex
- Minimum cash: $166k
- Month 1 break-even
What HBOT clinic operating costs reduce owner income most?
Payroll is the biggest drag on owner income in a Hyperbaric Oxygen Therapy Clinic, followed by medical oversight, rent, insurance, and equipment funding. Year 1 payroll is $550k, fixed overhead is $198k/month, and variable costs start at 120% of revenue, so profits can get squeezed fast; see What Is The Estimated Cost To Open And Launch Your Hyperbaric Oxygen Therapy Clinic? for the startup capital context. One line: cash has to cover losses and capex before owners take distributions.
Main cost drains
- Payroll: $550k in Year 1
- Payroll: $945k by Years 4-5
- Lease: $12k monthly facility cost
- Malpractice: $3k monthly insurance
Cash pressure points
- Utilities: $15k monthly
- Software: $800 monthly
- Variable costs: 120% to 98% of revenue
- Capex: $12M, so reserves matter
How does cash pay versus insurance change HBOT clinic income?
For a Hyperbaric Oxygen Therapy Clinic, cash pay usually gives cleaner timing and easier forecasting, because you get paid closer to the session date. Use net collected revenue, not list price: at $300-$500 per session in Year 1 and $360-$600 by Year 5, payment processing fees of 20% in Year 1 and 18% by Year 5 cut the take-home amount fast. Insurance can raise volume, but income depends on allowed amounts, documentation, denials, and collection lag, so compliance review matters.
Cash pay
- $300-$500 per session in Year 1
- $360-$600 per session by Year 5
- 20% fee in Year 1
- 18% fee by Year 5
Insurance
- Use allowed amounts, not list price
- Watch denials and paperwork delays
- Expect collection lag in cash flow
- Keep compliance review in the loop
How many HBOT sessions does a clinic need to be profitable?
A Hyperbaric Oxygen Therapy Clinic needs about 188 completed paid sessions per month to break even in Year 1 at the model’s $396 average net price; quick math: 188 × $396 = $74,448 monthly net revenue. The 188-session target implies the cost inputs need validation because 120% variable cost load and $656k monthly overhead don’t reconcile; at the modeled 478 sessions/month, utilization still looks well above break-even, and retention should be tracked with What Is The Current Customer Satisfaction Level For Hyperbaric Oxygen Therapy Clinic?.
Break-even math
- Target: 188 paid sessions/month
- Net price: $396 per session
- Break-even revenue: $74,448/month
- Modeled volume: 478 sessions/month
Inputs to watch
- Use completed sessions, not bookings
- Model cancellations and session length
- Track payer mix by net price
- Check capacity from 600%-650% toward 800%-900%
Want the six HBOT clinic income drivers?
1
478-1,718/moSession Volume
More booked sessions spread the fixed clinic base, so each added treatment lifts owner income fast.
2
$396-$465Net Revenue
A higher net take per session compounds fast because each treatment adds margin with limited extra cost.
3
$700KChamber Capacity
Two chambers set the ceiling on throughput, and higher capacity lets the site earn more from the same overhead.
4
$550K-$945KPayroll Load
Clinical staffing is the biggest cost swing, so the team mix has a direct pull on take-home profit.
5
$19.8K/moFixed Overhead
Lease, utilities, insurance, and software keep running, so steady utilization is what covers the base.
6
5.0%-4.0%Referral Demand
Lower patient-acquisition spend keeps more of each billed dollar in the clinic once referrals start flowing.
Hyperbaric Oxygen Therapy Clinic Core Six Income Drivers
Paid Treatment Volume And Chamber Utilization
Paid Treatment Volume
Paid sessions are the main volume lever because each filled slot adds revenue after fixed costs are already covered. In the model, completed paid sessions rise from about 478/month in Year 1 to 1,718/month in Year 5, or about 3.6x. That is why higher utilization usually lifts owner profit and cash available for draw faster than price changes alone.
What this estimate hides is the drag from cancellations, session length, chamber downtime, and operating hours. Modeled source capacity moves from roughly 600%-650% early to 800%-900% later, so unused slots matter. EBITDA, or earnings before interest, taxes, depreciation, and amortization, improves fastest when chambers stay full and turns stay tight.
Track Fill Rate Weekly
Measure booked slots, completed sessions, cancellation rate, average session length, and chamber downtime each week. The math is simple: paid sessions × net revenue per session drives monthly revenue, so even a small fill-rate gain can change take-home income fast.
- Cut late cancels first.
- Shorten chamber turnover.
- Book peak hours tightly.
- Track downtime by chamber.
When utilization rises, the extra revenue usually drops to profit quickly because lease, payroll, and supervision costs are already in place. If no-shows climb or onboarding slows, owner pay falls even when demand looks strong.
1
Net Revenue Per Session And Payer Mix
Net Revenue Per Session And Payer Mix
Net revenue per session is what the clinic actually keeps after allowed amounts, collection rate, denials, and payment timing. In this model, average net revenue rises from about $396 per session in Year 1 to about $465 per session by Year 5, while source pricing runs $300-$500 in Year 1 and $360-$600 in Year 5. Small swings here hit owner pay fast because every session moves the margin line.
For a hyperbaric oxygen therapy clinic, payer mix matters because some sessions pay cleanly and others get reduced, delayed, or denied. Here’s the quick math: a higher collection rate and fewer denials lift cash per treatment, and that compounds across hundreds of monthly sessions. A $20-$30 swing per session can change monthly profit more than a small staffing tweak.
Track Allowed Amounts, Collections, And Denials
Measure gross charge, allowed amount, cash collected, denial rate, and days to collect by payer and by treatment type. Split medical referrals from cash-pay or wellness sessions, since payer mix changes the cash profile and the owner’s take-home. If one payer pays slower or denies more, it drags net revenue even when volume holds steady.
- Track net revenue per session weekly.
- Review denials by payer and reason.
- Compare pricing to $300-$500 and $360-$600.
- Watch timing on every reimbursement cycle.
2
Chamber Count And Equipment Leverage
Chamber Count And Equipment Leverage
More chambers lift income only when booked sessions fill the extra slots. The source model includes two chambers at $350k each, plus a $120k oxygen system, $200k build-out, and $80k monitoring equipment, within $12M total capex. If utilization stays low, that equipment adds financing, maintenance, and staff load before it adds profit.
The key input is chamber-hours sold versus chamber-hours available. High volume spreads fixed equipment cost across more treatments and helps owner pay; low volume turns capex into a cash drag because the clinic still pays for space, service, and coverage even when slots sit empty. One empty chamber is still an expensive room.
Fill Slots Before Adding Capacity
Track utilization, downtime, cancellations, and staffed operating hours before you buy another chamber. If the second chamber does not lift filled slots fast enough, the added asset can hurt cash flow more than it helps margin. The clean test is simple: does incremental capacity bring enough paid sessions to cover financing, maintenance, and staffing?
Forecast each chamber with the same discipline: expected sessions per day, service reserve, and labor coverage by shift. Keep expansion tied to referral flow and booked volume, not hope. If chamber count rises faster than patient demand, owner income usually falls even while revenue looks bigger on paper.
3
Staffing And Medical Supervision Costs
Staffing And Medical Supervision Costs
Payroll is the gatekeeper for owner pay. In Year 1, payroll is $550k, including a $220k Medical Director, $85k Lead HBOT Technologist, $70k HBOT Technologist, $75k Registered Nurse, $55k Patient Care Coordinator, and $45k Administrative Assistant. Those roles have to be covered before treatment revenue turns into profit.
By Years 4-5, payroll rises to $945k, or about $395k more than Year 1. That is a 72% increase. If staffing grows before paid session volume and chamber use catch up, the added labor cost compresses margin and delays owner draws.
Staff To Volume, Not Hope
Track payroll against completed paid sessions and staffed chamber hours. The key question is simple: are you paying for enough volume to support the team? Keep a monthly watch on role-by-role payroll, coverage gaps, cancellations, and chamber downtime so headcount only rises when utilization is already strong.
- Measure payroll per paid session.
- Watch staffed hours vs. filled slots.
- Delay hires until volume holds.
- Review coverage before adding shifts.
4
Fixed Overhead And Facility Economics
Fixed Overhead Floor
Fixed overhead is the monthly cost base that has to be covered before the owner pays themselves. Here, fixed costs total $198k/month, led by a $12k lease, $3k malpractice insurance, $15k utilities, and $1k medical cleaning, plus software, supplies, and professional services.
When payroll is added, the Year 1 fixed burden is about $656k/month. That’s why the clinic’s break-even floor sits at about 188 sessions: lower overhead cuts the session count needed to cover cash outflow and protects reserves when volume slips.
Control the Monthly Burn
Track fixed costs by line item every month: lease, insurance, utilities, cleaning, software, and admin spend. Then compare the total to paid-session volume, because every extra dollar of fixed cost raises the number of sessions needed before the owner sees profit.
- Review lease and utility bills monthly
- Separate fixed vs. variable payroll
- Test vendor renewals before signing
- Watch break-even against paid sessions
Here’s the quick math: if fixed overhead falls, the clinic needs fewer billed sessions to cover the same cash drain, so owner draw starts sooner and reserve pressure eases. If overhead rises faster than volume, profit gets squeezed even when chambers stay busy.
5
Referral Demand And Patient Acquisition
Referral Demand Quality
Referral demand means how many qualified patients get into the intake flow and start treatment. In this model, marketing and patient acquisition run at 50% of revenue in Year 1 and fall to 40% by Year 5, so weak referral flow can drain cash before chambers fill. The goal is simple: keep booked sessions steady enough that revenue covers acquisition, payroll, and overhead.
The main inputs are referral volume, local search leads, intake follow-up, and repeat treatment plans. The model starts with $25k in marketing assets, but the real test is conversion into filled sessions. One missed referral is not just lost revenue; it also leaves fixed clinic time unused.
Track Conversion, Not Just Leads
Measure referrals received, consults booked, show rate, treatment starts, and completed sessions. Here’s the quick math: if acquisition stays at 50% of revenue, then half of each dollar earned is already spoken for before owner pay. By Year 5, dropping that to 40% improves cash flow, but only if demand stays compliant and steady.
- Track cost per booked patient.
- Track cost per completed session.
- Review no-shows weekly.
- Keep referral scripts compliant.
What this hides: if intake follow-up is slow, or repeat plans are weak, acquisition spend rises while utilization falls. That squeezes margin and delays owner draw. Strong referral flow keeps chambers full without letting marketing outrun revenue.
6
Compare low, base, and high HBOT clinic owner income scenarios
Owner income scenarios
Owner income moves with session volume, staffing, and variable spend. The low, base, and high cases mirror Year 1, Year 3, and Year 5 operating scales.
| Scenario | Low CaseRamp path | Base CaseScale path | High CaseUpside path |
|---|---|---|---|
| Launch model | Owner income follows a lower Year 1 ramp. | Owner income follows the modeled Year 3 operating case. | Owner income follows the stronger Year 5 maturity case. |
| Typical setup | The clinic runs at about 478 sessions a month, with one physician, two technologists, one nurse, one coordinator, and Year 1 EBITDA as the income proxy. | The clinic reaches about 1,179 sessions a month, with higher staffing, more support roles, and Year 3 EBITDA as the income proxy. | The clinic reaches about 1,718 sessions a month, carries full staffing, and uses Year 5 EBITDA as the income proxy. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $1.13MYear 1 ramp | $4.23MYear 3 scale | $7.19MYear 5 maturity |
| Best fit | Use this to stress test a slower launch and lighter utilization. | Use this as the main planning case for a working clinic with steady demand. | Use this to test upside if demand stays strong and the clinic runs near full capacity. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Hyperbaric Oxygen Therapy Clinic Porter's Five Forces Analysis
- Hyperbaric Oxygen Therapy Clinic BCG Matrix
- Hyperbaric Oxygen Therapy Clinic Business Model Canvas
- 7 Critical KPIs for a Hyperbaric Oxygen Therapy Clinic
- Hyperbaric Oxygen Therapy Clinic Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Hyperbaric Oxygen Therapy Clinic Profitability
- Analyzing Monthly Running Costs for a Hyperbaric Oxygen Therapy Clinic
- Hyperbaric Oxygen Therapy Clinic Startup Costs: $656k Month 1 Burn
- Hyperbaric Oxygen Therapy Clinic Financial Model Template in Excel
- How to Open a Hyperbaric Oxygen Therapy Clinic in 4-9 Months
- How to Write a Business Plan for a Hyperbaric Oxygen Therapy Clinic
- Hyperbaric Oxygen Therapy Clinic Marketing Mix
- Hyperbaric Oxygen Therapy Clinic Marketing Plan
- Hyperbaric Oxygen Therapy Clinic Business Proposal
- Hyperbaric Oxygen Therapy Clinic PESTEL Analysis
- Hyperbaric Oxygen Therapy Clinic Pitch Deck Example Editable PPTX
- Hyperbaric Oxygen Therapy Clinic Business SWOT Analysis
- Hyperbaric Oxygen Therapy Clinic Value Proposition Canvas
Frequently Asked Questions
In this model, the owner income proxy is EBITDA, or earnings before interest, taxes, depreciation, and amortization It is $1128M in Year 1 and $7188M in Year 5 Actual owner take-home is lower if the clinic pays taxes, debt service, equipment reserves, or reinvests cash