Implantable Loop Recorder Startup Costs: $903K Funding Plan

You’re opening an Implantable Loop Recorder service, so the budget has to cover more than procedure equipment This outline uses researched US planning assumptions for the first operating year, including $385,000 in CAPEX, $903,000 minimum cash in Month 1, and launch costs tied to device inventory, monitoring technology, payer setup, staffing, and working capital These are planning estimates, not vendor quotes, reimbursement guarantees, or a full operating forecast
ILR Service CAPEX Calculator Objective
Startup CAPEX Calculator
Estimates capitalized startup assets only for an implantable loop recorder service launch, before any non-CAPEX funding needs.
Exclusions This calculator covers capitalized startup assets only. It excludes payroll runway, monthly rent, malpractice, IT support, marketing, working capital, debt service, deposits, payer enrollment delay, replenishment stock, and other operating costs.
What should the CAPEX view show?
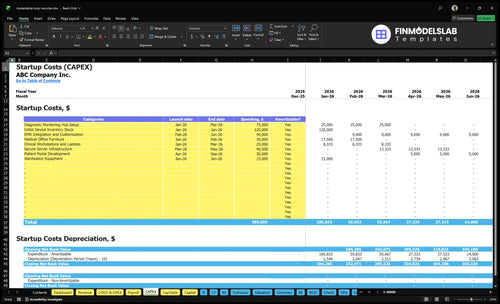
The Implantable Loop Recorder Services Financial Model Template shows the CAPEX tab, startup costs, launch timing, depreciation/amortization, and assumptions—review it.
Screenshot highlights
- $385k CAPEX base
- $903k month-one cash
- $120k inventory
- $75k monitoring hub
- $45k EMR integration
- $915k Year-1 payroll
- $39k monthly fixed costs
- Depreciation and amortization
- Payer delays and collections
- Staffing ramp and capacity
How much money do I need to open an ILR service?
You need at least $903,000 in Month 1 cash to open an Implantable Loop Recorder Services business; don’t plan around equipment alone. The funding stack should cover $385,000 in CAPEX, launch payroll, fixed expenses, insurance, credentialing, and collections runway; see How To Launch Implantable Loop Recorder Services Business? for the setup path.
Cash Needed
- $903,000 minimum Month 1 cash
- $385,000 CAPEX for setup
- $39,000 monthly fixed expenses
- Fund insurance, credentialing, and collections lag
Runway Math
- $915,000 Year 1 payroll
- $76,250 payroll per month
- 2,065 modeled procedures per month
- $2.139 million modeled Year 1 revenue
What hidden costs of starting an ILR service affect working capital?
If you’re sizing Implantable Loop Recorder Services, the hidden costs hit working capital fast: $39,000 per month from malpractice insurance, HIPAA-compliant software, IT security, marketing, office rent, and ASC access, before payroll or device stock. If you want the KPI view, see What Are The 5 KPIs For Implantable Loop Recorder Services Business?; these costs sit outside the $385,000 CAPEX total and need separate funding. Credentialing, payer enrollment lag, claim denials, cybersecurity, device carrying costs, staff onboarding, and launch payroll all squeeze cash early.
Monthly cash burn
- $8,500 malpractice insurance
- $3,200 HIPAA-compliant software
- $2,800 IT security and support
- $4,500 professional marketing services
Working-capital traps
- $5,000 administrative office rent
- $15,000 ASC access lease
- Credentialing delays cash collection
- Claim denials slow reimbursement
What is the biggest cost to start an implantable loop recorder service?
The biggest named startup cost for implantable loop recorder services is device inventory at $120,000. If you launch lean, though, cash pressure can shift to monitoring hub setup at $75,000, EMR integration at $45,000, and server infrastructure at $40,000, plus staffing ramp. In Year 1, variable costs can also include 120% implantable device procurement, 25% disposable surgical kits, 45% billing and RCM fees, and 10% remote monitoring data fees.
Biggest CAPEX
- $120,000 device inventory.
- $75,000 monitoring hub setup.
- $45,000 EMR integration.
- $40,000 server infrastructure.
Year 1 cash load
- 120% implantable device procurement.
- 25% disposable surgical kits.
- 45% billing and RCM fees.
- 10% remote monitoring data fees.
Implantable Loop Recorder Startup Cost Breakdown Table
Startup cost summary
This table separates CAPEX from excluded launch cash for an implantable loop recorder service.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| Initial Device Inventory Stock | $120,000 | Device purchase volume and supplier pricing | Yes |
| Diagnostic Monitoring Hub Setup | $75,000 | Monitoring equipment and setup scope | Yes |
| EMR Integration and Customization | $45,000 | Software integration and workflow build | Yes |
| Secure Server Infrastructure | $40,000 | Secure hosting and data infrastructure | Yes |
| Medical Office Furniture, Workstations, Patient Portal, and Sterilization Equipment | $105,000 | Clinic buildout and launch systems | Yes |
| Minimum Cash Reserve | $903,000 | Month 1 reimbursement lag and launch losses | No |
Implantable Loop Recorder Services Core Five Startup Costs
Clinical Space and Procedure Room Setup Startup Expense
Procedure Room Cost
For an implant procedure room, start with the physical space, not the device. The hard CAPEX floor is $35,000 in medical office furniture plus $15,000 in sterilization equipment, before leasehold improvements, lighting, utilities, storage, and sterile handling flow. If you use an existing cardiology office, this is mostly fit-out; a leased office or ASC space needs more prep.
Price Inputs
Price the room by inputs: number of procedure chairs or tables, lighting, storage, work areas, and infection-control updates. Get vendor quotes for each item, then add any wall, power, or plumbing work needed for patient flow and sterile handling. One room with reused furniture costs very differently from a full leased buildout.
- Count room-specific fixtures.
- Quote buildout and install.
- Separate setup from rent.
Keep Costs Clean
Do not bury monthly space cost in CAPEX. If you use ASC access, the $15,000 per month fee belongs in pre-opening or working capital, along with deposits and early operating losses. That keeps the setup budget clean and stops you from overstating the procedure-room asset base.
- Keep rent off CAPEX.
- Track deposits separately.
- Fund launch losses upfront.
Best Launch Path
The lowest-complexity launch is usually an existing cardiology office with one dedicated procedure room, because patient flow, storage, and clinical utilities may already be in place. A leased office needs more leasehold work, while ASC access shifts cost into monthly cash burn. The budget question is setup cost, not total launch cash.
Device Inventory and Implantation Supplies Startup Expense
Starter Stock
This cost covers starter device stock plus sterile kits, drapes, local anesthetic, dressings, sharps disposal, and a reorder buffer. Use $120,000 for Month 1 initial inventory, then size the rest from case volume, vendor quotes, and lead time. Replenishment buys are operating inventory, not CAPEX.
Build the Order
Here’s the quick math: Year 1 assumptions include 120% implantable device procurement and 25% disposable surgical kits. Ask how many cases start in Month 1, who carries unused device risk, and whether stock is purchased or consigned. That tells you how much cash sits in shelves versus how much stays free for payroll.
- Match stock to first-month cases
- Confirm vendor payment terms
- Set reorder lead time
Keep Cash Lean
Use consignment or just-in-time supply if vendors allow it, because that cuts cash tied up in inventory without hurting care. Don’t overbuy for a small launch, and don’t treat refill orders as startup CAPEX. The clean rule is simple: stock for demand, not for pride.
Risk Buffer
The real swing factor is who owns the unused device risk. If the vendor keeps title until use, startup cash need drops; if not, you fund the shelf and the risk. Keep the opening $120,000 stock separate from later replenishment so working capital stays honest.
Monitoring Technology and Clinical Software Startup Expense
What it covers
This stack covers the diagnostic monitoring hub, remote patient portals, device interrogation and programming access, EMR integration, revenue cycle management setup, secure messaging, clinical laptops, and servers. The one-time build is $215,000 from $75,000 hub setup, $45,000 EMR work, $25,000 workstations, $40,000 servers, and $30,000 portal development.
Setup math
Estimate this from vendor quotes and scope by system: hub, EMR, portal, laptops, and servers. Here’s the quick math: $75,000 + $45,000 + $25,000 + $40,000 + $30,000 = $215,000 in CAPEX. Keep remote monitoring data fees out of setup and treat them as operating cost.
Monthly load
Recurring cost is $3,200 a month for the HIPAA-compliant software license plus $2,800 for IT security and support, or $6,000 monthly before data fees. Add the 10% remote monitoring data fee on monitored volume, and budget it as variable cost, not startup build.
Keep it lean
Cut waste by buying only the integrations you need at launch and delaying custom workflow work until case volume proves out. One clean rule: separate setup, subscriptions, and usage fees in the model. That makes margin easier to track, and it avoids mixing one-time build with monthly burn.
Licensing, Credentialing, Payer, Compliance, and Insurance Startup Expense
Pre-open costs
Licensing, credentialing, payer setup, and compliance are pre-opening professional costs, not CAPEX. Budget for entity setup, legal review, provider credentialing, payer enrollment, HIPAA rules, malpractice, general liability, cyber insurance, billing setup, and policies. Key recurring lines are $8,500 a month for malpractice insurance and $3,200 a month for HIPAA-compliant software.
Cost build
Build this from provider count, payer count, and months to approval. Add the 0.5 FTE compliance officer at $45,000 in Year 1 payroll, plus the monthly insurance and software run rate. This budget covers launch readiness, not rooms, devices, or imaging gear.
- Count each provider credentialed
- Price each payer application
- Model months until first cash
Control spend
Keep it tight by using one compliance calendar, standard policy templates, and early payer packet filing. Rework is expensive here; slow credentialing and weak billing setup can burn cash before claims pay. The goal is clean submission, not extra headcount.
- Submit payer files early
- Track license renewals monthly
- Standardize billing workflows
Working capital
Payer enrollment lag and claim denials raise working capital needs, but they do not change equipment cost. Cash still has to cover payroll, malpractice, software, and billing while collections catch up. Treat that gap as pre-opening runway, not as a procedure-room or device expense.
Staffing Readiness, Training, Launch Payroll, and Working Capital Startup Expense
Launch payroll
Year 1 staffing is modeled at $915,000, or about $76,250 per month. That covers 1 medical director at $280,000, 2 lead cardiac technicians at $95,000 each, 2 clinical liaisons at $85,000 each, 2 patient care coordinators at $60,000 each, 1 operations manager at $110,000, and a 0.5 compliance officer line at $45,000.
Cost build
Estimate this cost as headcount × salary plus training and onboarding time before collections start. At 2,065 modeled procedures per month, payroll is about $37 per procedure before devices, rent, or software. Use current salary quotes and make sure clinical, billing, and monitoring roles are staffed before launch.
Runway reserve
Keep payroll runway separate from equipment and buildout. This reserve should cover delayed payer setup, claim timing, and early ramp losses, not the procedure room or device stock. The common mistake is funding fixed payroll with capital dollars; that hides burn and leaves less cash when collections are still thin.
Cash timing
Before launch, the team needs cardiologist time, clinical support, monitoring staff, billing support, and training hours already paid for. That means the working capital plan should cover payroll first, while leasehold improvements, procedure-room setup, and device inventory stay in their own budget lines.
Lean, Base, and Full ILR Service Startup Cost Scenario Table
Launch cost scenarios
Lean, Base, and Full change startup cash need because space, device inventory, monitoring staff, and working capital scale fast in this service.
| Scenario | Lean LaunchLowest cash need | Base LaunchSource model | Full LaunchHighest build |
|---|---|---|---|
| Launch model | Physician-led launch that uses existing space, lean inventory, and limited monitoring staff. | This matches the source model with a full outpatient setup and standard staffing. | This version adds more provider capacity, stronger IT, larger inventory buffer, and dedicated monitoring staff. |
| Typical setup | Keep buildout light, reuse clinical rooms, and buy only core devices and software. | Use $385,000 CAPEX, $903,000 Month 1 minimum cash, $120,000 device inventory, $75,000 monitoring hub, and $39,000 fixed monthly expenses. | Expand staffing, add deeper monitoring coverage, and carry more working cash for a bigger rollout. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | Below base modelLeanest start | $903,000 minimum cashBase case | Above base modelUpper band |
| Best fit | Best for an existing cardiology practice that can start inside current space. | Best for an outpatient launch that wants the modeled setup and cash plan. | Best for a multi-provider monitoring operation that needs broader coverage and more cushion. |
Planning note: These scenario ranges are researched planning assumptions, not vendor quotes or exact quotes.
Related Products
- Implantable Loop Recorder Services Porter's Five Forces Analysis
- Implantable Loop Recorder Services BCG Matrix
- Implantable Loop Recorder Services Business Model Canvas
- What Are The 5 KPIs For Implantable Loop Recorder Services Business?
- Implantable Loop Recorder Services Business Plan Template in Pre-Written Word
- How Increase Profits For Implantable Loop Recorder Services?
- What Are Operating Costs For Implantable Loop Recorder Services?
- Implantable Loop Recorder Services Financial Model Template in Excel
- How Much Implantable Loop Recorder Service Owners Can Make: $159M
- Open an Implantable Loop Recorder Service in 3–6 Months
- How To Launch A Business Plan For Implantable Loop Recorder Services?
- Implantable Loop Recorder Services Marketing Mix
- Implantable Loop Recorder Services Marketing Plan
- Implantable Loop Recorder Services Business Proposal
- Implantable Loop Recorder Services PESTEL Analysis
- Implantable Loop Recorder Services Pitch Deck Example Editable PPTX
- Implantable Loop Recorder Services Business SWOT Analysis
- Implantable Loop Recorder Services Value Proposition Canvas
Frequently Asked Questions
The researched base case uses $385,000 of CAPEX That includes $120,000 for initial device inventory stock, $75,000 for diagnostic monitoring hub setup, and $45,000 for EMR integration and customization CAPEX does not include launch payroll, payer enrollment delay, malpractice insurance, monthly rent, replenishment inventory, or claim collection timing