 Time to Open6 monthsSetup window
Time to Open6 monthsSetup windowHow To Open An IV Ketamine Therapy Clinic In 4 To 9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6 monthsSetup window  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckLicense gateState rules
Key BottleneckLicense gateState rules First Revenue StepPaid inductionReferral consults
First Revenue StepPaid inductionReferral consults


You’re launching a medical clinic, not a wellness room, so the opening path starts with physician leadership, state medical rules, and controlled-substance workflows This guide covers 4 to 9 months of launch work, from entity setup and infusion-room readiness to staffing, referrals, and first-year model checks using 1 medical director, 2 infusion nurses, and 50% nurse capacity as planning assumptions Your next step is to validate compliance, staffing, and patient flow before signing fixed commitments
Time to Open6 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepPaid inductionReferral consultsKetamine clinic launch timeline
This short web summary shows the launch plan, and the XLSX export contains the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9
Compliance
- Form entity papers
- Map state rules
- DEA workflow set
- Malpractice review
Medical leadership
- Hire medical director
- Set clinical governance
- Define physician coverage
- Approve escalation tree
Facility buildout
- Finalize floor plan
- Start buildout work
- Soundproof treatment rooms
- Install safety fixtures
Equipment and vendors
- Order infusion pumps
- Source IV supplies
- Set drug storage
- Install EHR systems
- Set billing workflow
Staffing and training
- Recruit nurse team
- Confirm NP coverage
- Train infusion team
- Build screening scripts
- Complete consent training
Referrals and launch
- Build referral list
- Set website intake
- Start outreach calls
- Test patient flow
- Open soft launch
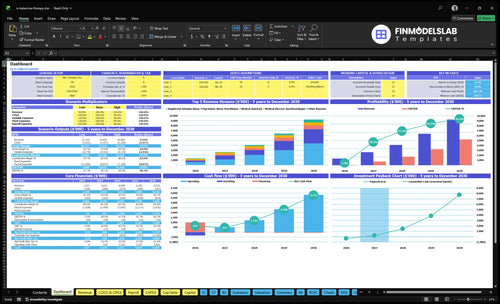
Why test launch numbers before you open?
It shows revenue, costs, cash needs, assumptions, and break-even logic. Open the IV Ketamine Therapy Clinic Financial Model Template.
Financial model highlights
- $179k monthly gross revenue
- 40% to 50% capacity
- 45% pharma, 30% supplies
- 100% marketing outreach
- Staffing and runway risk
What are the requirements to open a ketamine clinic?
To open an IV Ketamine Therapy Clinic, verify state medical rules first: physician ownership, corporate practice of medicine limits, prescribing authority, DEA registration, and state controlled-substance registration where required. Ketamine is a Schedule III controlled substance, so fix physician authority before you sign a lease, run ads, or hire staff; for startup cost planning, see How Much To Start An IV Ketamine Therapy Clinic Business?.
Compliance first
- Verify state medical ownership rules
- Set physician-led or compliant MSO structure
- Confirm medical director authority
- Secure malpractice and clinic policies
Launch order
- Complete legal review first
- Document consent, screening, and charts
- Build controlled-substance workflow
- Train emergency procedures before opening
How do you get patients for a ketamine clinic?
Get patients by building referral trust first, not by chasing broad ads. Start with education-first ties to psychiatrists, therapists, pain physicians, primary-care providers, and veterans’ mental health networks, and use a screened consult path that turns approved patients into paid treatment plans; for the KPI view, see What Are The 5 Core KPIs For IV Ketamine Therapy Clinic Business?
Referral trust
- Teach referral criteria upfront
- Review contraindications before consults
- Share compliant process content
- Build one-to-one provider relationships
Early volume
- Convert screened consults first
- Schedule induction series fast
- Use 80 psychiatric nurse practitioner treatments at $600
- Use 100 registered infusion nurse treatments at $500
How long does it take to open a ketamine clinic?
Opening an IV Ketamine Therapy Clinic usually takes 4 to 9 months. The early phase covers legal structure, physician leadership, malpractice, and controlled-substance workflow; the middle phase covers lease, infusion-room setup, EHR, payment workflow, medication sourcing, monitoring equipment, IV supplies, and emergency readiness. The late phase covers staff onboarding, protocol approval, referral outreach, screened consults, and soft launch, and the main delays come from state medical rules, DEA or state controlled-substance steps, facility readiness, malpractice underwriting, hiring qualified clinicians, and clinical protocol signoff.
Timeline by phase
- 4 to 9 months is the usual range
- Early phase sets the legal base
- Middle phase builds the clinic
- Late phase gets you to soft launch
Main delay points
- State medical rules can slow startup
- DEA or state steps add time
- Malpractice underwriting can stall opening
- Protocol signoff and hiring take time
Confirm the clinic is ready to open, not just planned
Launch readiness checklist
This is a go-live approval checklist to confirm the clinic is ready before opening.
Clinical rules
- Entity and medical director approvedCritical
Confirm the clinic's legal structure and medical director role before any patient care starts.
- DEA and prescribing authority clearedCritical
Controlled-substance rules and prescribing rights must be clear before ketamine is handled.
- Consent forms and charting reviewedHigh
Consent and documentation rules need to fit depression and pain treatment workflows.
- Malpractice coverage boundCritical
Coverage should be active before the first infusion or consult is booked.
Facility safety
- Private infusion rooms readyHigh
Private rooms support privacy, calm treatment, and safer patient observation.
- Monitoring and crash gear installedCritical
Vital signs monitors and emergency gear must work before the first infusion.
- Secure medication storage verifiedCritical
Secure storage is required for controlled substances and basic medication control.
- Accessibility and privacy passedHigh
Accessibility and privacy gaps can block patient flow and raise launch risk.
Medication supply
- Ketamine supplier contractedCritical
A confirmed source is needed so treatment starts are not delayed by stockouts.
- IV kits stocked for openingHigh
IV kits, tubing, and disposables need to cover the first operating month.
- Emergency meds and fluids stockedCritical
Backup meds and fluids matter because adverse events must be handled on site.
- Storage and waste logs readyHigh
Tracked storage and medical waste steps keep controlled handling auditable.
Staffing
- Medical director schedule lockedCritical
The anesthesiologist medical director must be available for oversight and escalation.
- NP, nurse, and assistant hiredCritical
Core clinical staffing must cover infusion, intake, prep, and room turnover.
- Psychologist consult coverage setHigh
Psychology support matters for depression care and patient screening decisions.
- Emergency drill and escalation runCritical
Staff need a practiced response for sedation events, monitoring alarms, and transfers.
Patient flow
- Referral outreach list builtHigh
Map psychiatrists, therapists, pain physicians, primary care, and veterans' mental health sources.
- Intake and scheduling testedCritical
Patients need a simple path from referral to consult to treatment slot.
- Payment and billing flow testedHigh
Billing must work on day one so first revenue is not stuck in admin work.
- First treatment slots publishedHigh
Published slots help convert referrals and support the 40% to 50% first-year ramp.
Cash signoff
- Month 12 cash floor coveredCritical
The model's $657k minimum cash at Month 12 needs funding before launch.
- Capex and opening spend approvedCritical
Buildout, equipment, and security spend must be signed off before orders go out.
- Monthly burn forecast reviewedHigh
Burn needs to fit the Month 2 breakeven path and the 21-month payback window.
- Go-live signoff completedCritical
Do not open until compliance, staffing, supply, and patient flow are all green.
What decides whether this clinic can open safely?
1Medical Legal
License gateYou can't safely sign the lease, hire, or market until physician authority and legal structure are set.
2Controlled Protocols
Drug protocolWritten controlled-substance protocols and training cut day-one medication risk and build referral trust.
3Facility Ready
Soft launchPrivate rooms, monitors, IV supplies, and secure storage keep patient flow from stalling at opening.
4Staff Coverage
6 rolesSigned coverage and credential files protect day-one scheduling and keep scope-of-practice gaps from delaying care.
5Referral Funnel
Live referralsA screened referral list turns opening rooms into booked consults and cleaner patient selection.
6Capacity Check
40%-50%Year 1 starts at 40%-50% capacity, so validate rooms, coverage, no-shows, and payment timing first.
Medical And Legal Authority
Medical and legal authority
You can’t safely sign a lease, hire staff, market, or book patients until state medical rules and physician authority are set. For an IV ketamine therapy clinic, the opening gate is the legal structure: who owns or manages the clinic, who serves as medical director, who can prescribe, and what supervision is required.
The readiness signal is simple: a documented ownership or management structure, a signed medical director agreement, confirmed prescribing authority, a malpractice binder, and legal review of corporate practice of medicine, scope of practice, chart review, referral acceptance, and advertising limits. If you assume a non-physician model works everywhere, you can lose weeks to rework and confuse payer, vendor, and referral talks.
Lock the structure before launch
Start with the state rules, then build the operating model around them. Do not lock in rent, staffing, or patient scheduling until counsel confirms who can own, manage, supervise, and prescribe in that state. That keeps your first-day plan realistic and avoids opening with a structure that can’t pass review.
Here’s the quick checklist: verify corporate practice rules, scope of practice, supervision, chart review, referral acceptance, and ad limits. Also get the physician paperwork, insurance binder, and management docs signed before you announce dates. That sequence cuts rework and makes payer and referral conversations cleaner.
- Confirm ownership rules first
- Sign medical director terms early
- Verify prescribing authority in writing
- Bind malpractice before scheduling
- Review ads before launch
1
Controlled-Substance And Clinical Protocols
Controlled-Substance Protocols
Ketamine is a Schedule III controlled substance, so the clinic cannot open cleanly without secure sourcing, storage, inventory logs, prescribing workflow, patient screening, consent, monitoring, and emergency escalation. If these pieces are not set before day one, launch slips and the first patients face avoidable safety and documentation gaps.
The readiness signal is simple: approved written protocols, staff training records, medication logs, consent forms, EHR templates, and emergency drill completion. Here’s the risk: loose documentation or unclear accountability can slow opening, trigger underwriting issues, and weaken referral trust before the first visit.
Lock Protocols Before Opening
Build the control stack first, then schedule patients. Tie each task to one owner, one deadline, and one sign-off, with physician leadership, pharmacy or supplier setup, DEA workflow, state rules, and malpractice review all checked before launch. That keeps the opening date realistic and avoids last-minute rework.
- Confirm secure medication storage
- Finish inventory log setup
- Train staff on escalation
- Test consent and EHR templates
- Complete emergency drills
2
Facility And Infusion-Room Readiness
Infusion-Room Flow
Facility readiness decides whether the clinic can open on time and treat the first patient without friction. If private infusion rooms, patient monitoring equipment, IV supplies, emergency equipment, secure medication storage, privacy controls, EHR access, and payment workflow are not in place, patient flow breaks before revenue starts.
The key dependency is final protocol design before equipment and layout decisions. Build around intake, treatment, observation, discharge, documentation, and room turnover, not interior style. If the room is designed first and the workflow later, the launch gets stuck in rework and the soft launch will likely have fewer schedule gaps.
Build the room around the workflow
Before opening, verify that each room can support the full visit path from check-in to discharge. The clinic should test the room as if a patient is already on site, with staff able to monitor, document, store meds, and collect payment without leaving the care area.
- Map intake, treatment, and discharge
- Check monitoring and emergency gear
- Confirm secure med storage
- Test EHR and payment access
- Time room turnover before launch
Assign one owner for room turnover, one for documentation, and one for supply checks. Then run a mock day and fix any delay that slows observation or blocks the next patient. That keeps the first schedule realistic and protects day-one capacity.
3
Qualified Staffing And Coverage
Qualified staffing and coverage
Coverage rules vary by state, so this clinic cannot open safely until the right licensed roles are signed and mapped. The first-year staffing assumption is 1 anesthesiologist medical director, 1 psychiatric nurse practitioner, 2 registered infusion nurses, 1 clinical psychologist, and 1 medical assistant. If these roles are not credentialed and scheduled, day-one capacity gets shaky fast.
The real readiness signal is a signed coverage schedule plus credential files, emergency training, infusion competency, intake workflow, documentation training, and backup coverage. This is where many launches slip: if hiring starts after marketing, patient slots fill before staffing does. The result is delayed openings, weaker scheduling, and more no-shows in care delivery.
Lock roles before patient scheduling
Map each job before opening: physician oversight, APRN or PA where allowed, RN infusion coverage, behavioral health, medical assistant support, billing, and admin. One clean rule: no marketing until every shift has named coverage. That keeps the launch tied to real capacity, not hopeful headcount.
- Verify state scope of practice first.
- File credentials before first booking.
- Train on emergency response and documentation.
- Assign backup coverage for absences.
Without this, the clinic may have a room, equipment, and demand, but still miss openings because the schedule is not legally or operationally covered.
4
Referral And Patient-Screening Funnel
Referral Funnel Ready
No screened consults means no day one revenue. For an IV ketamine therapy clinic, first patients usually come from trusted clinical referral channels, not walk-in demand, so the launch lives or dies on a live referral list, screening criteria, contraindication review, and a consult path that actually converts.
If the clinic opens with rooms ready but no approved referrals, capacity sits idle and the first revenue slips. Keep the process tight: education materials, treatment-plan approval, and induction-series scheduling have to work before the doors open, or the business looks open while the calendar stays empty.
Build the Referral Path First
Lock the sequence before launch: referral education, screening, contraindication review, consult workflow, approval, then scheduling. One owner should track every referred patient from first contact to booked induction, so people do not stall between clinical review and calendar placement.
Keep outreach educational and compliant, with no cure claims. Focus on psychiatrists, therapists, pain physicians, primary-care providers, and veterans’ mental health networks, and verify the referral list is live, named, and current before opening.
- Live referral list with named contacts
- Screening criteria and contraindications
- Consult approval workflow in writing
- Induction scheduling ownership assigned
- Compliant education only, no cure claims
5
Financial Model And Capacity Validation
Capacity and cash reality check
This driver decides whether the clinic can open on time and actually fill the schedule on day one. The model only works if room count, treatment length, provider coverage, and nurse capacity support the planned mix: 40 medical director treatments at $1,200, 80 psychiatric nurse practitioner treatments at $600, 100 registered nurse treatments at $500, 60 clinical psychologist sessions at $250, and 120 medical assistant-supported visits at $150.
That mix totals about $179,000 in modeled monthly gross revenue capacity, but Year 1 is only 40% to 50% of that load. If no-shows, slow collections, or long room turns cut throughput, the clinic can open with rooms ready and still miss cash needs. The real risk is overbuilding before referral demand is proven.
Validate the schedule before you buy the buildout
Build the opening plan backward from the service mix, not from the lease. Confirm room count, treatment length, observation time, and staff coverage against the monthly cap. Then test what happens at 40%, 50%, and a no-show case so the first schedule is realistic, not optimistic.
- Map each visit to one room.
- Assign registered nurse and clinician coverage.
- Model payment timing into cash runway.
- Load pharmaceuticals at 45% of cost.
- Load disposable supplies at 30% of cost.
- Treat outreach as 100% cash out.
Before opening, document the breakeven path, the refill cadence, and the minimum referral volume needed to keep the calendar full. If the staffing grid cannot support the modeled mix without overtime or gaps, delay launch rather than absorb avoidable burn in month one.
6
Related Products
- IV Ketamine Therapy Clinic Porter's Five Forces Analysis
- IV Ketamine Therapy Clinic BCG Matrix
- IV Ketamine Therapy Clinic Business Model Canvas
- What Are The 5 Core KPIs For IV Ketamine Therapy Clinic Business?
- IV Ketamine Therapy Clinic Business Plan Template in Pre-Written Word
- How Increase Profits For IV Ketamine Therapy Clinic?
- What Are IV Ketamine Therapy Clinic Operating Costs?
- IV Ketamine Therapy Clinic Startup Costs With $93k Monthly Fixed Burn
- IV Ketamine Therapy Clinic Financial Model Template in Excel
- IV Ketamine Therapy Clinic Owner Income: $215M Revenue Model
- How To Write A Business Plan For IV Ketamine Therapy Clinic?
- IV Ketamine Therapy Clinic Marketing Mix
- IV Ketamine Therapy Clinic Marketing Plan
- IV Ketamine Therapy Clinic Business Proposal
- IV Ketamine Therapy Clinic PESTEL Analysis
- IV Ketamine Therapy Pitch Deck Example Editable PPTX
- IV Ketamine Therapy Clinic Business SWOT Analysis
- IV Ketamine Therapy Clinic Value Proposition Canvas
Frequently Asked Questions
Start with state medical rules and physician authority You’ll need the right ownership or management structure, medical director coverage, prescribing authority, controlled-substance procedures, malpractice coverage, clinical policies, and documentation workflows Plan for a 4 to 9 month launch path before treating patients