 Owner income$337k to $6.6m
Owner income$337k to $6.6mHow Much Does a Laser Eye Surgery Center Owner Make at 44 Cases/Month?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$337k to $6.6m  Net margin257% to 639%
Net margin257% to 639% Revenue for target pay$157k/mo
Revenue for target pay$157k/mo Business difficultyHard
Business difficultyHard



Key Takeaways
- Procedure volume is the main break-even lever.
- Higher case prices lift revenue only if volume holds.
- Surgeon pay can outweigh small savings elsewhere.
- Staffing must match safe throughput, not budget alone.
Owner income$337k to $6.6mNet margin257% to 639%Revenue for target pay$157k/moBusiness difficultyHardWant to test your own owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not a guaranteed salary, tax advice, or owner distribution advice.
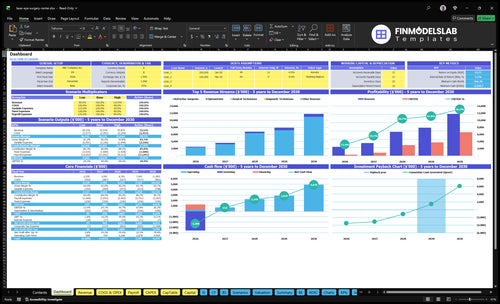
How do you check owner income in the full financial model?
This dashboard shows revenue, margin, costs, reserves, and owner take-home; open the Laser Eye Surgery Center Financial Model Template to see the full model.
Owner-income model highlights
- Year 1 owner output
- Revenue and profit compare
- Scenario tests assumptions
What laser eye surgery center operating costs reduce owner take-home?
In a Laser Eye Surgery Center, owner take-home gets squeezed most by fixed overhead and payroll, not just procedure costs; for the startup side, see How Much Does It Cost To Open And Launch Your Laser Eye Surgery Center?. The modeled monthly overhead is $29,000, including $15,000 rent, $4,000 malpractice insurance, $2,500 utilities, and $2,000 software. Year 1 COGS is 50% technology usage fees and royalties plus 30% disposable medical supplies, while variable selling costs add 60% marketing and patient acquisition plus 20% payment processing; equipment financing and service contracts should sit in separate cash flow inputs.
Fixed cost drags
- $29,000 monthly fixed overhead
- $15,000 rent
- $4,000 malpractice insurance
- $2,500 utilities and $2,000 software
Variable cost drags
- 50% technology usage fees and royalties
- 30% disposable medical supplies
- 60% marketing and patient acquisition
- 20% payment processing
How many procedures does a laser eye surgery center need to be profitable?
For a Laser Eye Surgery Center, break-even is about 32 procedures per month on surgery alone, or about 30 per month with $12,000 in modeled optometry revenue. The pressure comes from $93,333 in monthly payroll plus $29,000 in fixed overhead, while each $4,500 procedure carries an 84% contribution after COGS, marketing, and processing. If owner pay rises, each extra $100,000 of annual target pay needs about 22 more monthly procedures.
Cost base
- $93,333 monthly payroll
- $29,000 fixed overhead
- 84% contribution rate
- $4,500 procedure price
Volume math
- 32 monthly procedures break even
- 30 with $12,000 optometry revenue
- 22 more procedures per $100,000
- Owner pay changes the floor fast
How much can a LASIK center owner make?
A Laser Eye Surgery Center owner can model about $648,800 in Year 1 income capacity before tax, debt service, and reserves; the same model shows about $362 million in Year 3 and $755 million in Year 5, so this is scenario math, not a universal paycheck. The main swing factors are 44 to 187 monthly refractive procedures, price per procedure, surgeon payroll, marketing efficiency, and owner role; track the core driver here: What Is The Most Important Metric To Measure The Success Of Your Laser Eye Surgery Center?
Modeled owner income
- Year 1: $648,800 before major deductions
- Year 3: $362 million modeled output
- Year 5: $755 million modeled output
- Volume range: 44 to 187 procedures/month
What changes payout
- Raise price per refractive procedure
- Control surgeon payroll and staffing
- Improve marketing cost per patient
- Separate surgeon-owner pay from distributions
Want the six owner income drivers?
1
44→187/moProcedure Volume
Booked procedures rise from 44 per month in Year 1 to 187 in Year 5, so every extra case lifts revenue and spreads fixed costs.
2
$4.5K-$4.9KProcedure Price
Prices move from $4,500 to $4,900, and even small gains per case add up fast at higher volume.
3
$750K-$1.35MSurgeon Pay
Surgeon payroll scales as FTEs rise, so staffing choice changes owner take-home directly.
4
$29K/moOverhead Load
Fixed overhead runs about $29,000 a month, so rent, insurance, and admin costs eat margin fast when volume slips.
5
6%-4%Marketing Pull
Patient acquisition cost falls from 6% to 4% of sales, and better referral flow keeps more revenue in the clinic.
6
50%-85%Utilization
Capacity moves from 50% to 85% on core staff, so better clinic flow turns the same headcount into more income.
Laser Eye Surgery Center Core Six Income Drivers
Procedure Volume And Conversion
Procedure Volume and Conversion
This driver is the count of completed refractive procedures, not just consults. At 44 procedures per month in Year 1 and 187 in Year 5, volume is the main way the center spreads fixed payroll and rent over more revenue, so owner pay rises fastest when booked patients actually reach surgery day.
Here’s the quick math: under Year 1 assumptions, break-even is about 30 to 32 procedures per month. Missed consult conversion hurts twice because marketing spend is wasted and paid clinical capacity sits unused, which cuts cash flow and leaves less profit for owner draw.
Track the Full Surgery Funnel
Measure the path from consults to eligibility to booked surgery to completed cases. The goal is simple: fill surgery days with enough approved patients so the center keeps fixed costs covered and the owner can take home more profit.
- Track consults booked each month
- Track eligibility rate after consult
- Track booked surgeries vs consults
- Track cancellations before surgery day
- Track completed cases per surgery day
If completed volume stays below 30 to 32 cases a month, profit gets tight fast. Tight follow-up, lower cancellations, and enough surgery-day slots matter more than small cost cuts, because unused clinical time still costs money.
1
Average Procedure Price And Service Mix
Procedure Price and Mix
Average procedure price is the amount collected per completed refractive case after discounts and patient financing terms. The model uses $4,500 per procedure in Year 1 and $4,900 by Year 5, an 8.9% lift. If volume holds, that change flows straight into revenue and owner draw, but only if realized price stays close to plan.
Optometry revenue adds $12,000 per month in Year 1 and $67,320 per month in Year 5. Bilateral mix, premium positioning, and discounting can move revenue per completed case fast, so pricing is a sensitivity, not a market promise. The quick check is simple: higher realized price usually means more cash for the owner, if costs do not rise with it.
Track Realized Price and Mix
Measure realized price per case, not list price. Track completed cases, discount rate, bilateral vs. single-eye mix, financing approval rate, and optometry revenue separately. If realized price slips, profit and owner pay fall even when procedure count holds. One clean rule: watch the gap between quoted price and cash collected.
- Log price by procedure type.
- Separate cash and financed cases.
- Review discounting weekly.
- Model optometry revenue monthly.
2
Owner Role And Surgeon Compensation
Owner Pay vs Surgeon Payroll
Here, the big swing is who earns the clinical fee. The model uses a $450,000 lead surgeon salary and a $300,000 associate surgeon salary, with 2 refractive surgeons in Year 1 and 4 in Year 5. If the owner is also the surgeon, part of that pay may come back as clinical income; if the owner is an investor, those salaries hit profit before any owner distribution.
That makes surgeon comp a bigger income lever than small supply savings. One extra surgeon on payroll can move cash flow more than trimming minor disposables, because the pay is large and fixed. Medical director cost, supervision, and state ownership rules should be modeled separately from owner draw, since they can change what stays in the business and what gets paid out.
Track Clinical Pay by Role
Build the owner model around role, not just headcount. Track lead surgeon salary, associate salary, medical director fees, and whether the owner performs cases. Then forecast owner income as clinical pay plus profit distributions, not one blended number. If the owner covers more cases, take-home can rise without changing procedure volume.
Use a simple staffing check: 2 surgeons in Year 1, 4 in Year 5, and each added surgeon should be justified by booked cases, not optimism. If supervision or ownership rules differ by state, price those costs before you set owner draw. That keeps reported profit and actual cash available to the owner from getting mixed up.
- Track surgeon pay by role
- Separate owner draw from wages
- Model medical director fees separately
- Test profit after each surgeon hire
3
Laser Equipment And Facility Overhead
Laser & Facility Overhead
This center carries $29,000 per month of fixed overhead before owner pay. $15,000 rent is about 52% of that base, with $4,000 malpractice insurance and $2,000 IT and software adding more fixed drag. That’s $348,000 a year that has to be covered before distributions, so weak volume quickly cuts the owner’s take-home.
The model does not break out separate equipment leases, maintenance, calibration, software fees, or depreciation, so those should be added as scenario inputs if financing is used. If equipment debt is added, it sits after operating profit and before owner distributions, which means the owner only gets paid after the clinic clears all operating costs and financing.
Track the Fixed Burn
Measure overhead as a monthly burn rate and compare it to procedure margin. Here’s the quick math: every $1,000 increase in fixed overhead adds $12,000 per year to the profit hurdle before owner pay moves at all.
- Equipment lease payment
- Maintenance and calibration
- Software and support fees
- Depreciation or financing cost
- Insurance and rent renewals
Keep each item under contract and review it before renewal. If the clinic is paying for financed equipment, track the debt service separately from rent and payroll so cash flow, not just accounting profit, decides how much the owner can safely draw.
4
Marketing Efficiency And Referral Flow
Marketing Efficiency And Referral Flow
Patient acquisition cost is the margin test. The model puts marketing and patient acquisition at 60% of revenue in Year 1, easing to 40% by Year 5. Track cost per booked consult, consult-to-surgery conversion, and cancellations, because weak leads burn cash before they ever reach the procedure room. One bad funnel can cut owner draw fast.
Referral flow matters because it fills consult slots without discounting. More referrals mean more completed cases from the same clinic capacity, so fixed costs get spread across more revenue. That pushes more cash into take-home income and less into paid ads. More booked consults, less price pressure is the cleanest path here.
Measure Booked Consults First
Build the forecast from the top of the funnel. Measure consults booked, show rate, consult-to-surgery conversion, and cancellation rate, then compare spend to contribution per completed procedure . If referral leads book better, shift budget there. If paid leads do not convert, cut them fast. The goal is more completed cases, not more clicks.
- Cost per booked consult
- Consult-to-surgery conversion
- Cancellations
- Contribution per completed case
When referrals keep the calendar full, the owner keeps price intact and protects margin. If consult slots sit open, every extra lead has to work harder just to cover the same overhead, and owner pay drops after COGS and processing.
5
Staffing Utilization And Clinical Throughput
Staffing for Safe Throughput
Staffing is not a fixed budget line here; it has to match how many exams, surgery days, follow-ups, compliance checks, and patient touchpoints the clinic can safely handle. In this model, payroll is $112 million in Year 1 and $234 million in Year 5, while refractive surgeon and surgical technician capacity rises from 55% to 85%. Too few staff cuts volume, and too many staff crushes margin.
Here’s the quick math: payroll only helps owner income when each staffed hour supports more completed cases. Track completed procedures, consult-to-surgery conversion, cancellations, overtime, and idle time by role. If staffing runs ahead of demand, cash gets tied up in labor before it reaches profit or owner draw.
Measure Cases per Staffed Day
Use booked consults, eligible patients, surgery-day slots, follow-up load, and management coverage to set schedules. The goal is not to keep headcount low; it is to keep the right people busy enough to protect safety and patient experience. If exams or post-op visits stack up, throughput slips before the payroll line does.
Watch cases per staffed day and payroll as a share of revenue each week. When cancellations rise or referral flow drops, cut back variable shifts before service quality falls. When volume holds and staff utilization moves toward 85%, the clinic can support more profit and more owner pay.
6
Compare low, base, and high laser eye surgery center income scenarios
Owner income scenarios
Owner income moves with volume, staffing, and fixed overhead. These scenarios show how Year 1, Year 3, and Year 5 assumptions change modeled cash before taxes, debt service, and reserves.
| Scenario | Low CaseDownside case | Base CaseBase case | High CaseUpside case |
|---|---|---|---|
| Launch model | Lower modeled earnings path using Year 1 volume and staff levels. | Modeled middle path using Year 3 volume and staffing assumptions. | Stronger modeled earnings path using Year 5 volume and staffing assumptions. |
| Typical setup | About 40 refractive procedures and 100 exam visits a month, with 2 surgeons, 1 optometrist, lean support staff, and $28,000 in fixed overhead. | About 50 refractive procedures and 110 exam visits a month, with 3 surgeons, 2 optometrists, and a larger support team. | About 55 refractive procedures and 120 exam visits a month, with 4 surgeons, 3 optometrists, and the fullest staff buildout in the model. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $337kYear 1 income | $3.0MYear 3 income | $6.6MYear 5 income |
| Best fit | Fits a slow start, weaker conversion, or a launch period with tighter demand. | Fits a steady clinic that reaches the model's midcycle operating level. | Fits a clinic that runs near planned capacity and keeps demand strong. |
Planning note: Scenario figures are researched planning assumptions only. They are not guaranteed earnings, salary promises, tax advice, or distribution forecasts.
Related Products
- Laser Eye Surgery Center Porter's Five Forces Analysis
- Laser Eye Surgery Center BCG Matrix
- Laser Eye Surgery Center Business Model Canvas
- 7 Critical KPIs to Measure Laser Eye Surgery Center Success
- Laser Eye Surgery Center Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Laser Eye Surgery Center Profitability
- How Much Does It Cost To Operate a Laser Eye Surgery Center Monthly?
- Laser Eye Surgery Center Startup Costs for a 2-Surgeon Launch
- Laser Eye Surgery Center Financial Model Template in Excel
- How to Open a Laser Eye Surgery Center in 9 to 18 Months
- How to Write a Business Plan for a Laser Eye Surgery Center
- Laser Eye Surgery Center Marketing Mix
- Laser Eye Surgery Center Marketing Plan
- Laser Eye Surgery Center Business Proposal
- Laser Eye Surgery Center PESTEL Analysis
- Laser Eye Surgery Center Pitch Deck Example Editable PPTX
- Laser Eye Surgery Center Business SWOT Analysis
- Laser Eye Surgery Center Value Proposition Canvas
Frequently Asked Questions
In this model, it is profitable in Year 1 after operating costs Monthly revenue is $210,000, monthly payroll plus fixed overhead is about $122,333, and revenue-linked costs are 160% That leaves about $54,100 in monthly operating profit, assuming 44 refractive procedures and 60 optometry visits per month