 Time to Open6-12 monthsOpening prep
Time to Open6-12 monthsOpening prepHow To Open A Medical Clinic: 6–12 Month Launch Plan

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6-12 monthsOpening prep  Launch Sequence6 stagesLicensing first
Launch Sequence6 stagesLicensing first Key BottleneckCredentialing lagProvider lead time
Key BottleneckCredentialing lagProvider lead time First Revenue StepBilled visitsCode and collect
First Revenue StepBilled visitsCode and collect


To open a medical clinic, define your service scope, form the legal entity, verify state requirements, lease and prepare clinical space, hire providers and staff, set up Electronic Health Record (EHR) and billing systems, complete payer enrollment, and book the first patient visits A common planning range is 6–12 months, with delays tied to state rules, lease buildout, payer credentialing, and provider hiring In the researched planning assumptions, Year 1 monthly revenue capacity is about $75,790 at modeled utilization, before supplies, lab fees, billing fees, marketing, fixed overhead, and payroll First revenue starts only when visits are scheduled, documented, coded, billed, and collectible
Time to Open6-12 monthsOpening prepLaunch Sequence6 stagesLicensing firstKey BottleneckCredentialing lagProvider lead timeFirst Revenue StepBilled visitsCode and collectLaunch Timeline
This is a short web summary of the clinic launch plan, and the XLSX export contains the detailed Gantt chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Legal / compliance
- State filing package
- Ownership review
- Malpractice coverage
- HIPAA policies
- OSHA readiness
Facility / equipment
- Lease sign
- Buildout permits
- Exam room setup
- IT wiring
- Equipment install
Staffing
- Physician recruiting
- Nurse hiring
- Assistant hiring
- Admin training
- Provider onboarding
Technology
- EHR setup
- Hardware install
- Scheduling launch
- Billing rules
- Claim testing
Payer enrollment
- Payer list
- Credential applications
- Directory checks
- Contract follow-up
- Go-live approval
Marketing
- Clinic profile
- Referral outreach
- Website listing
- Soft launch
- First bookings
Why test a Medical Clinic launch before you open?
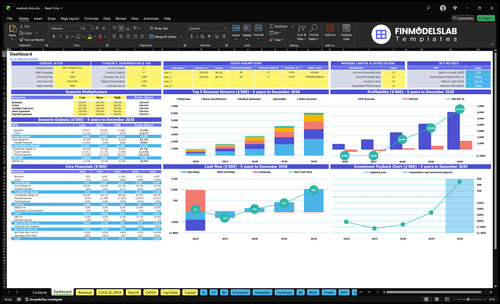
The Medical Clinic Financial Model Template screenshot shows revenue, costs, cash needs, assumptions, and break-even logic—open the model.
Financial model highlights
- Year 1 staffing plan
- About $75.8k monthly revenue
- $19.6k overhead, $47.5k payroll
- 50% to 85% ramp
What do you need to open a medical clinic?
To open a Medical Clinic, start with scope of services, then clear state, facility, payer, and safety rules before seeing patients; primary care, phlebotomy, prescribing, and lab testing can each add a different approval path. This is an operating checklist, not legal advice, and What Is The Main Indicator Of Success For Your Medical Clinic? should sit beside it because access, capacity, and compliance drive the same launch plan.
Legal setup
- Verify state clinic license and entity rules
- Check physician ownership and practice limits
- Name a medical director if required
- Confirm licenses and malpractice insurance
Open-ready proof
- Set HIPAA policies under 45 CFR 164
- Follow OSHA blood rules: 29 CFR 1910.1030
- Choose CLIA status for 3 lab levels
- Secure zoning, permits, inspections, and payer path
What mistakes delay a medical clinic launch?
The biggest launch mistake is opening before the operating pieces are ready: payer credentialing, lease use, billing, staffing, HIPAA, OSHA, and the appointment pipeline. For a Medical Clinic, the burn is fast: $19,600 in monthly fixed overhead plus at least $47,500 in payroll means $67,100 a month before variable costs, so delays drain cash quickly. If claims are unsubmitted and schedules are empty on day one, the clinic starts behind and keeps slipping.
Launch risks
- Start payer applications early.
- Confirm clinical use before signing.
- Test billing workflows before opening.
- Build the referral pipeline first.
Readiness gaps
- Unsubmitted claims slow cash.
- Untrained staff slows intake.
- Missing HIPAA steps raise risk.
- Empty schedules waste opening week.
How do you get patients for a new medical clinic?
Get patients by making the Medical Clinic easy to find, easy to book, and aligned with payer contracts and capacity. For a cost context, see How Much Does It Cost To Open And Launch Your Medical Clinic Business? First-year planning assumes 160 treatments per physician, 180 per nurse practitioner, 200 per medical assistant, 120 per specialist, and 300 per phlebotomist before utilization, with 60%, 65%, 70%, 50%, and 75% utilization by role. Since marketing is modeled at 3% of revenue in Year 1, wasted leads hit cash fast.
Build local demand
- Show up in local search.
- Complete Google Business Profile.
- List in insurance directories.
- Book visits before opening.
Match capacity
- Use referral relationships.
- Reach local employers.
- Run community awareness.
- Keep billing workflow ready.
Confirm whether the clinic is ready to open safely and bill cleanly
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Compliance
- Entity registration filedCritical
Needed before permits, banking, and contracts can move.
- State clinic permits approvedCritical
Clinic work should not start until state rules are cleared.
- Medical director assignedHigh
Many clinics need medical oversight before opening.
- Malpractice policy boundCritical
The model carries $3,000 monthly; bind it before patient care.
Facility
- Lease executed and usableCritical
You need a usable site before buildout and inspections.
- Exam rooms fully outfittedHigh
Rooms must support visits, vitals, and basic procedures.
- OSHA and HIPAA procedures postedCritical
Staff need clear safety and privacy rules on day one.
- Security and cleaning activeHigh
The model includes $600 security and $800 cleaning each month.
Systems
- EHR configured and testedCritical
Charting and orders must work before first patient check-in.
- Billing vendor can submit claimsCritical
Cash is late if claims cannot be sent on time.
- Lab and supply vendors setHigh
Tests and routine care need stable supply and lab support.
- CLIA status confirmed if testingMedium
If testing is offered, lab status must match the service.
Staffing
- Providers credentialed with payersCritical
Uncredentialed providers can block reimbursement and launch.
- Staff schedules cover openingsHigh
Coverage must match visit volume from the first month.
- Intake and triage trainedHigh
Front-desk and clinical intake must run without gaps.
- Referral and handoff paths setMedium
Patients need a clean path to specialists and follow-up.
Patient flow
- Booking and phone workflows liveCritical
Patients need a working way to book, ask, and confirm.
- Appointment templates match capacityHigh
Slots should fit the Year 1 staffing and visit ramp.
- Patient intake to billing worksCritical
If intake breaks, the bill-to-cash flow breaks too.
- First payer claims acceptedCritical
Revenue starts only when the payer actually accepts claims.
Cash
- Opening cash covers runwayCritical
Cash must reach the Month 25 low point in the model.
- Payroll and overhead fundedCritical
Rent, salaries, and software need cash before revenue catches.
- Monthly revenue target reviewedHigh
Use the $75,790 model and 15% variable load in the test.
- Go-live signoff completedCritical
Open only after every prior gate is ready.
Want the six launch drivers in one view?
1Compliance Ready
6-12 moState registration, malpractice, and privacy rules are the go/no-go gate for opening.
2Facility Setup
$19.6KBuildout, equipment, and inspections decide opening date, and space gaps trigger reschedules.
3Provider Staffing
Year 1 mixYear 1 needs 2 physicians, 1 nurse practitioner, 2 medical assistants, 1 specialist, and 1 phlebotomist.
4Payer Billing
15% loadBilling and collections are a 15% load, so weak claim setup slows cash.
5EHR Workflows
$3.2K/moEHR and IT need to be live before booking starts, or claim errors rise.
6Patient Pipeline
$75.8K/moLocal search and referrals fill the first month, matching 50% to 75% role utilization.
Regulatory And Compliance Readiness
Compliance Readiness
Regulatory and compliance readiness is a go/no-go item for a medical clinic. If state registration, medical board rules, ownership structure, malpractice coverage, privacy policies, OSHA procedures, controlled substance rules, or CLIA status are not set, you may not be allowed to offer the service line on opening day.
The launch risk rises fast when you add lab testing, prescribing, or multi-state providers. The ready signal is simple: documented policies, active coverage, approved registrations, trained staff, and a verified scope. That setup cuts inspection issues, cleans up payer applications, and lowers opening-week disruption.
- Confirm service lines first.
- Match scope to licenses.
- Verify medical director need.
- Track payer enrollment timing.
- Prepare for facility inspections.
Lock the Go/No-Go Items
Before you open, build a checklist for registration, insurance, privacy, OSHA, controlled substances, and CLIA. If one item is missing, pause the launch plan instead of pushing visits into a gray area. The clinic should only schedule services that fit the approved scope and staffed coverage.
Assign one owner to each dependency: licensing, medical director, payer enrollment, and inspection prep. Then test the day-one workflow with the exact services you plan to offer. If a policy is not written, a file is not signed, or staff are not trained, treat it as a launch blocker, not a later fix.
1
Facility And Clinical Setup
Clinical Space Ready
Facility setup is a go/no-go for opening on time. The clinic needs a suitable lease, completed buildout, exam rooms, reception, accessibility checks under the Americans with Disabilities Act (ADA) where applicable, medical equipment, supplies, infection control, IT wiring, signage, cleaning, security, and inspections before first patients can walk in safely.
Here’s the quick math: base site costs already run about $12,900/month, made up of $10,000 rent, $1,500 utilities, $800 cleaning, and $600 security. The bottleneck risk is signing a space that needs more clinical work than planned, which can push the opening date and force early reschedules.
Map Patient Flow First
Walk the space before you commit. Check where EHR hardware sits, how lab workflow runs, where supplies and sharps disposal go, and whether staff can move through rooms without crossing paths or backing up the front desk. That flow affects day-one safety and how fast the clinic can see patients.
Use a pre-open checklist and test it before launch: IT wiring live, signage up, cleaning scheduled, security in place, and inspections lined up. If any of those slip, first-week operations turn manual fast, and the clinic starts with slower visits and more reschedules.
- Confirm exam-room count and layout.
- Verify ADA access where applicable.
- Place EHR, supplies, and sharps storage.
- Test staff movement from check-in to exit.
- Schedule cleaning and inspection dates early.
2
Provider And Staff Recruitment
Provider And Staff Recruitment
Without signed coverage for clinicians and support staff, the clinic cannot open with enough appointment slots, clean billing flow, or a steady front desk. The Year 1 plan calls for 2 physicians, 1 nurse practitioner, 2 medical assistants, 1 specialist, 1 phlebotomist, plus 1 clinic manager, 1 receptionist, and 1 medical biller. The disclosed salary base is at least $570,000 before adding the nurse practitioner and other clinical roles.
The launch risk is simple: if hiring starts after payer applications or opening marketing, the clinic can look open but still miss calls, underfill schedules, and delay revenue ramp. Signed coverage before scheduling opens is the readiness signal. That protects day-one patient experience and gives enough staffing depth to handle check-in, rooming, billing, and leadership coverage without scrambling.
Verify Coverage Before Booking
Build the staffing plan in the same order as opening tasks. Lock the providers first, then the medical assistants, front desk, billing, and clinic leader. Tie each role to a start date, training plan, and backup coverage. If one role is late, the whole schedule can slip because a clinic needs more than exam rooms; it needs people who can run intake, documentation, and claims from day one.
Use a simple launch checklist:
- Signed offers for all core roles
- Credential and license checks complete
- Front desk coverage for open hours
- Billing support ready before first visit
- Manager set to handle call volume
That sequencing helps prevent missed calls, thin schedules, and a weak first month.
3
Payer Enrollment And Billing Readiness
Payer Enrollment Ready
For a medical clinic, this driver is the gate between seeing insured patients and getting paid for them. If the NPI is set up where required, payer applications are submitted, and contracts are tracked, you can start collecting revenue sooner after the first billable visits. Without that, the clinic may be open but still stuck with unpaid claims.
The setup also has to include billing software, coding workflows, claim submission testing, denials handling, and payment posting. Year 1 billing and collections fees are modeled at 4% of revenue, plus external lab fees at 3%, so clean claim flow matters from day one. If visits cannot be billed cleanly, cash conversion slows even when schedules are full.
Load Claims Before Opening
Start with the inputs that payers and billing need: provider licenses, entity data, malpractice coverage, bank details, service scope, and EHR integration. Then verify the chain in order: enroll, track contracts, configure the billing system, train coding, test claim submission, assign denials work, and confirm payment posting. One broken step can delay first cash.
- Confirm NPI setup where required.
- Submit payer applications early.
- Test at least one claim path.
- Assign one denials owner.
- Document payment posting steps.
Keep this tight before opening. If payer setup slips past the first visit date, the clinic may need manual follow-up, delayed collection, and extra staff time to fix claims after the fact. That creates opening-week cash strain and distracts the front desk from patient flow.
4
EHR And Operating Workflows
EHR And Workflow Setup
The clinic can’t open cleanly if staff still have to jump between paper, spreadsheets, and the system. The launch point is a single flow from booking to documentation to billing, with EHR software at $2,000 per month plus IT support at $1,200 per month. If that flow is broken, check-in slows, claims get messy, and day-one volume turns into manual chaos.
Readiness means the patient portal is live, online scheduling works, intake forms are loaded, templates are built, and billing data moves into the chart correctly. The main risk is fixing workflow gaps after launch, when front desk scripts, medical assistant steps, and provider preferences are already in motion.
Test The Full Patient Path
Before opening, run one full test from appointment request to final charge. That means payer setup is in place, provider rules are set, the front desk script is written, and medical assistants know their steps. If e-prescribing applies, confirm it works. If lab or referral work is part of the visit, check those links too.
- Load intake and consent forms.
- Test billing integration end-to-end.
- Confirm chart templates by provider.
- Train staff on check-in screens.
- Fix errors before first patient day.
Here’s the quick math: the clinic is carrying $3,200 per month just for EHR and IT support, so the system has to work on day one. Clean testing usually means fewer claim errors and a shorter check-in time.
5
Patient Acquisition And Referral Pipeline
Patient Demand Setup
For a medical clinic, this driver decides whether day one starts with booked visits or empty chairs. The goal is to fill the first operating month with patients who match capacity and payer readiness, so the clinic can bill sooner and avoid delay from broad branding with no schedule. Year 1 patient acquisition spend is modeled at 3% of revenue, so early marketing has to create visits, not just awareness.
Timing matters because Year 1 utilization ranges from 50% for specialists to 75% for phlebotomists. That means demand-building must be role-specific, with enough bookings for each service line before opening. Here’s the quick math: if pre-opening work does not produce scheduled visits, the clinic starts below capacity and cash comes in later than planned.
Book Visits Before Open
Before opening, verify the readiness signal: local search setup, Google Business Profile live, payer directory listings checked, referral partners contacted, employer outreach started, community awareness plan active, and pre-opening appointments booked. If those pieces are not live, the clinic may open on time but still miss early revenue.
- Match outreach to each role’s capacity.
- Track booked visits by payer type.
- Push referrals before broad advertising.
- Test scheduling before the first day.
What this estimate hides is no-shows and payer mix. Still, if visits are booked before launch, the clinic can start with billable volume instead of spending opening week chasing demand.
6
Related Products
- Medical Clinic Porter's Five Forces Analysis
- Medical Clinic BCG Matrix
- Medical Clinic Business Model Canvas
- 7 Critical KPIs to Scale Your Medical Clinic
- Medical Clinic Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Medical Clinic Profitability and Margins
- How Much Does It Cost To Run A Medical Clinic Each Month?
- Medical Clinic Startup Costs: $515K CAPEX to Open a Small Clinic
- Medical Clinic Financial Model Template in Excel
- How Much Does a Medical Clinic Owner Make? $3679K Year 1 Model
- How to Write a Medical Clinic Business Plan in 7 Steps
- Medical Clinic Marketing Mix
- Medical Clinic Marketing Plan
- Medical Clinic Business Proposal
- Medical Clinic PESTEL Analysis
- Medical Clinic Pitch Deck Example Editable PPTX
- Medical Clinic Business SWOT Analysis
- Medical Clinic Value Proposition Canvas
Frequently Asked Questions
Start by defining the service scope, then verify state rules, ownership limits, medical director needs, malpractice coverage, facility requirements, and payer strategy Build the opening plan around the modeled Year 1 team: 2 physicians, 1 nurse practitioner, 2 medical assistants, 1 specialist, and 1 phlebotomist Then test EHR, scheduling, billing, and first-visit workflows before opening