 Owner income$3.68M to $486M
Owner income$3.68M to $486MHow Much Does a Medical Clinic Owner Make? $3679K Year 1 Model

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$3.68M to $486M  Net margin40.4% to 80.2%
Net margin40.4% to 80.2% Revenue for target pay$9.1M to $606M
Revenue for target pay$9.1M to $606M Business difficultyHard
Business difficultyHard


In the supplied assumptions, medical clinic owner income starts from modeled operating profit of about $3679K in the first year on $9095K of collected revenue By the mature year, revenue reaches about $606M and modeled operating profit reaches about $486M, before personal taxes, reserves, debt principal, and unlisted provider payroll These are model outputs, not guaranteed earnings or universal averages The main levers are visit volume, collections per visit, staffing costs, payer mix, billing performance, and overhead
Owner income$3.68M to $486MNet margin40.4% to 80.2%Revenue for target pay$9.1M to $606MBusiness difficultyHardWant to test your clinic owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Medical Clinic model?
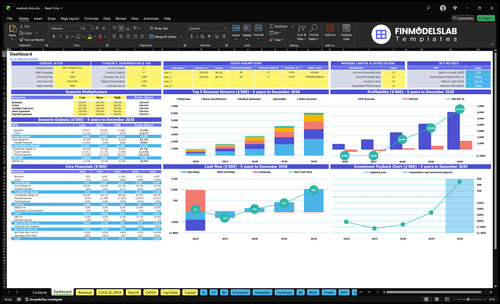
This Medical Clinic Financial Model Template dashboard pulls assumptions, revenue build, staffing, expenses, scenarios, owner income, charts, and cash flow into one view, with $9,095K and $606M revenue anchors. Open the model.
Owner-income model highlights
- Owner take-home output
- Visit-based revenue build
- Scenarios test costs
How does a physician owner compare with a nonclinical clinic owner?
A physician owner can earn from clinical labor plus profit distributions, while a nonclinical owner usually has to pay clinicians, may need a medical director, and carries more management payroll. For Medical Clinic, the supplied data shows provider counts and visit capacity, but it does not show provider salary lines, so the ownership math is incomplete. Because ownership and supervision rules vary, use counsel before you set the structure.
Physician owner
- Can earn wages and profit
- Clinical labor is part of earnings
- Separation matters for clean math
- Visit capacity drives revenue
Nonclinical owner
- Usually pays hired clinicians
- May need a medical director
- Management payroll is usually higher
- Rules need legal review first
What costs reduce medical clinic profit margin most?
For a Medical Clinic, the biggest profit-margin hits are the $196K monthly fixed overhead and the 150% first-year variable cost load; see How Much Does It Cost To Open And Launch Your Medical Clinic Business? for the setup side. Wages add $170K in year one, so labor and overhead both pressure margin hard. Keep gross margin, operating profit, reserves, and owner take-home separate so the cash picture stays clear.
Fixed cost pressure
- $196K monthly fixed costs
- $2.352M annual fixed costs
- $170K added wages in year one
- Overhead cuts profit before growth helps
Variable cost pressure
- 150% first-year variable costs
- 50% supplies burden
- 30% external labs burden
- 40% billing plus 30% marketing add more drag
What revenue is needed to pay a medical clinic owner?
Medical Clinic needs about $4.767M in annual revenue to cover $4.052M of first-year fixed costs and wages before owner pay, assuming 15% variable costs and an 85% contribution margin. Add owner pay on top of that, and the first-year revenue target rises to about $9.095M. Here’s the quick math: divide $4.052M by 0.85, then add owner pay to the numerator before dividing again.
Core math
- $4.052M fixed costs and wages
- 15% variable costs
- 85% contribution margin
- $4.767M break-even before owner pay
Owner pay target
- Add owner pay to the numerator
- Then divide by 85%
- First-year revenue target: $9.095M
- Revenue alone does not set pay
Want to see what drives clinic owner income?
1
874-4,841Visit Volume
Monthly visits scale from 874 in Year 1 to 4,841 in Year 5, and that is the biggest swing in owner take-home.
2
$30-$280Payer Mix
Modeled service prices run from $30 to $280, so better reimbursement raises revenue fast before labor and fees hit.
3
$795KStaffing Mix
Year 1 wages are about $795K, so every added provider only helps if it brings enough billable visits.
4
$250-$280Acuity Mix
A bigger share of specialist-level care at $250 to $280 per service lifts average revenue per visit.
5
$235KFixed Overhead
Fixed non-wage costs run about $235K a year, so rent, software, and insurance keep pressure on breakeven.
6
3.5%-4.0%Billing Fees
Billing and collections fees start at 4.0% in Year 1 and ease to 3.5% by Year 5, so weak collections cut take-home directly.
Medical Clinic Core Six Income Drivers
Patient Visit Volume
Patient Visit Volume
Patient visit volume is the main top-line driver in a fee-for-service clinic. The model shows 874 monthly visits and $758K monthly revenue in year 1, then 4,841 visits and $5,047K monthly revenue at maturity. Here’s the quick math: that is about $868 per visit early and $1,043 per visit later, before expenses hit owner pay.
Visits depend on provider count, monthly treatment capacity, and utilization (filled capacity). More volume only helps if extra collections cover the added staffing, supplies, billing, and admin costs. If booked slots rise but rooms, clinicians, or front desk hours do not, revenue leaks into overtime, delays, and lower margins.
Fill Capacity Without Breaking Margin
Track visits per provider, open slots, and show rate each month. The useful test is simple: incremental revenue per added visit must stay above the full variable cost of that visit. If a new provider or extra sessions add volume but the clinic cannot collect enough cash after claims and patient balances, owner income drops even when the schedule looks full.
Use a weekly capacity plan. Match provider hours to demand, then test one change at a time: more sessions, longer clinic hours, or a different service mix. If utilization stays low, fixed overhead still sits on top of the same base; if utilization rises, the same rent and admin spread across more visits and protect take-home pay.
1
Payer Mix And Reimbursement
Payer Mix And Reimbursement
Here, reimbursement is modeled through treatment price, not a fixed payer rate. Prices range from $30 for phlebotomy to $250 for specialist visits, and the weighted first-year revenue per visit is disclosed at $8,672. That means small shifts in service mix can move booked revenue and the owner’s pay fast.
What this estimate hides is cash timing. Denials (claims the payer rejects), allowed amounts (the amount the plan will pay), patient balances, and slow payment can pull cash below billed revenue, so profit on paper does not always turn into money the owner can draw.
Test Payer Mix Before You Hire Ahead
Model payer mix (the share of patients by plan), visit type mix, service price, denial rate, allowed amount, and days to collect. If specialist visits rise, revenue per encounter improves; if lower-priced visits dominate, the same visit count can support much less owner income.
- Track revenue per completed visit.
- Test payer mix monthly.
- Watch denials and patient balances.
- Stress cash flow, not just revenue.
Build sensitivity cases around payer mix, not one base case. If reimbursements soften or collections slow, reduce owner draws early so payroll, rent, and billing costs stay covered.
2
Owner Role And Provider Payroll
Provider Payroll Pressure
Provider payroll is the fastest way owner pay changes in a clinic. The model shows provider counts, but it does not show provider salary lines, so profit can look healthy until clinician pay is added. If the owner also treats patients, split clinical pay from profit distributions so you know what the practice earns versus what the owner earns.
Nonclinical owners need enough paid providers, management coverage, and sometimes a medical director. The model already shows admin wages of $170K in year 1 and $235K in later scale years, so provider payroll has to fit around those fixed labor costs or owner draw gets squeezed fast.
Track Pay Before You Scale
Track provider headcount, scheduled hours, visits per provider, and total payroll as a share of revenue. Here’s the quick math: if new providers add visit capacity but payroll rises faster than collections, owner income falls even when top-line revenue grows. That is the risk to watch.
Set pay rules before hiring: salary, production bonus, and coverage cost for admin or medical director time. Use pay per visit and revenue per provider as control metrics, and test each hire against the clinic’s fixed wage base of $170K to $235K so the owner does not absorb hidden labor drag.
3
Service Mix And Ancillary Revenue
Service Mix Revenue Per Encounter
Service mix changes how much each patient visit earns. In this model, first-year prices are $150 for physician visits, $120 for nurse practitioner visits, $40 for medical assistant visits, $250 for specialist visits, and $30 for phlebotomy specialist services. A mix with more physician and specialist care raises revenue per encounter and can lift owner profit if added labor and billing costs stay controlled.
Lab-related services can add visit volume, but they do not always add much margin. Here’s the quick math: higher-priced visits improve top-line revenue faster than low-priced support services, yet every added service still needs payer coverage, staff, compliance, and patient demand. If the clinic cannot bill for the service cleanly, the extra volume can raise work without raising take-home income.
Track Mix By Service Line
Measure revenue and margin by service type each month. Track visits, revenue per encounter, and labor hours for physician, nurse practitioner, medical assistant, specialist, and phlebotomy work. That shows which services actually fund owner pay and which ones just fill the schedule.
Use payer contracts and staffing limits before adding any service. Test demand before opening more specialist or lab slots, and watch denials and unfilled appointments closely. If a low-price service adds volume but no margin, trim it or bundle it only where the payer and workflow support it.
- Track revenue per encounter by service
- Compare margin by provider type
- Check contract coverage before launch
- Watch staffing and compliance load
- Cut services with thin contribution
4
Operating Overhead
Clinic Overhead
This driver is the clinic’s fixed cost base: $196K/month in overhead, including $10K rent, $3K malpractice insurance, $2K for electronic health record software, $15K utilities, and other admin costs. First-year listed wages add $170K, so owner pay gets tight until visit volume covers the load.
Overhead reduces profit before owner distributions. When capacity fills, each extra visit helps spread fixed costs across more revenue; when visits lag, cash flow stays thin and the draw to the owner gets pushed down.
Track Overhead Per Visit
Measure overhead against booked visits, not just total spend. The key inputs are rent, malpractice, software, utilities, admin costs, and wages, then compare them with monthly visit volume so you can see whether the clinic is paying too much for the demand it has.
- Track overhead per visit each month.
- Watch payroll as visits rise.
- Fill open slots before adding costs.
5
Collections, Denials, And No-Shows
Collections, Denials, and No-Shows
Collections rate changes cash, not just booked revenue. In year one, billing and collections fees are 40% of revenue, then fall to 35% in the mature year, so slower cash capture can eat owner draw even when visits are booked. Eligibility checks, coding, denial follow-up, and patient balances all affect when cash lands.
No-shows cut filled capacity, so the clinic can lose revenue while rent, wages, and other fixed costs stay flat. That means owner pay drops twice: fewer collected visits and the same overhead base. Here’s the quick math: if a slot goes empty, you lose the service revenue and the chance to spread fixed costs over one more visit.
Track Cash Capture, Not Just Charges
Measure collection rate, denial rate, days in accounts receivable, and no-show rate by provider and visit type. If denials rise, fix eligibility checks and coding first, because those are the fastest cash levers. If no-shows rise, tighten reminders and same-day fill rules so the clinic keeps capacity paid.
- Reconcile charges to cash weekly.
- Track denied claims by reason.
- Monitor empty slots by provider.
6
Compare low, base, and high clinic owner income scenarios
Owner income scenarios
Owner income changes fast as visit volume rises and staffing fills out. Early years carry heavy fixed payroll and setup costs, while mature years spread those costs across more visits.
| Scenario | Low CaseDownside | Base CaseBase Case | High CaseUpside |
|---|---|---|---|
| Launch model | The low case assumes a slow first-year ramp and negative operating profit before taxes and debt. | The base case assumes the third-year operating model, where volume is high enough to clear fixed costs. | The high case assumes mature-year scale and the strongest profit path before taxes and debt. |
| Typical setup | Year 1 runs at 874 monthly visits with 60% to 75% provider capacity, high startup payroll, and fixed rent-led overhead. | Year 3 runs at 2,387 monthly visits with fuller provider schedules, more staff, and positive operating profit. | Year 5 runs at 4,841 monthly visits with higher provider counts, stronger capacity use, and the widest cost spread. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | -$380k to -$241kLow Income | $226k to $581kBase Income | $581k to $1.422MHigh Income |
| Best fit | Use this to stress-test a slow ramp, longer cash burn, and early staffing pressure. | Use this as the core planning case for lender talks, hiring, and monthly cash targets. | Use this to test upside if the clinic fills capacity faster and holds costs down. |
Planning note: These ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. They exclude personal taxes, reserves, debt principal, and any unlisted provider payroll.
Related Products
- Medical Clinic Porter's Five Forces Analysis
- Medical Clinic BCG Matrix
- Medical Clinic Business Model Canvas
- 7 Critical KPIs to Scale Your Medical Clinic
- Medical Clinic Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Medical Clinic Profitability and Margins
- How Much Does It Cost To Run A Medical Clinic Each Month?
- Medical Clinic Startup Costs: $515K CAPEX to Open a Small Clinic
- Medical Clinic Financial Model Template in Excel
- How To Open A Medical Clinic: 6–12 Month Launch Plan
- How to Write a Medical Clinic Business Plan in 7 Steps
- Medical Clinic Marketing Mix
- Medical Clinic Marketing Plan
- Medical Clinic Business Proposal
- Medical Clinic PESTEL Analysis
- Medical Clinic Pitch Deck Example Editable PPTX
- Medical Clinic Business SWOT Analysis
- Medical Clinic Value Proposition Canvas
Frequently Asked Questions
Under the supplied model, operating profit is about $3679K in the first year and about $486M in the mature year That is before personal taxes, debt principal, reserves, and any provider salaries not shown as expense lines Treat this as a planning case, not a guaranteed owner salary