 Time to Open6 monthsLaunch runway
Time to Open6 monthsLaunch runwayHow To Open A Mental Health Clinic In 3 To 9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6 monthsLaunch runway  Launch Sequence8 stagesCompliance first
Launch Sequence8 stagesCompliance first Key BottleneckLicense gateState rules
Key BottleneckLicense gateState rules First Revenue StepPrivate-pay visitsCash pay first
First Revenue StepPrivate-pay visitsCash pay first


To open a mental health clinic, set up the business, confirm state-specific licensing rules, hire credentialed clinicians, install Health Insurance Portability and Accountability Act compliant systems, test intake, and choose a private-pay, insurance, or mixed revenue path A practical opening timeline is 3 to 9 months, but state rules, payer enrollment, and staffing can move that date The researched planning case starts with 13 clinicians, modeled Year 1 utilization of about 996 visits per month, and about $158,840 in monthly revenue once those capacity assumptions hold Your first revenue usually comes from private-pay sessions, referral-driven appointments, or insurance visits after payer approval
Time to Open6 monthsLaunch runwayLaunch Sequence8 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepPrivate-pay visitsCash pay firstLaunch timeline
This short web summary shows the launch timeline, and the XLSX export carries the full Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Legal & licensing
- Entity filing
- State license review
- Malpractice coverage
- NPI enrollment
- Policy drafting
Facility & systems
- Lease review
- Build-out plan
- Telehealth workflow
- Equipment install
EHR & billing
- EHR setup
- Billing rules
- Payer enrollment
- Consent forms
- Test claims
Hiring & training
- Hire clinicians
- Credential review
- Schedule templates
- Intake training
- Clinical training
Marketing & intake
- Website launch
- Referral outreach
- Lead capture
- Intake scripts
- Appointment reminders
Finance & ops
- Budget lock
- Cash forecast
- Payroll setup
- Launch review
- Weekly cash check
Why test the clinic launch plan before go-live?
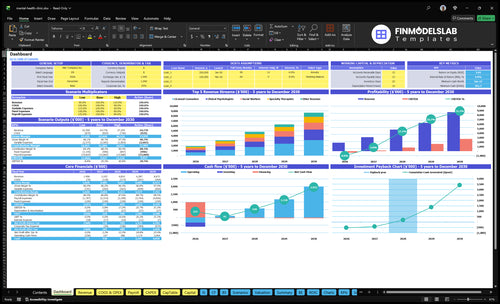
This screenshot in the Mental Health Clinic Financial Model Template shows revenue, costs, cash needs, assumptions, and break-even logic—open the model.
Financial model highlights
- 13 providers at launch
- 996 visits monthly volume
- $158,840 monthly revenue
- 14% variable costs
- $16,600 fixed overhead
What mistakes create the biggest mental health clinic launch risks?
The biggest launch mistake for a Mental Health Clinic is opening before licensing and payer rules are clear, because the clinic can burn through $16,600 in monthly fixed overhead fast if claims stall or intake stays thin. Here’s the quick math: weak documentation, no referral pipeline, poor scheduling, and slow onboarding can delay collections even when demand exists.
Big launch risks
- Check state licensing first
- Confirm payer rules early
- Test EHR notes and claims
- Map referral sources before opening
Simple readiness checks
- Set same-day intake response
- Build provider calendars in advance
- Model collections lag
- Stress-test cash runway
How do you get clients for a mental health clinic?
For a Mental Health Clinic, the first clients usually come from referral partners, primary care offices, directories, local search, and insurance listings, so the launch goal is booked appointments, not broad awareness. If you want the startup math too, read How Much Does It Cost To Open, Start, And Launch Your Mental Health Clinic? and build your referral list before go-live. If Year 1 needs 996 monthly visits, that is about 249 visits per week, so weekly referral targets have to match provider capacity. The real bottleneck is demand that does not turn into kept sessions.
Best first sources
- Referral partners first
- Primary care relationships
- Therapist and insurance directories
- Local search and employer links
Launch setup
- Confirm accepted payer terms
- Publish clinician specialties
- Answer intake fast
- Cut scheduling friction
How does insurance credentialing affect the mental health clinic launch timeline?
Insurance credentialing can push a Mental Health Clinic launch into a 3 to 9 month window, and the timing depends on payer enrollment, contracts, and how ready your operations are. If cash runway is tight, start with private-pay or out-of-network, because revenue can start sooner once clinicians, consent, billing, and intake are ready. The real bottleneck is opening with staff booked but no clear path to collected revenue.
Launch sooner
- Private-pay can start revenue earlier
- Get clinicians ready first
- Set consent and intake forms
- Confirm billing workflow is live
Insurance launch
- Enroll with each payer
- Load fee schedules correctly
- Set claims and denial workflows
- Plan for collection lag
Verify the clinic is ready to accept patients safely and bill cleanly
Launch readiness checklist
Use this go-live approval checklist before opening to confirm compliance, staffing, systems, and cash are ready.
Compliance
- Entity structure approvedCritical
The clinic needs a legal home before licenses, contracts, and payroll move ahead.
- State licenses verifiedCritical
All required clinic and clinician licenses must be active before any patient visit.
- Malpractice coverage boundCritical
Coverage should be in force before staff see clients or deliver treatment.
- Clinical scope documentedHigh
Clear service boundaries reduce risk when intake, referrals, and treatment plans start.
Privacy
- HIPAA policies finalizedCritical
Privacy rules must be set before records, messages, and visit notes go live.
- Consent forms approvedCritical
Patients need clear consent before therapy, testing, or psychiatric treatment begins.
- Release forms approvedHigh
Release forms are needed for coordinated care and outside provider communication.
- Incident reporting definedHigh
A written response path helps staff act fast on privacy or safety events.
Facility
- Treatment rooms inspectedHigh
Private rooms need to support safe sessions and protect client confidentiality.
- Security system testedHigh
Security should work before staff, records, and equipment are on site.
- Accessibility path clearedMedium
Clients and staff need a clear path into the clinic without barriers.
Systems
- EHR workflow testedCritical
The EHR must handle notes, records, and client files without launch-day errors.
- Telehealth visits testedHigh
Remote care should work before any patient relies on it.
- Scheduling flow testedCritical
Booking must be smooth so intake does not stall at the first step.
- Claims workflow testedCritical
Claims need to move cleanly or cash will lag right after launch.
- Secure messaging testedHigh
Secure chat should protect patient data and support quick follow-up.
Staffing
- Year 1 roster matchedCritical
The opening roster should match the Year 1 plan: 3 psychologists, 4 counselors, 3 social workers, 1 psychiatrist, 2 specialty therapists.
- Licensure checks completedCritical
Each clinician must have verified credentials before any appointment is booked.
- Coverage schedule approvedHigh
Coverage has to support intake, therapy, psychiatry, and follow-up work.
- Referral sources namedMedium
Named referral paths help fill the first schedule and reduce empty slots.
Runway
- Cash runway confirmedCritical
The model needs to hold the $361k minimum cash level before opening.
- Month 13 floor fundedCritical
Cash must stay above the Month 13 low point or launch risk climbs fast.
- First revenue model checkedHigh
Year 1 should still work at 996 monthly visits, $158,840 revenue, 14% variable cost, and $16.6k fixed overhead.
- Go-live signoff completeCritical
No blocker should remain in compliance, intake, billing, staffing, or cash runway.
Want the six drivers that decide launch readiness?
1Licensing
3-9 moThe clinic can't open until licenses, policies, forms, and supervision rules are signed off.
2Billing Setup
Claims livePayer approval and tested claims protect cash flow, so visits start collecting sooner.
3Clinical Staffing
13 providersThirteen Year 1 providers set day-one coverage, and hiring too early leaves paid hours empty.
4EHR Ops
EHR liveA tested EHR flow keeps intake, notes, telehealth, and billing moving without missed handoffs.
5Referral Intake
Intake speedFast intake and active referral channels turn marketing into kept sessions, not empty leads.
6Cash Runway
$361KRunway has to cover the $361K cash trough before Month 14 breakeven, or launch slows.
Licensing And Compliance
Licensing Gate
A mental health clinic cannot open safely until entity setup, state rules, clinician licenses, malpractice coverage, privacy policies, consent forms, documentation standards, and supervision rules are all done. This is the launch gate: if one item is missing, the first appointment slips, and day-one care can be delayed.
The readiness signal is a signed-off compliance checklist and trained staff. Because licensing is state-specific, confirm requirements with regulators and advisors before you book clients. If patient care starts before required permissions or forms are complete, you raise legal, billing, and care-quality risk right at launch.
Checklist Before Scheduling
Start with the order that blocks opening: form the entity, confirm state rules, then verify each clinician’s license, malpractice policy, privacy notice, consent package, and supervision plan. Test the documentation flow before go-live so intake, notes, and release forms are ready on day one.
What this prep protects: fewer launch delays, cleaner records, and less avoidable billing trouble. The clinic should not schedule active visits until every required form is approved and every staff member knows the process. One missed approval can stop revenue and force a reset.
- State licensing requirements
- Clinician licenses
- Malpractice coverage
- Privacy and consent forms
- Documentation standards
- Supervision rules
- Staff training sign-off
1
Credentialing And Billing Setup
Credentialing and Billing Setup
Credentialing is the gate between a completed session and cash in the bank. For a mental health clinic, that means payer enrollment, fee schedules, billing workflows, claims testing, private-pay policy, denial management, and collection tracking must be ready before the first visit if insurance is part of go-live.
The launch risk is simple: if each clinician does not have clear payer status, visits may still happen, but revenue can stall. A tested billing path lowers unpaid sessions and improves cash timing; if payer approval slips, the clinic may need to open with private-pay only and delay insured volume.
Pre-Open Billing Readiness
Use a launch checklist that shows payer status by clinician, fee schedule setup, claims test results, and who owns denials and collections. Do not count on insurance revenue until each payer has approved the clinician and the billing path has been tested end to end.
Build the plan around the real Year 1 load: 25% billing service fees and 8% marketing and client acquisition are part of the variable expense model. The quick test is whether the clinic can send a claim, get it accepted, track the balance, and know when the money is due.
- Confirm payer enrollment status
- Load contracted fee schedules
- Test claims before opening
- Set private-pay rules
- Assign denial follow-up
- Track collections weekly
2
Clinical Staffing And Provider Capacity
Clinical Staffing And Capacity
A mental health clinic can’t open cleanly unless the schedule is real on day one. The Year 1 plan calls for 3 clinical psychologists, 4 licensed counselors, 3 social workers, 1 psychiatrist, and 2 specialty therapists, but coverage only works if licenses, supervision, and admin support are already in place. Utilization is modeled from 50% for psychiatrists to 65% for licensed counselors, so staffing too early can leave you with empty paid hours.
The key risk is hiring before referral volume or credentialing is ready. That creates payroll before sessions, plus gaps in specialty coverage if one provider type is missing. Readiness means active licenses, open calendars, approved specialties, and supervision coverage lined up before the first client books. One clean rule: don’t staff for hope, staff for booked demand.
Lock Coverage Before Hiring
Build the roster in the same order patients will use it: confirm licenses, then payer status, then calendars, then admin support. Here’s the quick check: if the psychiatrist is only 50% utilized and counselors are at 65%, the opening schedule still needs enough demand to fill those hours without dragging cash. That keeps day-one access real instead of theoretical.
- Verify every active license first.
- Match specialties to referral demand.
- Test supervision and admin handoffs.
3
EHR And HIPAA Operations
EHR Workflow Ready
A mental health clinic cannot open cleanly until the full EHR workflow works: scheduling, intake, telehealth, consent, clinical notes, billing, claims, and secure messaging. The fixed base assumption is $1,500 per month for the EHR platform, plus 2% Year 1 telehealth platform usage fees. If that stack is not live before day one, visits can happen, but they won’t reliably turn into compliant notes or clean claims.
The launch gate is a tested patient journey from inquiry to completed note and bill. Here’s the risk: if forms, reminders, billing rules, or HIPAA settings are missing, you get dropped leads, delayed documentation, and slower cash collection. One clean workflow matters more than extra software features.
Test the Full Patient Flow
Before opening, verify the setup in order: HIPAA policies, staff training, form library, appointment reminders, and billing rules. Then test a real case flow: inquiry, booking, intake, telehealth check-in, consent capture, session note, claim, and secure follow-up. If one step fails, launch-day throughput drops and staff end up fixing process gaps instead of seeing patients.
Use the first test to find the weak link, not after revenue starts. If the EHR is live but forms are incomplete or reminders do not send, the clinic can still miss visits and delay billing. That hits both patient experience and early cash flow.
- Load every consent form.
- Train staff on HIPAA workflows.
- Test reminders and secure messages.
- Confirm billing rules before go-live.
4
Referral Pipeline And Intake
Referral Pipeline And Intake
For a mental health clinic, referral pipeline and intake is what turns launch marketing into booked visits. You do not open strong on day one unless named referral partners, live directory profiles, and a clear scheduling script are already in place, because the clinic’s first revenue comes from getting inquiry calls into kept sessions fast.
The main risk is not lack of interest; it is traffic or referrals that never convert. With 8% of revenue modeled for Year 1 marketing and client acquisition, the plan has to track each source to an appointment and then to a kept session. If intake is slow, launch-week utilization drops, cash comes in later, and staffing looks fuller than it really is.
Build Intake Before You Open
Set up the referral mix before go-live: referral relationships, online directories, local search, payer directories, community partners, employers, schools, and primary care offices. Each source needs a live profile, a contact path, and one owner who responds fast and books the visit. One clean script beats a long sales process.
- Confirm named referral partners
- Publish live profiles
- Test intake response timing
- Train the scheduling script
- Track source to kept session
Here’s the quick math: if marketing is fixed at 8% of revenue, weak intake can waste that spend fast. What this estimate hides is the gap between booked and kept sessions, so test the handoff before opening. If your team cannot answer, schedule, and confirm quickly, day-one capacity will sit empty even when leads are coming in.
5
Capacity Planning And Cash Runway
Cash Runway and Capacity Fit
A mental health clinic can only open cleanly if provider calendars, payer mix, and claim timing line up with real demand. At modeled capacity of 996 visits/month and $158,840 in monthly revenue, the schedule has to be built around actual available hours, not wishful volume.
Here’s the quick math: 14% variable expenses leave about 86% contribution before fixed overhead and wages. With $16,600 in fixed monthly overhead before wages, a slow ramp or delayed reimbursement can create a cash gap even when the clinic looks busy on paper.
Model the First-Days Cash Need
Build the launch plan from provider hours out. Test the schedule against expected sessions, payer mix, and reimbursement timing before you commit to staffing and rent. One clean rule: if the visit flow is not tied to cash timing, the opening date is too optimistic.
- Map provider hours by role.
- Count expected kept sessions.
- Separate payer and self-pay visits.
- Track claim-to-cash timing.
- Cover $16,600 overhead first.
- Hold cash for wages and delays.
If the first month lands below plan, the clinic still has to pay overhead, wages, and billing costs while collections catch up. That is why launch readiness here is not just about filling the calendar; it is about proving the calendar can fund the business from day one.
6
Related Products
- Mental Health Clinic Porter's Five Forces Analysis
- Mental Health Clinic BCG Matrix
- Mental Health Clinic Business Model Canvas
- 7 Essential KPIs for Mental Health Clinic Growth
- Mental Health Clinic Business Plan Template in Pre-Written Word
- 7 Proven Strategies to Boost Mental Health Clinic Profit Margins
- Analyzing Monthly Running Costs for a Mental Health Clinic
- Mental Health Clinic Startup Costs: $245K+ CAPEX Before Runway
- Mental Health Clinic Financial Model Template in Excel
- How Much Does A Mental Health Clinic Owner Make At $19M-$87M?
- How to Write a Mental Health Clinic Business Plan in 7 Steps
- Mental Health Clinic Marketing Mix
- Mental Health Clinic Marketing Plan
- Mental Health Clinic Business Proposal
- Mental Health Clinic PESTEL Analysis
- Mental Health Clinic Pitch Deck Example Editable PPTX
- Mental Health Clinic Business SWOT Analysis
- Mental Health Clinic Value Proposition Canvas
Frequently Asked Questions
Start with state rules, clinician licensing, malpractice coverage, HIPAA-ready systems, and a clear payer or private-pay plan The researched Year 1 case uses 13 providers, about 996 monthly visits at modeled utilization, and roughly $158,840 in monthly revenue once capacity assumptions hold Build the opening plan before signing long fixed-cost commitments