 Owner incomeNot defensible
Owner incomeNot defensibleHow Much Does A Mental Health Clinic Owner Make At $19M-$87M?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner incomeNot defensible  Net margin-17% to 32%
Net margin-17% to 32% Revenue for target pay$2.7M
Revenue for target pay$2.7M Business difficultyHard
Business difficultyHard


A mental health clinic owner’s take-home can’t be stated as a fixed salary from these assumptions because the payroll data is incomplete and taxes, debt service, and reserves are excluded The clinic generates about $158,840 per month in the first year and $722,600 per month by Year 5 under the provided volume, pricing, and utilization assumptions After visible costs only, the first-year pre-tax surplus ceiling is about $525k, but that excludes unprovided clinician wages for several roles and cash kept in the clinic Treat that as planning capacity, not guaranteed owner income
Owner incomeNot defensibleNet margin-17% to 32%Revenue for target pay$2.7MBusiness difficultyHardWant to test your clinic owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from monthly revenue, margin, operating costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Actual owner take-home depends on collections, payroll, taxes, reserves, and owner draws; it is not guaranteed salary, tax advice, or owner distribution advice.
Need the full Mental Health Clinic financial model?
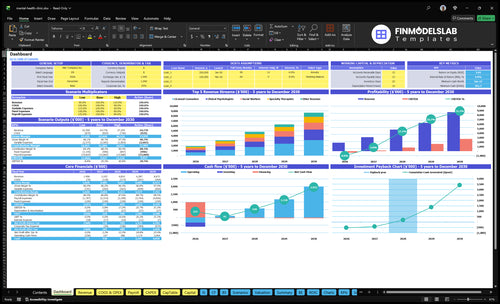
The dashboard shows revenue, margin, cash, and owner-income outputs, with assumptions for providers, sessions, pricing, utilization, payroll, fixed costs, COGS, and variable expenses in the Mental Health Clinic Financial Model Template; open it to test low, base, and high utilization, plus owner-pay sensitivity.
Owner-income model highlights
- Owner pay sensitivity
- Revenue and margin dashboard
- Low, base, high cases
How much revenue does a mental health clinic need to pay the owner?
A Mental Health Clinic needs about $1.47M in revenue to cover the visible $150k owner target, $915k payroll, and $1,992k fixed overhead before reserves. The first-year revenue figure shown is $1.91M, but the real need is higher once clinician wages and any reserve policy are added.
Visible cost base
- $150k owner target pay
- $915k first-year payroll
- $1,992k fixed overhead
- Minimum revenue: about $1.47M
What still moves the target
- Fee-for-service means session volume matters
- Revenue depends on delivered treatments
- Practitioner capacity drives monthly revenue
- Clinician wages and reserves lift the need
Can a mental health clinic owner make money?
Yes, a Mental Health Clinic owner can make money, but take-home pay depends on what’s left after payroll, fixed costs, reserves, and taxes. Here’s the clean read: first-year collected revenue is listed at $191M from 13 providers at 500%-650% utilization, but What Is The Current Growth Rate Of Patient Engagement At Your Mental Health Clinic? matters because filled sessions drive collections. If the owner also works as Clinical Director, the $150k salary may be labor pay, not profit, and missing payroll lines mean final owner income cannot be stated.
What Pays
- $191M first-year collected revenue
- 13 provider revenue base
- 500%-650% utilization range
- Fee-for-service session model
What Limits Take-Home
- $150k Clinical Director salary
- Therapist wages are not profit
- Need full payroll detail
- Taxes and reserves still apply
Which mental health clinic costs reduce owner take-home most?
For a Mental Health Clinic, clinician payroll is the biggest owner take-home drain: Clinical Psychologists and Licensed Counselors alone are listed at $605k in Year 1 and $172M in Year 5, while admin payroll starts at $310k/year and rises to $3,825k/year. Fixed overhead is $166k/month, and if you’re sizing launch costs, see How Much Does It Cost To Open, Start, And Launch Your Mental Health Clinic? because every dollar added before reserve cuts owner distribution capacity.
Biggest cash drains
- Clinician payroll hits take-home first
- $605k Year 1 for key clinicians
- $172M Year 5 clinician cost listed
- $310k/year admin payroll starts the burn
Other margin drains
- $166k/month fixed overhead stays high
- Billing and tools take 40% of Year 1 revenue
- Marketing plus telehealth equal 100% of Year 1 revenue
- More spend before reserve means less owner draw
Want the six biggest income drivers?
1
$159-$182Collected rate
More cash per session drives revenue, and the model rises from about $159 in Year 1 to about $182 in Year 5.
2
50%-85%Utilization
Booked clinician time spreads payroll across more sessions, so higher utilization lifts owner income fast.
3
$1.48M-$3.71MProvider pay
Staff pay is the biggest cost block, with payroll rising as headcount grows from Year 1 to Year 5.
4
Month 14Payer mix
The right mix of payers and fast collections decides how much billed revenue turns into cash, and break-even lands in Month 14.
5
$16.6K/moFixed overhead
Rent, software, insurance, and admin costs must be covered every month before owner draws start.
6
35 moOwner scale
Owner take-home depends on what is left after payroll, reserves, and tax planning, and payback is about 35 months.
Mental Health Clinic Core Six Income Drivers
Collected Revenue Per Session
Collected Revenue Per Session
Collected revenue per session is the cash you actually keep for each completed visit, after payer contracts, denials, and write-downs. In Year 1, the weighted benchmark is about $159/session; by Year 5 it rises to $182/session. That lifts revenue without adding clinical hours first-year prices range from $130 for Social Workers to $250 for Psychiatrists.
Billed charges are not collections. In Year 5, prices range from $150 to $280, but what matters is what lands in cash. If payment delays stretch out or contract terms weaken, owner income drops even when the schedule is full.
Track net collections, not posted rates
Measure collected dollars per completed session, plus denial rate and days to cash. Here’s the quick math: at 996 sessions/month, every $1 change in collected revenue per session changes monthly revenue by about $996; every $10 changes it by $9,960.
Watch payer contracts, because fee cuts or slow remits can erase price gains. Tie forecasts to collected revenue, not charge sheets, so you can tell whether owner draw is coming from better pricing, better collections, or just more visits.
- Track collected dollars per session.
- Track denial rate and lag.
- Separate charges from cash.
1
Clinician Utilization And Session Volume
Clinician Utilization
Utilization turns available clinical time into billed visits, so it drives revenue without adding much fixed cost. In year 1, utilization ranges from 500% for Psychiatrists to 650% for Licensed Counselors, with collected sessions at about 996/month. By year 5, utilization reaches 750% to 850% and volume rises to about 3,966/month.
That gap matters for owner pay. Cancellations, no-shows, and ramp-up reduce collected sessions even when headcount looks strong, so payroll and overhead can outrun cash. The key inputs are provider count, scheduled hours, show rate, and average completed sessions per clinician. One clean takeaway: more kept visits usually means more take-home, unless staffing or billing costs rise faster.
Track Kept Visits, Not Just Headcount
Measure scheduled sessions, completed sessions, cancellation rate, and no-show rate by clinician type. If a clinician is on payroll but not converting time into completed visits, the clinic is leaking margin. Forecast monthly collections as completed sessions × collected revenue per session, then compare that to payroll and fixed overhead.
Set a simple target: close the gap between booked and kept visits first. If year 1 lands near 996 collected sessions/month and year 5 near 3,966/month, the business only scales if onboarding is fast and schedules stay full. One missed visit is small; hundreds of missed visits a month is owner income.
2
Provider Compensation Model
Provider Payroll
Payroll sets gross margin after clinicians are paid, so this driver hits owner income fast. In year 1, visible payroll is $285k for Clinical Psychologists and $320k for Licensed Counselors; by year 5, those lines rise to $760k and $960k. If compensation grows faster than collected revenue, the owner’s draw gets squeezed.
This driver includes base pay, benefits, supervision time, retention costs, and admin work tied to employee status. Contractor pay can look lighter on paper, but it can still carry higher supervision or turnover costs. The key inputs are provider count, pay mix, benefit load, and collected revenue per session. Higher payroll only helps if collections rise faster.
Track Pay Per Collected Session
Watch payroll as a % of collected revenue, not just headcount. Build the model from collected sessions, average collected rate, and all provider comp tied to each role. That shows whether a new hire adds margin or just adds cost. One clean rule: if a role adds more pay than it adds collections, owner income falls.
- Track pay by provider type.
- Include benefits and supervision.
- Separate employee and contractor costs.
- Compare payroll growth to collections.
Test comp plans against volume and mix. A full-time clinician with weak utilization can raise fixed payroll without lifting revenue enough to cover it. Also, document who handles admin time, since employee models usually add more oversight. Classification is not a financial shortcut.
3
Payer Mix And Collections
Payer Mix And Net Collections
Payer mix changes collected revenue, not just posted charges. An insurance-heavy clinic can add volume, but cash still gets shaved by billing fees, denials, and slow pay. With billing service fees at 25% of revenue in Year 1 and 20% in Year 5, owner income depends on net collections, not session count.
Self-pay usually keeps more of each dollar, but it depends on demand and positioning. The key input is collected revenue per session—about $159 in Year 1 and $182 in Year 5. What this hides is timing: posted revenue can look strong while cash lags behind.
Track Cash By Payer
Model denial leakage, payment lag, and credentialing ramp by payer. A clinic with good volume can still miss owner pay if claims sit unpaid or need rework. Revenue only counts when it lands in cash and stays collected.
- Split self-pay and insurance.
- Track denied claims monthly.
- Measure days to cash.
- Map credentialing start dates.
4
Fixed Overhead And Operating Costs
Fixed Overhead
Fixed overhead is the monthly cost base that hits cash whether the schedule is full or light. Here, researched overhead is $166k/month, including $10k rent, $18k utilities, $15k EHR, $12k insurance, plus smaller facility costs. That means owner take-home drops fast if collected visits slow down, because these bills still land every month.
For break-even, split the $166k fixed monthly cost from per-visit costs like marketing and telehealth. The key inputs are collected sessions, net revenue per session, and the variable cost rate. One clean test: if collections rise but overhead stays flat, profit improves; if utilization dips, fixed costs eat the margin first.
Track Break-Even Monthly
Build the forecast around fixed cost per month, not just headcount or licensed capacity. Track rent, utilities, EHR, insurance, and all other recurring bills separately from per-visit costs. That lets you see the real break-even point before owner pay and avoid mistaking busy calendars for healthy cash flow.
Watch collections per session, session volume, and variable cost share together. If marketing sits at 80% and telehealth at 20% in Year 1, a small drop in visits can wipe out owner draw fast. The practical move is simple: cut nonessential fixed spend before it locks in, and reforecast monthly.
5
Owner Role And Clinic Scale
Owner Role and Scale
Owner income changes with the role mix. If the owner treats clients, income ties to session volume and collection per visit. If the owner manages clinicians, take-home depends more on surplus left after payroll, admin, billing, supervision, and cash timing. The model’s $150k Clinical Director line is labor cost unless it sits on the owner’s pay.
Scale matters because the clinic grows from 13 providers to 35 providers. Bigger teams can create more surplus, but only if scheduling, billing, and supervision stay tight. Less personal clinical work can lift owner profit, but it also adds management risk and more chance of cash leaks if controls are weak.
Track Surplus Per Provider
Measure what the owner actually keeps. Track collected revenue per provider, clinical payroll, the $150k Clinical Director role, and fixed overhead each month. Here’s the quick filter: if added providers raise collections faster than admin, billing, and supervision costs, owner pay can rise; if not, scale just adds complexity.
Watch these inputs closely:
- 13 to 35 providers
- Collections per session
- Clinical payroll
- Billing lag and denials
- Supervisor and admin load
If the owner steps back from treating clients, they need stronger cash controls and faster billing close. That is the trade: less direct revenue, more management leverage. The clinic pays the owner from what is left after labor and overhead, so the real test is whether each new provider adds more surplus than it costs to support them.
6
Compare low, base, and high mental health clinic income scenarios
Owner income scenarios
Owner income shifts with provider count, utilization, and cost load. Early years can look tight, while scaled years show much wider planning ceilings.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | This is the tighter earnings path, where the clinic clears only a small visible surplus. | This is the modeled middle path, with steadier earnings and a wider surplus ceiling. | This is the stronger earnings path, where scale pushes the highest planning ceiling. |
| Typical setup | Year 1 uses 13 providers, $191M revenue, 500%-650% utilization, and 140% direct plus variable costs, so payroll and reserves stay under pressure. | Year 3 uses 24 providers, $481M revenue, and steadier utilization, with the surplus improving as fixed costs spread. | Year 5 uses 35 providers, $867M revenue, and stronger utilization, with scale easing the drag from staffing and variable costs. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $525k ceilingTight ceiling | $257M ceilingMidrange ceiling | $546M ceilingUpside ceiling |
| Best fit | Use this to stress test early cash strain and staffing risk. | Use this as the core operating plan and comparison case. | Use this to test expansion upside and capacity limits. |
Planning note: These figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or owner distributions.
Related Products
- Mental Health Clinic Porter's Five Forces Analysis
- Mental Health Clinic BCG Matrix
- Mental Health Clinic Business Model Canvas
- 7 Essential KPIs for Mental Health Clinic Growth
- Mental Health Clinic Business Plan Template in Pre-Written Word
- 7 Proven Strategies to Boost Mental Health Clinic Profit Margins
- Analyzing Monthly Running Costs for a Mental Health Clinic
- Mental Health Clinic Startup Costs: $245K+ CAPEX Before Runway
- Mental Health Clinic Financial Model Template in Excel
- How To Open A Mental Health Clinic In 3 To 9 Months
- How to Write a Mental Health Clinic Business Plan in 7 Steps
- Mental Health Clinic Marketing Mix
- Mental Health Clinic Marketing Plan
- Mental Health Clinic Business Proposal
- Mental Health Clinic PESTEL Analysis
- Mental Health Clinic Pitch Deck Example Editable PPTX
- Mental Health Clinic Business SWOT Analysis
- Mental Health Clinic Value Proposition Canvas
Frequently Asked Questions
The provided assumptions do not support a final owner-income number because payroll is incomplete The clinic produces $191M in first-year revenue and $867M by Year 5 First-year visible surplus is about $525k before unprovided clinician wages, reserves, taxes, and debt service