 Owner income$317k
Owner income$317kHow Much Does a Mobile Dental Clinic Owner Make? $180K Plus Profit

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$317k  Net margin193% → 557%
Net margin193% → 557% Revenue for target payY1 $59k; Y5 $278k
Revenue for target payY1 $59k; Y5 $278k Business difficultyHard
Business difficultyHard


Key Takeaways
- Filled visits spread fixed costs and lift income.
- Collected revenue matters more than billed charges.
- Service mix lifts average revenue per completed visit.
- Better routes and staffing control break-even volume.
Owner income$317kNet margin193% → 557%Revenue for target payY1 $59k; Y5 $278kBusiness difficultyHardWant to test your own owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Mobile Dental Clinic financial model?
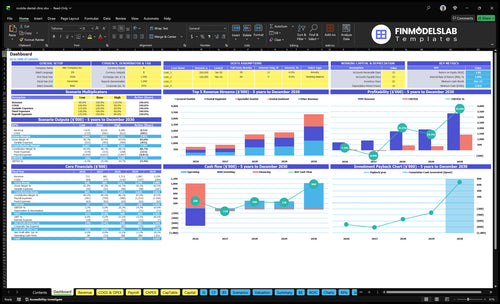
The dashboard shows revenue, margin, costs, reserves, and owner take-home assumptions in the Mobile Dental Clinic Financial Model Template; open it.
Owner-income model highlights
- Owner take-home output
- Revenue and margin view
- Scenario testing inputs
Does a mobile dental clinic owner make more as the dentist?
Yes, Mobile Dental Clinic usually keeps more cash when the owner is also the dentist, because the owner salary is already in payroll at $180,000. But that labor is not free; hiring a dentist adds about $150,000 per FTE and a hygienist adds about $80,000 per FTE, so coverage gets better and payroll gets bigger. Multi-route scale can lift profit, but it needs more providers, assistants, admin support, vehicle control, and schedule management; the fifth-year revenue figure given is $3339 million.
Owner-dentist case
- $180,000 stays in payroll
- Preserves cash inside the business
- Owner labor still has real value
- Best when routes are tight
Hired-clinician case
- General dentist pay: $150,000 per FTE
- Hygienist pay: $80,000 per FTE
- More coverage, but higher payroll
- Scale needs tighter scheduling
What affects mobile dental clinic profit margin?
Mobile Dental Clinic profit margin rises or falls on clinical labor, provider utilization, and service mix, then on vehicle costs, supplies, lab fees, insurance, billing, and uncollected claims. In the model, first-year operating margin is 193% after owner salary, with variable costs at 150% of revenue and fixed overhead at $5,250/month; see What Is The Estimated Cost To Open And Launch Your Mobile Dental Clinic Business? for the launch-cost side. By year five, variable costs fall to 125% as utilization rises, so the biggest win is keeping the mobile schedule full.
Margin drivers
- Clinical labor is the top driver.
- Provider utilization lifts margin fast.
- Service mix changes gross profit.
- Uncollected claims cut cash margin.
Cost stack
- Variable costs total 150% of revenue.
- 60% is supplies.
- 30% is lab fees.
- $5,250/month is fixed overhead.
How much can a mobile dental clinic owner take home after expenses?
A Mobile Dental Clinic owner can model $180,000 in first-year salary, plus up to $137,472 in operating profit before taxes, debt service, reserves, and distributions; What Is The Most Important Indicator Of Success For Mobile Dental Clinic? matters because $712,320 revenue is not owner income. Here’s the quick math: after $405,000 payroll, $63,000 fixed overhead, and variable costs, profit is the cash pool to split carefully.
Owner Pay
- Set salary at $180,000
- Treat revenue as business inflow
- Distribute profit only after obligations
- Keep cash for reserves
Expense Load
- Payroll runs $405,000
- Fixed overhead totals $63,000
- Supplies and lab fees apply
- Vehicle and insurance fees add friction
What really drives mobile dental clinic owner income?
1
304-1,338/moBooked Visits
More visits spread the mobile unit and fixed team cost across more billable slots, so before-tax owner take-home rises fastest.
2
$120-$500Service Mix
Mixing hygiene, general, and specialist care lifts revenue per visit, and a richer mix feeds EBITDA faster.
3
2.0%-1.5%Payer Collections
Insurance processing fees falling from 2.0% to 1.5% keep more billed cash, so less revenue leaks out before take-home.
4
60%-90%Route Utilization
Higher capacity use turns drive time into billable time and cuts the cost of empty miles.
5
$405K-$1.0MStaffing Model
Payroll is the biggest swing cost, so matching FTE to demand protects margin as the clinic scales.
6
$63K/yrOverhead Control
Keeping rent, software, permits, and insurance tight protects cash because fixed overhead hits take-home every month.
Mobile Dental Clinic Core Six Income Drivers
Booked Visits And Appointment Utilization
Booked Visits And Utilization
Booked visits only help income when they turn into completed visits. In year one, effective monthly visits are 304; by year five, they rise to 1,338, or about 4.4x. More filled slots spread fixed costs across more revenue, but cancellations, no-shows, travel time, and setup time cut collected income fast.
Think in completed visits, not booked visits. A full school, employer, or senior site schedule can raise revenue without another vehicle, but route gaps leave chair time idle and push owner pay down.
Track Fill Rate and Kept Visits
Measure the chain from capacity to booked appointments to completed visits. Use capacity, booked appointments, completed visits, cancellations, no-shows, chair time, setup time, and travel time. Fill rate means the share of capacity that turns into completed visits, and that is what raises margin and cash for the owner.
- Booked vs. completed visits
- No-shows by site type
- Travel time per route
- Chair time per visit
If a site blocks a full day but fills only part of it, the model looks busy and still under-collects. Tight route planning and reminder calls protect revenue because unused time is the real cost here.
1
Payer Mix And Collections
Collections Drive Owner Pay
Collected revenue is what pays the owner, not billed charges. In year one, the model uses collected treatment prices of $120, $200, and $500, so payer mix changes cash fast. Private pay, employer contracts, and cleaner collections lift income; slower Medicaid, insurance, and nonprofit payments can cut cash even when visits look strong.
Here’s the quick math: the same visit volume can create very different owner pay if claims sit in accounts receivable (money owed later). A full schedule still feels weak if denials, underpayment, or late remits delay cash before payroll. High billed production is not the same as strong take-home income.
Track Cash by Payer Type
Build the forecast by private pay, Medicaid, insurance, employer contracts, school programs, senior care sites, and nonprofit partnerships. Track collected amount, days to collect, denial rate, and write-offs for each bucket. That shows whether each completed visit is really funding owner pay or just creating unpaid receivables.
- Separate billed from collected.
- Watch weekly cash receipts.
- Rebill denials fast.
- Hold draws until cash clears.
A $500 billed service that pays late can still strain payroll and overhead. If reimbursement is lower than expected, or claims take longer to settle, reduce spending fast and update the cash forecast before the month-end draw.
2
Service Mix And Revenue Per Visit
Service Mix and Revenue per Visit
When more completed visits shift from hygiene to general or specialist care, collected revenue per visit rises fast. In year one, the model uses $120 for hygienist visits, $200 for general dentist visits, and $500 for specialist visits, for a blended average of about $195 per completed visit. That average drives cash available for payroll, travel, supplies, and owner pay.
The mix matters as much as volume. A heavy share of cleanings and exams keeps revenue lower, while more simple restorations, extractions, X-rays, sealants, and fluoride pushes ticket size up. But scope and licensing limits can cap in-vehicle care, so some higher-value cases become referrals instead of revenue. Fifth-year pricing rises to $130, $220, and $550, which helps margins if collections keep pace.
Track Visit Mix, Not Just Visit Count
Here’s the quick math: if completed visits stay flat, a better service mix lifts collected revenue without adding more drive time. Track completed visits by service line, collected dollars per visit, and referral rate. One clean rule: higher-value care should fill the schedule only when setup time and clinician scope still leave room for profit.
- Split visits by procedure type.
- Watch collected revenue per visit.
- Measure referral leakage by site.
- Price simple add-ons separately.
- Match scope to clinician licenses.
If most demand is hygiene, plan around the $120 base. If employer, senior, or family sites support more general dentistry, the blended average can move closer to $195 or higher. What this hides: a richer mix can also mean longer chair time and more supply cost, so the owner still has to protect margin, not just gross revenue.
3
Route Efficiency And Productive Clinic Days
Route Density Sets Billable Capacity
When travel time replaces chair time, the mobile unit earns less per day. In this model, capacity rises from 600% to 850% for the general dentist, 700% to 900% for the hygienist, and 500% to 750% for the specialist dentist, so route quality directly lifts collected revenue before you hire more staff.
Here’s the quick math: more productive operating days, shorter drive time, faster setup, better parking access, and denser sites mean more completed visits per route. What this estimate hides is lost time from weather and maintenance downtime, which can cut chair time fast. If route gaps grow, owner pay drops even when booked demand looks strong.
Track Minutes, Not Just Visits
Measure drive time, setup time, site density, weather delays, and maintenance downtime by location. A route with fewer miles but more waiting can still hurt income. Use completed visits per productive day as the main score, because that shows whether the vehicle is making money or just moving around.
Vehicle operating costs start at 40% of revenue and fall to 35% as routing improves, so every $100 collected keeps about $60 to $65 before fixed overhead. Push full-day site blocks, group nearby locations, and avoid thin routes. Better routing raises income without adding another vehicle.
4
Staffing Model And Provider Compensation
Staffing and Provider Pay
Payroll is the biggest cash pull in this model. Year one payroll is $405,000: $180,000 owner salary, $75,000 general dentist coverage, $80,000 hygienist, $45,000 dental assistant, and $25,000 admin coordinator. That is about $33,750 per month before taxes or overtime, so underused staff can cut owner pay fast. Unfilled labor is expensive.
Track Utilization Before You Hire
Track payroll as a share of collected revenue by role, not just total headcount. Build the forecast from owner salary, clinician pay, assistant hours, and admin coverage, then compare it with booked visits and collections each month. If the owner covers more chair time, cash flow can improve, but the schedule gets tighter and burnout risk rises.
Hire support staff only when they protect paid chair time. Assistants, drivers, billing staff, and admin staff help clinicians stay productive, but each hire raises the volume needed to pay everyone. Test one change at a time and watch utilization, no-shows, and revenue per visit before locking in more payroll.
5
Vehicle, Equipment, Compliance, And Overhead Control
Overhead Sets Owner Pay
Here’s the quick math: fixed overhead is $5,250/month, or $63,000/year, before vehicle operating costs and processing fees. The biggest lines are $1,500 office base rent and $2,050 in insurance and permits. That means take-home income only improves when collected revenue stays well above these recurring costs.
This driver also depends on cash reserves for maintenance, sterilization, imaging, compressors, permits, software, and supply swings. If the vehicle is down, revenue can stop while overhead keeps running. A mobile dental clinic needs enough cash to cover those gaps without cutting owner pay first.
Track Fixed Cost Per Month
Measure fixed overhead, variable overhead, and collected revenue separately. Track office rent, insurance, accounting, software, and utilities as a share of cash collected, not billed work. If processing fees or vehicle costs climb, route density and pricing need to cover them, or the owner’s draw gets squeezed.
- Fixed overhead: $5,250/month
- Office base rent: $1,500
- Vehicle insurance and permits: $1,000
- Professional liability insurance: $800
- Accounting and legal: $750
- EHR and billing software: $500
Set a reserve plan for repairs and supply spikes before they happen. If a site schedule adds more drive time than visits, overhead per treatment rises fast. The fix is simple: keep the route full, keep downtime low, and hold enough cash to survive a bad month without touching payroll or owner pay.
6
Compare lean, base, and high-utilization owner income cases
Owner income scenarios
Owner income changes with visit volume, provider use, and payroll load. This table compares a lean ramp, a base case, and a high-utilization case.
| Scenario | Low CaseEarly ramp | Base CaseScaled team | High CaseMulti-provider |
|---|---|---|---|
| Launch model | This is the lower owner-income path built on early ramp volume and one mobile unit. | This is the modeled mid-case as visits, staffing, and pricing scale steadily. | This is the stronger income path when multi-provider use pushes the unit close to full capacity. |
| Typical setup | It assumes 304 monthly visits, $59,360 monthly revenue, $712,320 annual revenue, and $405,000 payroll, with the owner taking $180,000 salary and limited profit upside. | It assumes 760 monthly visits, $142,749 monthly revenue, about $1.713 million annual revenue, and $727,500 payroll before reserves. | It assumes 1,338 monthly visits, $278,250 monthly revenue, about $3.339 million annual revenue, and $1,000,000 payroll before reserves. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $180,000 - $317,472Early ramp | Up to $863,883Scaled team | Up to $2,039,000Multi-provider |
| Best fit | Use this to stress-test a cautious launch and lower route density. | Use this for the expected staffing and utilization path. | Use this to test upside if the clinic runs at high density across multiple providers. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Mobile Dental Clinic Porter's Five Forces Analysis
- Mobile Dental Clinic BCG Matrix
- Mobile Dental Clinic Business Model Canvas
- Tracking Key Performance Indicators for a Mobile Dental Clinic
- Mobile Dental Clinic Business Plan Template in Pre-Written Word
- Increase Mobile Dental Clinic Profitability in 7 Essential Strategies
- Analyzing the Monthly Running Costs for a Mobile Dental Clinic
- Mobile Dental Clinic Startup Costs: $640K+ Before Runway
- Mobile Dental Clinic Financial Model Template in Excel
- How To Open A Mobile Dental Clinic In 3-9 Months With First Routes
- How to Write a Mobile Dental Clinic Business Plan
- Mobile Dental Clinic Marketing Mix
- Mobile Dental Clinic Marketing Plan
- Mobile Dental Clinic Business Proposal
- Mobile Dental Clinic PESTEL Analysis
- Mobile Dental Clinic Pitch Deck Example Editable PPTX
- Mobile Dental Clinic Business SWOT Analysis
- Mobile Dental Clinic Value Proposition Canvas
Frequently Asked Questions
In the first-year model, the clinic keeps $137,472 in operating profit after a $180,000 owner salary, $405,000 payroll, and $63,000 fixed overhead That equals a 193% margin before taxes, debt service, reserves, and reinvestment Owner cash depends on how much profit is actually distributed