Mobile Medical Unit Startup Costs: $890K+ First-Year Plan

This mobile medical unit cost breakdown covers vehicle CAPEX, clinical buildout, diagnostic equipment, technology, compliance, launch payroll, supplies, and working capital The researched first-year model includes at least $890,000 of known startup CAPEX for 3 units, plus about $116,550 per month in payroll and fixed overhead during the opening month and early ramp-up period These are planning assumptions, not vendor quotes, and total funding need is higher than the vehicle budget alone
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a mobile medical unit, before contingency.
What this excludes This calculator covers capitalized startup assets only. It excludes initial medical inventory, payroll runway, deposits, debt service, working capital, and other post-launch operating costs.
What should the CAPEX tab show?
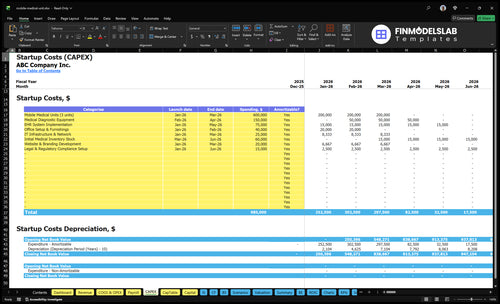
Open the Mobile Medical Unit Financial Model Template CAPEX tab to check startup costs, Month 1-5 timing, depreciation, amortization, and cash runway. Review the source schedule and adjust assumptions.
Financial model screenshot highlights
- Month 1-5 CAPEX schedule
- $890k+ total spend
- $600k vehicle units
- $150k diagnostic equipment
- $75k EHR setup
- $65k office IT
- Reimbursement assumptions
- Staffing and revenue ramp
- $153M Year 1 revenue
- $116,550 monthly fixed costs
How should mobile medical unit business plan funding be modeled?
Model the funding ask as a Month 1 to Month 5 CAPEX build plus enough working capital to cover the gap before reimbursement cash comes in. For the Mobile Medical Unit, tie the raise to units, equipment, EHR, office, and IT, then show Year 1 staffing and a revenue run-rate of about $127,300 per month.
Use of funds
- Month 1–2: units and core equipment
- Month 3: EHR and IT setup
- Month 4: office buildout and admin tools
- Month 5: launch cash and reserve funding
Year 1 model
- Staffing: 2 doctors, 2 nurse practitioners
- Staffing: 3 medical assistants, 2 phlebotomists
- Staffing: 3 driver EMTs, 1 ops manager, 1 billing admin, 1 CEO
- Revenue: treatments × price × capacity = about $127,300/month
How much money do you need to start a mobile medical unit?
You need about $1,239,650 to start a Mobile Medical Unit: $890,000 in known CAPEX plus a 3-month working-capital cushion of $349,650. That’s the practical floor before unpriced inventory, deposits, financing costs, and launch losses; track it against What Is The Most Important Indicator Of Success For Mobile Medical Unit? so spend ties to patient volume.
Known CAPEX
- 3 units: $600,000
- Diagnostic equipment: $150,000
- EHR implementation: $75,000
- Office setup and IT: $65,000
Cash Cushion
- Monthly overhead: $116,550
- 3-month cushion: $349,650
- Practical start: $1,239,650
- Still excludes: inventory, deposits, financing, losses
How much does mobile clinic vehicle conversion cost?
A Mobile Medical Unit usually prices from the base vehicle, the conversion, and the installed medical equipment. One bundled model priced 3 units at $600,000, or $200,000 per unit, before you split out line items. The real cost drivers are layout, power, plumbing, HVAC, accessibility, cabinetry, infection-control surfaces, equipment capacity, and route durability, and the care model matters too: primary care, screenings, vaccines, occupational health, or outreach.
Cost drivers
- Separate vehicle, conversion, equipment.
- Layout changes labor and materials.
- HVAC and power raise spend.
- Plumbing and surfaces add cost.
Scope check
- Van, RV, bus, trailer, or specialty vehicle.
- Primary care needs different build-outs.
- Screenings and vaccines need less space.
- Route durability affects long-run cost.
Calculate Fuding Needs
Startup cost summary
This table breaks out the main launch costs for a mobile clinic vehicle, equipment, systems, and opening cash needs.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| Mobile Medical Units (3 units) | $600,000 | Vehicle buildout for three clinic units | Yes |
| Medical Diagnostic Equipment | $150,000 | Clinic-grade diagnostics and medical gear | Yes |
| EHR System Implementation | $75,000 | Patient record and billing setup | Yes |
| Office Setup & Furnishings | $40,000 | Office space, furnishing, and setup | Yes |
| IT Infrastructure & Network | $25,000 | Network, devices, and connectivity | Yes |
| Opening Cash Buffer | $393,000 | Month 1 fixed costs and Year 1 payroll runway; excludes debt service and ongoing losses | No |
Mobile Medical Unit Core Five Startup Costs
Vehicle Purchase Or Lease Startup Expense
Vehicle Budget
The source model sets $600,000 for 3 mobile medical units in Months 1 to 3, or a planning average of $200,000 per unit. This is the base vehicle cost only, so it should sit apart from conversion and medical equipment in the startup budget.
Cost Drivers
Price swings come from new versus used, mileage, size, accessibility, power needs, water systems, refrigeration, service routes, and whether the unit is a van, RV, bus, trailer, or specialty medical vehicle. Ask vendors to split chassis price, retrofit labor, and installed systems so the vehicle line stays clean.
- Use one quote per unit.
- Separate chassis and retrofit.
- Match vehicle to route needs.
Control Spend
Keep the vehicle spec tight: buy only the size and power setup the route needs, because extra length, lift access, refrigeration, or water capacity raises the check fast. A clean comparison of 3 units by mileage, age, and equipment package helps avoid paying for features that do not change patient care.
- Standardize the fleet spec.
- Price used units carefully.
- Skip unused luxury options.
Budget Fit
Plan this line as a first-wave cash need, since the model places the $600,000 outlay in Months 1 to 3. If you track it separately from conversion and equipment, you can see the real vehicle spend per unit and keep the launch budget from hiding cost creep.
Clinical Buildout And Vehicle Conversion Startup Expense
Buildout Scope
Clinical conversion is CAPEX, not repairs or payroll. It covers exam-room layout, cabinetry, flooring, HVAC, electrical, generator or battery system, plumbing, sink, lighting, accessibility, and infection-control surfaces. The source model folds this into the $600,000 mobile-unit line for 3 units, so ask vendors to split the chassis, retrofit labor, installed systems, and medical-ready finishes.
Quote It Cleanly
Price the conversion by scope, not as one lump sum. Use unit count, design spec, and vendor quotes for each system so you can compare bids on the same basis. Here’s the quick rule: if the quote does not separate buildout from the vehicle, you cannot tell what you are really buying.
- Split labor from materials
- Price power and plumbing separately
- Check accessibility in writing
Keep It Capital
Put the conversion on the startup balance sheet, alongside the vehicle, because it creates long-lived value. That avoids mixing one-time build costs with operating expenses. If a vendor calls part of it “maintenance,” push back and ask for the exact line items; otherwise, your startup budget will understate true launch cash needs.
Vendor Split
Ask every bidder to show base chassis, retrofit labor, installed systems, and medical-ready finishes as separate lines. That makes the $600,000 fleet number readable, and it helps you see whether one unit is a van, RV, bus, trailer, or specialty medical vehicle before you commit cash.
Medical Equipment And Diagnostic Devices Startup Expense
Clinic Kit
The mobile clinic equipment budget is $150,000 from Month 2 to Month 4, or about $50,000 per unit across 3 units. It should cover exam tables, vital signs gear, point-of-care testing, refrigeration, sterilization supplies, sharps handling, and service-specific devices for primary care, screenings, vaccinations, occupational health, phlebotomy, and outreach.
Budget Inputs
Start with 3 units × $50,000, then add vendor quotes for each device. Split the list by use case: primary care, screenings, vaccines, and phlebotomy. Count months of coverage for sterilization and sharps supplies, since those move with visit volume. This line sits inside total vehicle and conversion spend.
Control Spend
Keep the kit lean by matching equipment depth to the service mix. A screening-heavy route needs less than a phlebotomy-heavy route, so buy to the first 90 days of demand and compare at least 2 quotes per high-cost item. Avoid duplicate devices and idle inventory; that ties up cash fast.
Route Fit
Primary care and vaccine routes need exam tables, vitals gear, refrigeration, and point-of-care testing. Occupational health or community outreach can add service-specific devices. If one service drives most visits, put more of the $150,000 there first. One-size-fits-all kits waste cash.
Licensing Compliance And Insurance Startup Expense
License Stack
Mobile clinic licensing and insurance stack up fast because you need state healthcare rules, vehicle registration, malpractice, general liability, auto and fleet coverage, and sometimes CLIA if testing is done. The source model starts Fleet Insurance & Licensing at $4,000/month plus General Liability Insurance at $800/month, or $4,800/month from Month 1.
Cost Inputs
Estimate it with quotes × vehicles × months, then add any state filing fees, testing rules, and medical waste handling costs. Ask vendors to split legal setup, insurance, and compliance consulting so you can see what is one-time and what repeats each month.
- Count each unit separately.
- Price each state served.
- Check CLIA before testing.
Control Risk
Keep the policy mix lean, but don’t underbuy. The real risk is paying for the wrong scope, like skipping fleet coverage for a mobile unit or missing waste rules in a state where you operate. Verify rates and filing needs locally before launch, since they change by state, county, and service type.
Verify Locally
Ask for written quotes on malpractice, general liability, auto, and fleet coverage, then check state healthcare rules and medical waste handling before you buy. If you plan any lab work, confirm CLIA needs first, because testing can change both the license path and the monthly insurance load.
Technology Supplies And Launch Readiness Startup Expense
Launch tech stack
The tech budget splits into setup and monthly run-rate. Plan $75,000 for EHR implementation over Months 1 to 5, plus $25,000 for IT infrastructure over Months 1 to 3, then add the $1,500 monthly EHR and scheduling fee starting in Month 1. This covers records, scheduling, and connectivity, not clinical gear.
Set the base
Use vendor quotes, unit counts, and rollout months to price the stack. Separate one-time setup from recurring fees. The variable EHR and billing fee is 3% of Year 1 revenue, so the dollar cost rises with visit volume even when the rate stays flat.
Model supplies
Mobile medical unit supplies are usage based, so budget from expected treatments, test mix, and refill cadence. Plan 7% of revenue for supplies and pharmaceuticals, plus 3% of revenue for lab fees. Every extra patient visit pushes replenishment higher, so volume and service mix matter.
Keep it lean
Buy only the devices your service plan needs, then add more later. The common mistake is mixing setup with monthly spend, which hides real burn. If rollout slips past 5 months, the EHR build keeps drainin g cash longer, so lock scope, timeline, and vendor deliverables early.
Compare 3 Startup Cost Scenarios
Scenario table
Lean cuts vehicles and equipment, the base case funds a three-unit primary-care clinic, and the full build adds specialty gear, redundancy, and more cash reserve.
| Scenario | Lean LaunchScreening unit | Base LaunchPrimary care | Full LaunchSpecialty build |
|---|---|---|---|
| Launch model | Run one lighter vehicle with a narrow service line and slower staffing ramp. | Run the source base case with three units and full primary-care coverage. | Run a larger, multi-room unit with more service depth and higher uptime needs. |
| Typical setup | Use basic exam gear, lean tech, and lower on-hand inventory. | Use core diagnostics, standard clinic tools, and staffing sized to the model's base case. | Add specialty equipment, refrigeration, power redundancy, stronger tech, and extra cash reserve. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | $400,000 - $900,000Lower funding | $1,000,000 - $2,000,000Core build | $2,000,000 - $3,500,000Higher funding |
| Best fit | Best for a narrow outreach or screening start where speed matters more than breadth. | Best for founders launching a standard mobile clinic with broader patient coverage and room to scale. | Best for operators building a fuller service mix where reliability and clinical depth matter most. |
Planning note: These scenario ranges are researched planning assumptions, not exact vendor quotes or final budget numbers.
Related Products
- Mobile Medical Unit Porter's Five Forces Analysis
- Mobile Medical Unit BCG Matrix
- Mobile Medical Unit Business Model Canvas
- Tracking 7 Core KPIs for Mobile Medical Unit Success
- Mobile Medical Unit Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Mobile Medical Unit Profitability Fast
- Running Costs: How to Operate a Mobile Medical Unit Sustainably
- Mobile Medical Unit Financial Model Template in Excel
- How Much Mobile Medical Unit Owners Make: $154K First Year
- How To Open A Mobile Medical Unit In 4–9 Months With Routes
- Writing the Mobile Medical Unit Business Plan: 7 Actionable Steps
- Mobile Medical Unit Marketing Mix
- Mobile Medical Unit Marketing Plan
- Mobile Medical Unit Business Proposal
- Mobile Medical Unit PESTEL Analysis
- Mobile Medical Unit Pitch Deck Example Editable PPTX
- Mobile Medical Unit Business SWOT Analysis
- Mobile Medical Unit Value Proposition Canvas
Frequently Asked Questions
Carry enough to cover payroll, fixed overhead, and slow reimbursement during ramp-up In this model, payroll is about $103,750 per month and fixed overhead is $12,800 per month, so a 3-month cushion is about $349,650 before variable costs That reserve sits on top of the known $890,000 CAPEX plan