 Time to Open3-6 monthsSetup window
Time to Open3-6 monthsSetup windowHow to Open a Mobile Urgent Care Clinic in 3 to 6 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open3-6 monthsSetup window  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckLicense gateState rules
Key BottleneckLicense gateState rules First Revenue StepPaid visitsBooking live
First Revenue StepPaid visitsBooking live


You’re launching a field-based urgent care service, so the work is about clinical permission, provider coverage, safe kits, systems, and booked visits before the first patient call Plan on 3 to 6 months, with the first-year model using 3 general practitioners, 1 pediatric specialist, 1 geriatric specialist, 1 diagnostic tech, and 1 mental health pro at 60% capacity Use the financial model to test visit volume, staffing coverage, and cash runway, but keep launch execution first
Time to Open3-6 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepPaid visitsBooking liveMobile urgent care launch timeline
This is a short web summary of the launch plan, and the XLSX export carries the detailed Gantt chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11
Compliance
- Entity filing
- State licenses
- Malpractice cover
- HIPAA workflows
Clinical protocols
- Scope of care
- Triage rules
- Treatment protocols
- Escalation plan
- Chart templates
Fleet & equipment
- Vehicle quotes
- Fleet upfit
- Kit buildout
- Sanitation plan
- Restock system
Systems & billing
- EHR setup
- Booking flow
- Routing map
- Billing flow
- Secure messaging
Staffing
- Recruit GPs
- Recruit specialists
- Credential checks
- Hire coordinator
- Train team
Demand & partners
- Partner vendors
- Local search
- Employer outreach
- Senior living
- Soft launch
Want to test launch timing before you hire?
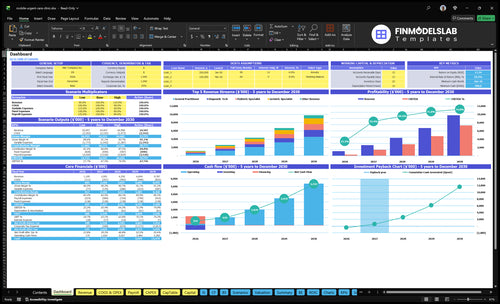
This screenshot shows revenue, costs, cash needs, assumptions, and break-even logic. Open the Mobile Urgent Care Financial Model Template to test launch assumptions first.
Model highlights
- Launch timing and staffing
- Visit ramp by month
- Pricing mix and costs
- Cash runway and break-even
Do you need a license to start a mobile urgent care clinic?
Yes, Mobile Urgent Care needs licensing before the first patient visit, but the exact rules vary across the 50 U.S. states; start with state medical practice rules, provider licenses, malpractice coverage, HIPAA workflows, and prescribing limits. The bottleneck is simple: don’t launch marketing until compliance is cleared; for market context, see What Is The Current Growth Trend Of Mobile Urgent Care?.
Licenses to verify
- Check state medical practice rules first
- Confirm physician, NP, and PA licensure
- Verify diagnostic and mental health staff rules
- Clear medical director and supervision requirements
Opening controls
- Set malpractice insurance before opening
- Build HIPAA intake, records, billing workflows
- Define prescribing and documentation standards
- Set emergency escalation before visit 1
What mobile urgent care launch mistakes create the most risk?
The biggest launch mistakes in Mobile Urgent Care are weak triage, unclear scope of care, no emergency referral path, and opening before the EHR, billing, and routing workflow are live. That creates bad patient flow, missing documentation, and supply gaps. Here’s the quick math: if Year 1 runs at 60% capacity with a 17% variable cost load and $8,500 in monthly fixed expenses, a slow start can squeeze cash fast.
Top launch risks
- Weak triage sends wrong cases.
- Unclear scope causes care drift.
- No ER referral path raises risk.
- Understocked supplies slow visits.
Readiness checks
- Confirm EHR and billing work.
- Test lab, pharmacy, waste flow.
- Lock provider schedules before open.
- Soft launch with full review.
How do you get patients for a mobile urgent care clinic?
If you want patients for Mobile Urgent Care, start with booked visits, not broad awareness. The first leads usually come from local SEO, a Google Business Profile, and paid search for “urgent care near me”; for launch planning, see How Much Does It Cost To Open, Start, And Launch Your Mobile Urgent Care Business? Publish your service area, hours, visit types, pricing, and no-go emergencies on day one, then push self-pay visits, employer visits, and concierge urgent care calls first.
Patient sources
- Local SEO brings nearby searches
- Google Business Profile drives calls
- Paid search catches urgent care intent
- Senior living and hotels can refer
First revenue moves
- Sell $200 general practitioner visits
- Price pediatric and geriatric at $220
- Charge $150 for diagnostic visits
- Track conversion by zip and provider capacity
Confirm the clinic can safely treat patients on day one
Launch readiness checklist
Use this go-live approval checklist before opening a mobile urgent care service.
Compliance gate
- Entity formation completeCritical
You need the entity in place before permits, banking, and contracts can move.
- Licenses and permits confirmedCritical
Operating licenses and local permits should be cleared before the first visit.
- State practice rules reviewedCritical
State medical rules set what this service can and cannot do on the road.
- Medical director oversight setHigh
If oversight is required, the launch stalls without a signed clinical lead.
Clinical scope
- Scope and exclusions approvedCritical
Clear no-go cases keep staff from treating beyond the model or license.
- Triage protocol signedCritical
Triage decides who gets a visit, a referral, or a higher level of care.
- Emergency escalation path setHigh
A named escalation path matters if a case turns urgent during a visit.
Mobile clinic
- Vehicles inspected and outfittedCritical
The fleet must support safe travel, storage, and patient care before go-live.
- Medical kits and PPE stockedCritical
Teams need kits and protective gear on day one to treat and protect.
- Supply vendors confirmedHigh
Supplies, labs, pharmacy, and imaging links need named vendors before launch.
- Sanitation and waste pickup activeHigh
Cleanup and medical waste handling must work before the first house call.
Systems live
- EHR configured and testedCritical
Records must capture visits, notes, orders, and billing from the first patient.
- Scheduling and messaging liveCritical
Patients need a working booking path and visit updates before launch.
- HIPAA and payment workflows verifiedCritical
Patients need protected intake, payment, and records flow before the first visit.
Staffing
- Year 1 provider roster setCritical
Year 1 needs the planned mix of 7 providers to cover demand.
- Shift coverage mappedCritical
Coverage has to match the 60% capacity plan and avoid missed visits.
- Training and drills completeHigh
Staff need practice with protocols, tools, and escalation before opening.
Launch economics
- Pricing band approvedCritical
Launch pricing should sit in the $150 to $250 range from the model.
- Revenue channels readyHigh
Self-pay, employer, senior living, and referral paths need to be active.
- Cash runway clearedCritical
The model hits minimum cash of $490k in Month 6, so launch needs that buffer.
- Go-live approval signedCritical
Final signoff should confirm compliance, coverage, systems, and cash.
What actually determines whether this clinic opens well?
1Compliance
3-6 moWritten approval, insured providers, and secure records let you treat patients without shutdown risk.
2Staffing
60% startYear 1 coverage starts at 60%, and 7 clinicians keep patient demand from outpacing license checks.
3Equipment
10% loadA stocked, checked kit before each shift cuts repeat trips and missed care.
4EHR Billing
$3K/moLive booking, documentation, and payment flows reduce missed visits and speed cash collection.
5Vendor Network
Payer lagSigned lab, imaging, pharmacy, and referral workflows keep visits from stalling after intake.
6Patient Pipeline
$150-$250Booked demand at $150-$250 per visit turns fixed overhead into first revenue.
Regulatory And Clinical Compliance
Clinical Compliance Gate
Mobile urgent care cannot treat patients until the legal and clinical setup is cleared. That means confirming state medical practice rules, the right entity structure, provider licenses, supervision or medical director rules, prescribing rules, malpractice coverage, HIPAA workflows, and charting standards. If any piece is missing, opening slips because you do not have permission to operate safely on day one.
The main risk is assuming a mobile model follows the same rules as a fixed clinic. It often does not. You also need a clear escalation path for symptoms outside scope, so staff know when to stop care and send the patient to emergency services. The readiness signal is simple: written approval path, insured providers, signed protocols, and secure record handling.
Lock the approval path first
Start with the rules that control who can treat, prescribe, and supervise. Then map the exact documents needed before launch: licenses, malpractice proof, supervision or medical director sign-off, HIPAA forms, consent language, documentation templates, and an emergency referral rule. One clean one-liner: no paperwork, no patient visit.
Use a go-live checklist and test it with a mock visit. The check should move from intake to note entry to secure storage without gaps. If any step still needs manual work, fix it before opening. That protects first-day service, keeps staff from guessing, and lowers the risk of a shutdown caused by a missed compliance step.
1
Provider Staffing And Medical Oversight
Licensed Coverage
Provider staffing and medical oversight decide whether the service can open on time and serve patients on day one. The Year 1 plan needs 3 general practitioners, 1 pediatric specialist, 1 geriatric specialist, 1 diagnostic tech, and 1 mental health pro. That mix sets scope, shift coverage, and patient experience, and it also defines how much demand you can safely take. Capacity starts at 60% and rises to 85% by Year 5.
The launch risk is simple: booking demand can outrun licensed coverage. If license checks, medical director oversight, or supervision rules are not locked in early, you get delays, reschedules, and weaker first-day service. The readiness signal is covered service hours with backup clinicians, not just a full hiring plan on paper.
Cover Every Shift
Before opening, verify each clinician’s license status, scope, supervision path, and backup coverage. If a medical director is required, assign that oversight early and document who approves protocols, escalations, and shift coverage. One clean rule helps: every patient-facing hour should have a named licensed clinician and a backup.
Also map intake support to the clinical schedule. Intake has to route patients to the right clinician type, and it has to do it without overbooking the team. Here’s the quick test: can you fill a normal day with the planned mix of providers and still absorb a call-out without canceling visits?
- Check licenses before scheduling.
- Document supervision and escalation steps.
- Assign backup clinicians by shift.
- Match intake volume to covered hours.
2
Vehicle Equipment And Supply Readiness
Mobile Kit Readiness
For mobile urgent care, the vehicle has to carry the approved scope of care on day one. That means exam kits, basic diagnostics, PPE, wound care supplies, medications within scope, and refrigeration if needed, plus secure storage, sanitation, and vehicle branding. If the kit is incomplete, the visit can stall, miss care, or turn into a repeat trip.
The money side is clear: Year 1 direct cost assumptions include 7% of revenue for medical supplies and pharmaceuticals and 3% for diagnostic lab fees, so 10% of revenue is tied to this readiness lane before fuel, labor, or vehicle costs. One missing item can delay launch or break the first-day schedule.
Pre-Shift Checks
Before opening, lock the workflow around a stocked, checked, and documented kit before each shift. That means assign one owner for counts, restocking, and cold-chain checks, then test the full loop: load, verify, document, and refill. If the team cannot prove the kit is ready, the launch is not ready.
- Match supplies to approved scope.
- Count inventory before every shift.
- Log restocks and shortages.
- Check refrigeration and storage.
Here’s the quick risk: weak supply control leads to missed treatment, slower visits, and extra labor from second trips. Build the checklist before the first patient, because a clean handoff between supply, vehicle, and clinician is what keeps same-day service real.
3
Scheduling EHR Billing Infrastructure
Live Scheduling and Billing Stack
If the booking, intake, routing, documentation, payment, and claims flow is not live before day one, the service opens with manual gaps. That creates missed visits, slow collections, and more staff time spent fixing records instead of treating patients. The system needs to support online booking, intake forms, triage questions, route scheduling, documentation, e-prescribing if in scope, payment collection, claims or superbills, messaging, and HIPAA-secure communication.
The modeled technology license is $3,000 per month from Month 1 through Month 60, so this is a fixed launch cost, not a later add-on. The readiness test is simple: one test visit should move from booking to payment to documentation with no manual handoffs. If that fails, day-one operations will leak time and cash.
Build the Visit Flow Before Opening
Set up the stack in launch order: booking first, then intake, triage, routing, charting, and payment. The team should confirm user access, templates, consent language, and message rules before opening. One clean rule: no patient slot counts as ready until the full visit can be closed inside the system.
- Verify HIPAA-secure messaging and role access.
- Test payment, superbills, and claim export.
- Run one full mock visit end to end.
- Check e-prescribing only if in scope.
What this setup hides is the labor cost of workarounds. If staff must rekey notes, chase payments, or fix routing outside the system, first-revenue speed drops and no-show recovery gets weaker. Build the test visit around the hardest case, not the easiest one, so the opening plan matches real volume and real admin load.
4
Vendor Payer And Referral Network
Vendor and payer setup
If labs, imaging, pharmacy, waste, supplies, and billing support are not lined up, the service cannot run cleanly on day one. Mobile urgent care depends on outside handoffs, so one missing path can delay treatment, force reroutes, or keep the launch stuck in self-pay only while payer credentialing is still pending.
The real go-live signal is signed vendor workflows plus named escalation contacts. That is what proves a visit can move from intake to test order, prescription, waste disposal, and billing without guessing. The model already assumes 7% of revenue for medical supplies and pharmaceuticals and 3% for lab fees, so weak vendor terms can blow up the launch budget fast.
Lock vendor paths before launch
Build the vendor map in two buckets: operational vendors and revenue partners. Operational vendors cover labs, imaging referrals, pharmacy coordination, medical waste disposal, medical supplies, billing support, and equipment suppliers. Revenue partners cover employers, senior living facilities, occupational health buyers, concierge communities, schools, hotels, and local referral partners.
Start with the highest-risk handoffs first: lab, imaging, and pharmacy. If payer credentialing slips, plan a self-pay opening only after every vendor has a named contact, written workflow, and escalation step.
- Confirm test and result routing.
- Document pharmacy coordination steps.
- Test one visit end to end.
- Hold payer launch until credentialed.
5
Patient Acquisition And First Revenue Pipeline
Patient Pipeline Before Opening
Open only when the local demand engine is already producing booked visits. For mobile urgent care, the launch risk is simple: fixed overhead starts on day one, but revenue only starts when self-pay, employer, or concierge calls are scheduled. Year 1 visit prices of $150 to $250 need clear pricing, fast booking, and a service-area plan that shows real demand before staff and vehicles sit idle.
This driver includes local SEO, a complete Google Business Profile, “urgent care near me” search coverage, paid search, referral outreach, employer accounts, and senior community partnerships. The readiness signal is booked demand by service area and provider schedule; the failure mode is opening with overhead, a route plan, and no patient pipeline.
Pre-Launch Booking Setup
Before opening, verify that every lead path lands on a fast booking flow with clear self-pay pricing, service-area boundaries, and a same-day or next-day appointment slot. Test the full path from search to call to booking to payment so a patient can schedule without back-and-forth. One clean booking process matters more than a long marketing list.
- Publish pricing before launch.
- Match ads to service areas.
- Route calls to live booking.
- Prebook employer and senior partners.
- Fill provider schedules before day one.
Track booked visits by neighborhood, employer, and partner source, then compare them with provider coverage hours. If demand is thin in one area, do not open broad coverage there yet; open where the schedule is already filling. That keeps the first revenue stream tied to capacity you can actually serve.
6
Related Products
- Mobile Urgent Care Porter's Five Forces Analysis
- Mobile Urgent Care BCG Matrix
- Mobile Urgent Care Business Model Canvas
- 7 Critical KPIs for Mobile Urgent Care Success
- Mobile Urgent Care Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Mobile Urgent Care Profitability
- How Much Does It Cost To Run Mobile Urgent Care Each Month?
- How Much It Costs To Start A Mobile Urgent Care Clinic: $11M Plan
- Mobile Urgent Care Financial Model Template in Excel
- How Much Mobile Urgent Care Owners Make at 462+ Monthly Visits
- How to Write a Mobile Urgent Care Business Plan: 7 Actionable Steps
- Mobile Urgent Care Marketing Mix
- Mobile Urgent Care Marketing Plan
- Mobile Urgent Care Business Proposal
- Mobile Urgent Care PESTEL Analysis
- Mobile Urgent Care Pitch Deck Example Editable PPTX
- Mobile Urgent Care Business SWOT Analysis
- Mobile Urgent Care Value Proposition Canvas
Frequently Asked Questions
Start by confirming state medical practice rules, forming the right clinical entity, securing licensed providers, and defining your scope of care Then set up EHR, scheduling, billing, malpractice coverage, lab referrals, pharmacy coordination, equipment kits, and emergency escalation The researched Year 1 plan uses 7 providers at 60% capacity, with visit pricing from $150 to $250