How Much It Costs To Start A Mobile Urgent Care Clinic: $11M Plan
The cost to open a mobile urgent care clinic is about $1095 million in this researched US planning case That includes $605,000 of CAPEX, led by $250,000 for the medical vehicles fleet, $100,000 for portable diagnostic equipment, and $75,000 for EHR and scheduling setup It also includes a $490,000 working capital reserve needed by Month 6 to cover the early ramp-up period Pre-opening expense planning should also reflect $11,500 in monthly fixed overhead and about $37,700 in monthly Year 1 admin payroll once operations start
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates the startup CAPEX for a mobile urgent care launch using capitalized assets only.
!
What's excluded CAPEX only: vehicles, equipment, software setup, IT, and startup systems. It excludes inventory, payroll runway, deposits, debt service, working capital reserve, licenses, insurance premiums, marketing, fuel, and fast-turn medical supplies. The model's $490,000 minimum cash need is separate from startup CAPEX.
Calculate Fuding Needs
Startup Cost Summary
This table summarizes the main startup build-out costs and the non-CAPEX cash reserve for launching a mobile urgent care service.
Highlighted CAPEX$525,000Base planning example
Excluded cash needs$490,000Outside CAPEX total
Funding need$1,015,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Medical Vehicles Fleet
$250,000
Vehicle count and upfit level
Yes
Portable Diagnostic Equipment
$100,000
Diagnostic scope and device mix
Yes
EHR and Scheduling Platform Setup
$75,000
System setup and workflow integration
Yes
Website and Mobile App Development
$60,000
Patient booking and dispatch build
Yes
IT Infrastructure and Hardware
$40,000
Devices, network, and security hardware
Yes
Working Capital Reserve
$490,000
Month 6 fixed overhead and admin payroll runway
No
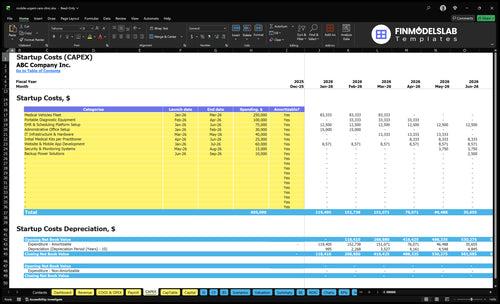
What does the CAPEX tab show?
This Mobile Urgent Care Financial Model Template screenshot shows the CAPEX tab for startup costs, timing, and depreciation or amortization. Open the model and review assumptions now.
Key screenshot highlights
Month 1 to 9 schedule
$490k Month 6 cash
$11.5k overhead, $37.7k payroll
Compare 3 Startup Cost Scenarios
Scenario table
More vehicles, broader diagnostics, and bigger staffing push startup cash up fast. Lean keeps the footprint tight, Base follows the model plan, and Full adds reserve and tech.
Lean, Base, and Full startup funding bands for mobile urgent care.
Scenario
Lean LaunchTight rollout
Base LaunchCore plan
Full LaunchWide rollout
Launch model
Start with core urgent care visits in a tight service area.
Start with 7 Year 1 clinical professionals and the sourced operating plan.
Start with broader visit types, more diagnostics, and a larger clinical bench.
Typical setup
Use fewer vehicles, a narrower service area, and a leaner support team.
Use the planned fleet, core clinic staff, and standard admin support.
Use broader diagnostics, advanced technology, and a stronger staffing bench.
Cost drivers
Fewer vehicles
smaller service area
lighter tech
lower launch reserve
Fleet capex
EHR setup
admin payroll
fixed overhead
working cash
More diagnostics
larger staff bench
advanced technology
bigger reserve
heavier payroll
Planning rangeCAPEX only
$850,000 - $1,000,000Lowest cash need
$1.09M - $1.10MFunding baseline
$1.35M - $1.60MHighest funding need
Best fit
Best for founders testing demand before a wider rollout.
Best for teams using the model as the funding case and operating target.
Best for operators aiming for wider coverage and faster build-out.
!
Planning note: These ranges are planning assumptions from the model, not exact vendor quotes or bids.
What are the hidden costs of starting a mobile urgent care clinic?
For Mobile Urgent Care, the hidden costs are not optional: payer credentialing delays, claims collection lag, malpractice coverage, commercial auto coverage, CLIA waiver or lab compliance, HIPAA policies, OSHA requirements, billing setup, staff training, fuel, maintenance, and replacement supplies all hit cash before revenue turns steady. If you want the owner-side math, see How Much Does The Owner Of Mobile Urgent Care Typically Make? and then stress-test the setup against the slow-pay cycle. The hard number to plan for is a $490,000 minimum cash need by Month 6.
Cash drain items
$1,000/month general business insurance
$1,200/month vehicle fleet insurance
30% of revenue for malpractice
40% of revenue for fuel and maintenance
Setup costs that lag cash
Payer credentialing delays slow collections
Claims collection lag ties up working capital
CLIA waiver and lab compliance add cost
HIPAA, OSHA, billing, and training stack up
How much does a mobile urgent care vehicle cost?
Mobile Urgent Care vehicle cost starts with a $250,000 vehicle fleet and buildout budget across Month 1 to Month 3. That covers buying, leasing, financing, or retrofitting the vehicle, plus clinical layout, secure storage, washable surfaces, refrigeration power, lighting, communications, safety equipment, and accessibility. Keep vehicle CAPEX separate from fuel and maintenance, which run at 40% of Year 1 revenue, and from fleet insurance at $1,200 per month.
Buildout scope
Buy, lease, finance, or retrofit the vehicle
Fit a clinical layout for patient care
Add secure storage and washable surfaces
Install refrigeration, power, lighting, and comms
Ongoing vehicle costs
Fuel and maintenance are separate
Fuel and maintenance run at 40% of Year 1 revenue
Fleet insurance is $1,200 per month
Model Month 1 to Month 3 separately
How much money do you need to start a mobile urgent care clinic?
To start Mobile Urgent Care, plan for about $1.095 million in funded capacity: $605,000 in CAPEX plus $490,000 minimum cash by Month 6. CAPEX means long-lived assets; working capital covers payroll, insurance, fixed overhead, supplies, and reimbursement timing, as explained in What Is The Current Growth Trend Of Mobile Urgent Care?. Year 1 assumes 7 clinical professionals, 600% capacity, $11,500 monthly fixed overhead, and about $37,700 monthly admin payroll, so treat this as planning capacity, not a guaranteed quote.
Funding Need
Use $1.095 million total capacity
Fund $605,000 in CAPEX
Hold $490,000 cash by Month 6
Don’t price only the vehicle
Cash Drivers
Cover $11,500 monthly fixed overhead
Budget $37,700 monthly admin payroll
Staff 7 clinical professionals
Plan around reimbursement timing
Key Takeaways
Vehicle buildout is the biggest upfront cash sink.
Medical equipment adds $125,000 before opening.
Licensing and compliance need legal review, not guesswork.
Recurring insurance and tech costs keep burning cash.
Mobile Urgent Care Core Five Startup Costs
Vehicle and Buildout Startup Expense
Fleet CAPEX
Treat this as capital spending (CAPEX): the base plan sets aside $250,000 in Month 1 to Month 3 for the medical fleet. That budget has to cover platform choice, buy vs lease, retrofit vs specialty unit, clinical layout, secure storage, sanitation surfaces, lighting, accessibility, refrigeration power, backup power tie-in, communications, and safety gear.
Budget Inputs
Estimate it from vehicle count × unit cost plus upfit quotes, then add registration and launch prep. Keep fuel and maintenance separate at 40% of Year 1 revenue, vehicle fleet insurance at $1,200 per month, and driver or practitioner payroll outside this line. That keeps CAPEX clean and easier to finance.
Cost Control
To reduce spend, compare a retrofit against a specialty medical unit and test lease terms only if you need faster launch or lower upfront cash. Don't cut lighting, secure storage, or backup power. The savings come from fitting one standard platform across the team and avoiding duplicate upfits.
Recurring Load
The recurring load is not trivial: $1,200 per month for fleet insurance, plus registration, fuel, maintenance, and driver or practitioner payroll. Keep these out of CAPEX so your startup budget doesn’t blur one-time buildout with Year 1 operating burn.
Licensing and Compliance Startup Expense
Scope first
This is a pre-opening cost, not a launch luxury. Budget for state medical business rules, entity formation, medical director setup, CLIA waiver or lab compliance, HIPAA, OSHA, payer credentialing, billing setup, clinical protocols, and controlled-access records. Don’t assume one national license covers every state; have a qualified compliance pro review each jurisdiction.
Budget inputs
Here’s the quick math: a medical director at $100,000 annual salary at 0.5 FTE is $50,000 in Year 1. Add $1,000 per month for professional services, or $12,000 over 12 months. Size this line with state count, filing quotes, review hours, and months of coverage.
Count each state filing.
Price legal review hours.
Use 12-month service quotes.
Limit rework
Keep the first launch narrow. Finish entity work before payer enrollment, write simple clinical and record rules early, and build controlled-access records before the first visit. The savings come from avoiding rework, not from skipping review. If onboarding drags or a state adds lab steps, the compliance bill goes up fast.
Start in one jurisdiction first.
Lock protocols before launch.
Track each filing deadline.
Review early
Put this cost in the budget before you sell the first visit. If the medical director plan, credentialing, or compliance review changes by state, the expense changes too, so build the model with jurisdiction-specific quotes and update it as filings move forward.
Insurance Startup Expense
Required Coverage
Before launch, budget for medical malpractice, general liability, commercial auto, workers compensation, cyber liability, property coverage for equipment, and policy deposits. The base plan already points to $1,000 per month for general business insurance and $1,200 per month for the vehicle fleet, so this is a real operating cost, not a one-time line.
Cost Build
Here’s the quick math: $1,000 a month for general coverage plus $1,200 a month for fleet coverage equals $2,200 per month, or $26,400 per year, before malpractice, cyber, and deposits. Practitioner malpractice is sized at 30% of Year 1 revenue, so the quote depends on visit volume and pricing.
One quote per policy
Annual premium and deductible
Year 1 revenue for malpractice
Keep It Clean
Get quotes early, then separate fleet, equipment, and data risk so you can see each driver clearly. Tie cyber and data risk to the $800 per month data hosting and security line. Do not bury insurance inside licensing or working capital; that hides the true launch burn and makes renewals harder to track.
Before First Visit
Insurance starts before the first patient visit and keeps running after launch. With known recurring items of $1,000, $1,200, and $800 per month, you already have $3,000 per month in coverage-related spend, before malpractice and policy deposits. That belongs in launch cash, not in licensing or working capital.
Medical Equipment and Diagnostic Startup Expense
Split the kit
Build this as reusable equipment plus consumable supplies. The sourced CAPEX is $100,000 for portable diagnostic equipment and $25,000 per practitioner for initial kits. With a Year 1 team of 7, that kit line is $175,000. Keep supplies and pharmaceuticals separate at 70% of Year 1 revenue.
What the kit covers
Size the kit with unit counts and vendor quotes for portable exam setup, vitals equipment, electrocardiogram equipment, point-of-care testing, specimen handling, emergency response items, sterilization tools, and durable clinical instruments. One clean rule: buy for the visits you can actually staff, not for a perfect clinic you do not have.
How to keep it tight
Lower spend by standardizing one base kit across all clinicians and adding only specialty tools where needed. Ask for 3 quotes, compare calibration and warranty terms, and avoid duplicate devices that sit idle. The big mistake is treating consumables like assets; they should stay in the operating budget, where they track visit volume and spoilage risk.
Budget guardrail
For this model, equipment spend should be tied to the staffed Year 1 team: 3 general practitioners, 1 pediatric specialist, 1 geriatric specialist, 1 diagnostic tech, and 1 mental health professional. If kits are not matched to that roster, launch cash gets trapped in idle gear instead of patient visits.
Technology and Staffing Setup Startup Expense
Core tech stack
Mobile urgent care needs one connected stack: EHR, scheduling, telehealth, routing, billing, and mobile connectivity. The sourced CAPEX is $75,000 for EHR and scheduling, $60,000 for website and app, $40,000 for IT hardware, and $15,000 for security and monitoring. That is $190,000 before monthly licenses.
Recurring tech load
Recurring technology runs at $3,000 per month for platform licenses plus $800 for data hosting and security. Estimate it from user count, device count, integration scope, and months of coverage. Keep records, billing, and routing live from day one, but do not pay for features the first team will not use.
Quote by active users.
Match devices to routes.
Skip unused add-ons.
Control setup cost
Lower cost by phasing rollout, not by cutting controls. Buy only the hardware and licenses needed for the first routes, then add capacity after visit volume proves out. Don’t trim security, billing setup, or onboarding. One clean rule: if a feature does not help book, treat, document, or bill a visit, delay it.
Phase features by route volume.
Delay nonessential app tools.
Protect billing and HIPAA controls.
Staffing and launch base
Staffing readiness must cover recruiting, onboarding, protocols, uniforms, and training, plus launch marketing. Year 1 admin payroll is about $37,700 per month and base marketing is $1,500 per month, so the fixed launch support is already near $39,200 before recurring tech.