 Owner income$19.6M-$106.9M
Owner income$19.6M-$106.9MHow Much Does A NICU Owner Make? $196M Year 1 EBITDA

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$19.6M-$106.9M  Net margin7.6%-8.8%
Net margin7.6%-8.8% Revenue for target pay$260M-$1.22B
Revenue for target pay$260M-$1.22B Business difficultyHard
Business difficultyHard


A NICU owner’s income is not the same as revenue or EBITDA Based on the researched assumptions provided, the business generates $260M in year 1 revenue and $196M in EBITDA, which means EBITDA margin is about 756% By year 5, revenue reaches $1221M and EBITDA reaches $1069M, but owner take-home still depends on reserves, financing, taxes, payer collections, and reinvestment Treat these as scenario-based planning outputs, not guaranteed earnings
Owner income$19.6M-$106.9MNet margin7.6%-8.8%Revenue for target pay$260M-$1.22BBusiness difficultyHardWant to test your NICU owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target owner pay.
Planning note: Research-based planning estimate only. Actual owner income depends on revenue, margin, staffing, taxes, debt, reserves, and payout policy. It is not guaranteed salary, tax advice, or owner distribution advice.
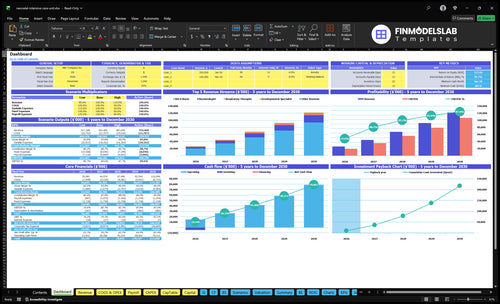
Want to check owner income in the NICU model?
The screenshot in the NICU Financial Model Template shows revenue forecast, staffing, capex, EBITDA, cash, and owner-pay sensitivity—open it.
Model tabs and outputs
- Assumptions, revenue, payroll tabs
- Capex, scenarios, output charts
- Revenue $260M to $1.221B
- EBITDA $196M to $1.069B
- Capacity, payer mix, staffing
- Reserves, debt service, owner pay
How much revenue does a NICU make per bed?
Revenue per staffed NICU bed can’t be calculated from the data given because the staffed-bed count is missing; use annual collected revenue ÷ staffed NICU beds. For context, revenue is $260M in year 1, $674M in year 3, and $1,221M in year 5, driven by utilization rising from 700% to 850%, plus service pricing, payer mix, denials, and collection timing. This is revenue only, not profit, EBITDA, or owner take-home.
Use the formula
- Annual collected revenue ÷ staffed beds
- Need actual staffed-bed count
- Year 1: $260M revenue
- Year 5: $1,221M revenue
What moves it
- Utilization rises from 700% to 850%
- Service pricing changes revenue
- Payer mix changes collections
- Denials and timing delay cash
How many NICU beds are needed to make a profit?
You can’t size profit from licensed beds alone. For NICU, the break-even answer has to use staffed beds, plus occupancy, reimbursement, cost per patient day, fixed overhead, reserves, and debt service. The model you gave shows break-even in Month 1 and a minimum cash balance of $288k, but that reflects the stated assumptions, not a bed count.
Break-even driver
- Use staffed beds, not licensed beds.
- Model occupancy by bed and day.
- Include reimbursement per patient day.
- Subtract cost per patient day and overhead.
Planning rule
- Target owner pay after reserves.
- Include debt service in cash flow.
- Keep minimum cash at $288k.
- Recheck profit if staffing changes.
What are the biggest NICU operating costs?
The biggest NICU operating costs are clinical staffing, medical supplies, diagnostics, billing, electronic health record fees, facility overhead, malpractice coverage, and capex. For the cost buildout, see What Is The Estimated Cost To Open And Launch NICU Hospital Unit? With $144k in monthly fixed overhead, that is $1.728M a year before variable costs; wage lines are $8,375k in year 1 and $965k from year 3 onward.
Main cost drivers
- Clinical staffing is the biggest load.
- Supplies and diagnostics add fast.
- Billing and EHR fees keep running.
- Malpractice and facility overhead stay fixed.
What the numbers say
- COGS + variable expense = 140% of revenue in year 1.
- That falls to 100% of revenue by year 5.
- Capex totals $465M.
- Staffing is a care constraint, not a simple cut line.
Want to see the main NICU income drivers?
1
700%-850%Bed Occupancy
More occupied, staffed beds spread fixed unit costs and lift owner income fastest.
2
$260M-$1.22BAcuity Mix
A sicker level-of-care mix raises billed value per patient and pushes revenue higher.
3
$196M-$1.07BPayer Mix
Cleaner payer mix and faster collections turn billed care into cash, and the model does not provide bed count, payer mix, or debt terms.
4
$144K/moStaffing Model
The staffing mix has to cover a $144K monthly overhead base, so poor scheduling cuts margin fast.
5
100-180/moReferral Flow
More admissions and shorter stays raise throughput, so the same unit earns more each month.
6
$4.65M+$288KCapital Load
Build-out, compliance, and reserve needs tie up cash early, and the model shows $4.65M capex plus $288K minimum cash.
NICU Core Six Income Drivers
Licensed And Staffed Bed Occupancy
Licensed and staffed bed occupancy
Licensed beds are approved beds, staffed beds are the beds the unit can safely run, and occupied beds create patient days. In this model, capacity rises from 700% in year 1 to 850% in year 5, and revenue grows from $260M to $1,221M. Low census still carries $144k in monthly fixed overhead, so empty beds drain cash fast.
More occupied beds lift revenue, but only if referrals fill the unit after staffing opens. Here’s the quick math: capacity without census means payroll and overhead hit before patient days do. One clean rule: occupancy has to rise faster than fixed cost if the owner wants real take-home pay.
Track beds, census, and fill rate
Measure licensed beds, staffed beds, occupancy, and patient days together. Also track referral volume, transfer timing, and discharge pace, because those inputs decide whether beds fill or sit idle. If census lags, phase staffing and open beds in step with real demand.
- Licensed beds and staffed beds
- Daily occupancy and patient days
- Referral flow and transfer lag
- $144k monthly fixed overhead
Watch cash weekly. When occupancy is thin, the owner still pays for the unit, so distributions should wait until payroll, overhead, and reserves are covered. Higher fill rate improves margin only when staffing stays matched to census.
1
Acuity And Level-Of-Care Mix
Acuity Mix
Acuity mix changes how much each NICU case can bill, but it also changes what it costs to deliver. In this model, prices range from $150 for lactation consultant services to $2,800 for neonatologist services by year 5. Higher acuity can lift revenue, but only if payer contracts pay for the added work and claims actually get paid.
More Level III or Level IV care does not automatically raise owner pay. Staffing ratios, respiratory support, pharmacy, diagnostics, equipment use, and compliance can rise faster than reimbursement, so gross margin can shrink even when the unit looks busier. Denials and slow collections can also push cash out past payroll and overhead.
Track Net Margin by Acuity
Track net revenue per patient day by acuity tier, not just case count. Build the estimate from payer allowed amount, staffing ratios, equipment hours, pharmacy spend, diagnostics, and denial rate. If a higher-acuity mix does not cover its incremental cost, the owner is buying complexity, not profit.
Test each service line against cash, not just billings. Add the extra labor and supply cost, then compare it with collected revenue after denials. The best mix is the one that protects margin and leaves room for owner draw after fixed overhead.
2
Payer Mix And Collections
Payer Mix and Collections
This driver is the gap between billed NICU services and cash you actually keep. Commercial contracts usually pay faster than Medicaid or managed care, while self-pay and denials slow cash and can cut realized revenue. With billing and collections fees at 40% of revenue in year 1 and 32% by year 5, a NICU can look busy on paper but still run short on cash.
Here’s the quick math: if claims lag or get denied, the revenue number is assumption-based, not guaranteed cash. That means owner draws should come after payroll, overhead, and reserves. In practice, payer mix changes both margin and pay timing, so strong volume can still miss distributions if collections slip.
Tighten Claims and Cash Controls
Track gross charges, allowed amounts, denials, and days in A/R by payer: commercial, Medicaid, managed care, and self-pay. Then compare billed revenue to cash collected each month. If the gap widens, the issue is not just volume; it is collection lag, contract rates, or claim quality.
Set a simple rule: no owner distribution until payroll, fixed overhead, and reserve cash are covered. In a NICU, that protects the business when claims are delayed or denied. The goal is not just more revenue; it is faster cash and a cleaner path to take-home pay.
3
Staffing Model
NICU Staffing Model
NICU staffing is the biggest cost gate on owner income. The model grows from 2 to 6 neonatologists, 10 to 30 NICU nurses, and 4 to 12 respiratory therapists, plus developmental, lactation, and management support. Wage lines add $8.375M in year 1 and $965k from year 3, and overtime, agency labor, and benefits are not separately provided, so actual labor cash can be higher.
Right-Size Coverage Before It Hits Cash
Track headcount by role, open shifts, overtime, and agency use against monthly treatment volume. The model assumes 100 neonatologist, 160 NICU nurse, and 120 respiratory therapist treatments per provider group in year 1, so use those inputs to test whether each hire is tied to real demand. Understaffing raises clinical risk; overstaffing cuts margin and delays owner pay.
4
Admissions, Length Of Stay, And Referral Flow
Admissions, Stay Length, and Referral Flow
Admissions create patient days, but they do not prove profit by themselves. In this NICU model, monthly treatment volume drives revenue more than raw admissions, with year 1 assumptions of 100 neonatologist treatments, 160 NICU nurse treatments, and 120 respiratory therapist treatments per provider group.
Length of stay, transfers, and discharge timing shape census, so referral flow matters as much as birth volume. If admissions rise but babies discharge faster, occupancy can still flatten. If transfers slow or referrals weaken, revenue can lag even when the unit looks busy. One clean rule: fuller beds do not always mean better cash.
Track Referrals, Not Just Admits
Measure referrals, births, transfers, discharge timing, and treatment counts each month. Tie them back to payer mix and staffing so you can see whether volume turns into billable care. The owner’s income improves when census stays steady enough to spread fixed overhead and keep payroll from outrunning collections.
Test which source feeds the best occupancy: hospital referrals, maternal-fetal medicine, obstetric volume, or transfer partners. Then forecast by monthly treatment volume, not admissions alone. If admissions look strong but average stay drops, revenue can slip fast, and owner draws should wait until cash is collected and reserve needs are covered.
5
Capital, Facility, Compliance, And Reserves
Capital, Reserves, and Owner Pay
Capital and reserves come off the top before owner distributions. In this NICU model, disclosed capex is $465M, with $15M for facility build-out, $750k for incubators and warmers, $600k for ventilators and respiratory support, and $500k for electronic health record implementation and hardware. That cash is tied up before profit rea ches the owner.
Here’s the quick math: fixed overhead is $144k per month, and minimum cash is $288k. Reserves also need to cover equipment replacement, malpractice exposure, compliance, cash lag, and debt service. If those buckets are underfunded, distributable cash looks better than it is, and owner pay becomes too risky.
Reserve Before You Distribute
Track a monthly reserve schedule that separates operating cash from true free cash. Set a floor for $288k minimum cash, then add planned replacement and compliance reserve targets before any draw. That keeps owner pay tied to cash that is actually safe to take.
Stress-test cash for delayed collections and debt service. If claims lag or denials rise, hold distributions until cash covers $144k of monthly overhead plus the reserve stack. A clean rule helps: no owner draw until fixed costs, debt, and required reserves are funded first.
6
NICU owner income scenario table
Owner income scenarios
Owner income swings with capacity, staffing, and fixed overhead in this NICU model. The low, base, and high cases map to Year 1, Year 3, and Year 5 planning periods.
| Scenario | Low CaseDownside case | Base CaseBase case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the lower owner-income path if the unit is still ramping and overhead stays heavy. | This is the modeled mid-case once the unit reaches Year 3 scale and throughput stabilizes. | This is the stronger owner-income path if the unit reaches Year 5 scale and stays efficient. |
| Typical setup | Year 1 ramp at 700% capacity with about $260M revenue, $196M EBITDA, $8.375M wage lines, and $173M fixed overhead. | Year 3 scale at 800% capacity with about $674M revenue, $564M EBITDA, 837% EBITDA margin, and $965k wage lines. | Year 5 mature case with about $1.221B revenue, $1.069B EBITDA, 850% capacity, and the highest modeled output. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $196MYear 1 ramp | $564MYear 3 scale | $1.069BYear 5 mature |
| Best fit | Use this to stress-test launch risk and early operating drag. | Use this as the main planning case for board, lender, and cash planning work. | Use this to test upside if volume, staffing, and overhead all stay efficient. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- NICU Porter's Five Forces Analysis
- NICU BCG Matrix
- NICU Business Model Canvas
- 7 Critical Financial KPIs for NICU Operations
- NICU Business Plan Template in Pre-Written Word
- 7 Strategies to Increase NICU Profitability and Margin Growth
- Analyzing NICU Running Costs: How to Operate a Specialized Unit
- NICU Startup Costs: Plan CAPEX Plus $214K Monthly Overhead
- NICU Financial Model Template in Excel
- How To Open A NICU In A Hospital: 12–24+ Month Launch Plan
- How to Write a NICU Business Plan: 7 Steps for Financial Success
- NICU Marketing Mix
- NICU Marketing Plan
- NICU Business Proposal
- NICU PESTEL Analysis
- NICU Pitch Deck Example Editable PPTX
- NICU Business SWOT Analysis
- NICU Value Proposition Canvas
Frequently Asked Questions
Reserve planning should start before owner distributions The provided model shows $465M in startup capex, $288k minimum cash, and $144k in monthly fixed overhead It does not specify a reserve policy, so owner take-home should be modeled after debt service, replacement equipment, malpractice risk, and collection delays