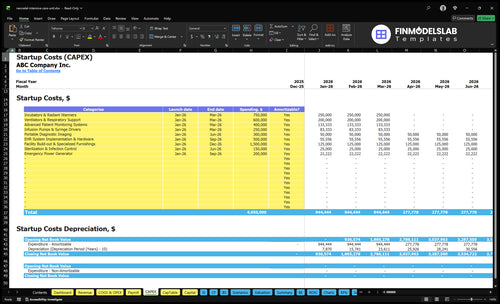
NICU Startup Costs: Plan CAPEX Plus $214K Monthly Overhead
This US NICU startup cost outline separates CAPEX, pre-opening expenses, and working capital because the model shows $213,792 in monthly fixed and admin overhead before variable care costs In the first operating year, the plan assumes 700% capacity, $217M in monthly revenue, and variable medical, diagnostic, billing, and EHR costs equal to 140% of revenue
Calculate Fuding Needs
Startup cost summary
This table breaks out NICU launch CAPEX and the excluded opening cash reserve across low, base, and high scenarios.
Highlighted CAPEX$3,750,000Base planning example
Excluded cash needs$288,000Outside CAPEX total
Funding need$4,038,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Facility Build-out & Specialized Furnishings
$1,500,000
Site-specific renovation scope and clinical room build-out
Yes
Incubators & Radiant Warmers
$750,000
Unit count and pediatric critical care equipment spec
Yes
Ventilators & Respiratory Support
$600,000
Ventilator count and support system configuration
Yes
EHR System Implementation & Hardware
$500,000
Clinical IT integration and hardware rollout scope
Yes
Advanced Patient Monitoring Systems
$400,000
Monitoring platform depth and bedside device count
Yes
Opening Cash Reserve
$288,000
Launch reserve for lease, insurance, compliance, software, and security
No
Estimate Startup Costs with Calculator
NICU Startup CAPEX Calculator
This estimates capitalized startup assets for a NICU only, including facility, equipment, IT, and support systems, and leaves out working capital and payroll runway.
!
CAPEX limits This calculator covers capitalized startup assets only. It excludes inventory, payroll runway, deposits, debt service, working capital, operating losses, and other non-CAPEX funding needs. Month 1 fixed and admin overhead is $213,792, so separate cash planning is still needed.
Does the NICU model cover startup costs?
This tab shows NICU startup-CAPEX, cost categories, launch timing, and depreciated/amortized items. Open NICU Financial Model Template and review.
Screenshot highlights
CAPEX and startup costs
Launch timing and costs
Depreciation, staffing, reserves
Compare 3 Startup Cost Scenarios
NICU launch scenarios
Lean, Base, and Full launches change startup cost because bed count, room mix, equipment depth, and staffing ramp all move together. The biggest swing comes from renovation scope and how much backup capacity you build in.
Lean, Base, and Full NICU launch cost comparison
Scenario
Lean LaunchLower-acuity setup
Base LaunchCore NICU setup
Full LaunchHigher-acuity setup
Launch model
A smaller NICU with more shared space, lower-acuity coverage, and a tighter working capital reserve.
A mid-size NICU that matches Year 1 staffing and about 70.0% capacity with standard monitoring and equipment.
A larger NICU with more private rooms, deeper backup equipment, and a larger reserve for higher-acuity care.
Typical setup
Uses fewer beds, more open bay care, lighter renovation, and only the core equipment needed to start.
Uses a mixed bed plan, a balanced open bay and private room mix, and a normal specialist ramp.
Uses more beds, stronger ventilation coverage, fuller monitoring integration, and a faster specialist staffing ramp.
Cost drivers
Smaller bed count
open bay mix
lighter equipment depth
lower ventilator capacity
tighter reserve use
Mid-size bed count
mixed room mix
standard monitoring
Year 1 staffing ramp
moderate reserve use
Higher bed count
private room mix
deeper backup equipment
integrated monitoring
larger reserve use
Planning rangeCAPEX only
$3.8M - $4.4MLower build
$4.6M - $5.2MBalanced build
$5.4M - $6.4MHigh-acuity build
Best fit
Best for teams that want a lower-acuity start and can phase in services over time.
Best for operators building to the model's Year 1 staffing and service level.
Best for systems that want more acuity, more redundancy, and room to absorb early volume swings.
!
Planning note: These scenario ranges are researched planning assumptions, not exact quotes or bids.
What drives the cost of opening a NICU?
A NICU is expensive to open because the biggest costs are the building and the clinical setup, not just the beds or machines. The main drivers are acuity level, licensed bed count, renovation versus new build, and the systems that keep fragile infants safe: medical gas, emergency power, HVAC, infection control, isolation rooms, private rooms versus open bays, ventilator depth, bedside monitoring, nurse call, and EHR integration. Staffing readiness matters too, since the model ramps clinical capacity from 700% in Year 1 to 850% in Year 5, with neonatologists growing from 2 to 6, NICU nurses from 10 to 30, and respiratory therapists from 4 to 12.
Facility cost drivers
Higher acuity raises build specs
Licensed beds shape total spend
Renovation usually costs less than new construction
Medical gas and emergency power are must-haves
Clinical readiness costs
HVAC and infection control add spend
Private rooms cost more than open bays
Ventilator depth and monitoring raise equipment needs
Specialist staffing is part of startup cost
How do NICU startup costs flow into financial projections?
For a NICU, startup costs should flow into CAPEX, startup expense, depreciation, amortization, staffing ramp, and a separate cash plan for payer delays. If you model Year 1 at 700% capacity, monthly revenue is about $217M, but you still carry about $144,000 in fixed overhead and $69,792 in admin wages. With 140% variable costs, keep accounting profit and cash timing separate so reserve needs don’t get missed.
Startup cost flow
Book setup spend as CAPEX.
Track launch costs separately.
Start depreciation on opening.
Use staffing ramp by service line.
Cash flow model
Model payer timing separately.
Hold reserves for reimbursement lag.
Layer in $144,000 fixed overhead.
Add $69,792 admin wages.
What hidden costs of opening a NICU should you budget for?
Budget past buildout: a NICU’s hidden costs are recruitment, credentialing, training, licensing prep, and payer lag, and if you want the owner-income side, see How Much Does The Owner Of NICU Business Usually Make?. The fixed opening load alone is about $48,000 a month from $25,000 malpractice insurance, $8,000 general and property insurance, $5,000 compliance fees, and $10,000 EHR base license. Year 1 admin payroll adds $837,500, or about $69,792 per month, so your working capital reserve should cover overhead plus variable costs before reimbursement stabilizes.
Opening cash drains
Recruit and credential staff first
Pay orientation and simulation training
Build clinical policies before launch
Cover payer enrollment lag early
Supply and reserve stack
Stock initial pharmacy items
Buy sterile and nutrition supplies
Budget accreditation preparation costs
Fund payroll before reimbursements hit
Key Takeaways
Buildout costs hinge on existing shell and life-safety gaps.
Equipment budgets rise with bed count and acuity.
Software is clinical spend, not office overhead.
Launch cash must cover licensing, training, and payroll.
NICU Core Five Startup Costs
Facility Construction And Hospital Buildout Startup Expense
Buildout Scope
A NICU buildout is not generic tenant work. It must cover bays or private rooms, medical gas, emergency power, HVAC, infection control, nurse stations, family areas, isolation capability, sterile storage, security, and code-compliant hospital infrastructure. The operating model already carries $75,000 monthly lease and $12,000 utilities, but it does not price construction CAPEX, so the budget needs site-specific quotes.
Price the Site
Start with the site, not a square-foot guess. The estimate changes based on existing hospital infrastructure, shell condition, room model, shared services, and the state life safety review. Ask for drawings, engineering gaps, and scope by room. One clean rule: if the shell is weak or utilities are absent, buildout cost rises fast.
Existing infrastructure?
Shell complete or raw?
Shared services available?
Keep Control
Use what the building already has, but only where it still meets code and infection control. Savings come from reusing HVAC, power, and support space, or phasing rooms instead of building all bays at once. Don’t cut life-safety work or isolation capacity. The best cost move is to avoid rebuilding systems that already pass state review.
Ask First
Before you price anything, confirm whether this is an added unit inside a licensed hospital or a new shell, because that changes engineering, utilities, and code work. Then verify the room count, isolation plan, and whether medical gas and emergency power already exist. Those answers drive the budget more than any headline rate.
Neonatal Critical Care Equipment Startup Expense
Capacity Driver
NICU equipment cost should be sized by bed count and acuity level, not by a one-device list. A Level IV unit needs incubators, radiant warmers, neonatal ventilators, CPAP systems, bedside monitors, infusion pumps, phototherapy, resuscitation gear, transport isolettes, and backup units matched to the number of beds and the sickest patients you plan to take.
What To Count
Build the budget from units × vendor price, then add spares, service coverage, and setup. Year 1 care delivery assumes 2 neonatologists, 10 NICU nurses, 4 respiratory therapists, 2 developmental specialists, and 1 lactation consultant, so the equipment mix has to support that staffing model and the expected patient volume.
Count equipment by staffed bed tier
Add backup units for critical devices
Match gear to Year 1 staffing
Acuity Push
Higher acuity means deeper budgets for ventilators, monitoring, and backup stock, because failures and cleaning cycles still have to be covered. The big gap is vendor pricing, so get quotes before final CAPEX and tie each quote to bed count, service terms, and spare inventory.
Quote each bed tier separately
Price service and replacement coverage
Ask for spare-unit pricing
Quote First
Do not lock the equipment budget from a generic list. Ask vendors for itemized pricing by bed tier, service coverage, and backup inventory, then compare those quotes with the planned Level IV acuity mix before you finalize CAPEX.
Licensing, Accreditation, And Professional Services Startup Expense
Licensing scope
This cost covers state hospital licensing, certificate of need where required, accreditation prep, life safety review, and legal, architectural, engineering, and healthcare compliance consulting. The source model carries $5,000 per month in regulatory compliance fees from Month 1. Actual spend depends on state rules, hospital licensure status, NICU level, and payer participation plans.
Budget inputs
Estimate this line by asking for state filings, consultant quotes, and months of work before opening. The key question is whether the NICU is being added to an existing licensed hospital or built as a new site. That answer changes the filing path, review depth, and how much legal and engineering help you need.
Check state hospital licensing rules first
Confirm certificate of need triggers
Price months of compliance support
Control the spend
Use one early gap review to catch missing permits, life safety issues, and policy gaps before drawings or filings get repeated. Don’t assume a flat fee will hold, because state rules and payer plans can change the scope fast. The cleanest savings come from reusing hospital systems and limiting rework.
Reuse existing hospital policies where allowed
Sequence reviews before final design
Avoid paying twice for revisions
State-specific risk
Requirements vary a lot by state, hospital licensure status, NICU level, and payer participation. This is not legal advice and it does not promise a fixed regulatory cost. If the NICU sits inside an existing licensed hospital, your timeline and consultant mix may be very different from a new facility build.
Staffing Readiness And Initial Supplies Startup Expense
Pre-Opening Team
Pre-opening staffing covers recruitment, credentialing, orientation, simulation training, and clinical protocols before the first infant arrives. The Year 1 plan assumes 2 neonatologists, 10 NICU nurses, 4 respiratory therapists, 2 developmental specialists, and 1 lactation consultant. This is launch readiness, not ongoing patient-care payroll.
Payroll Build
Payroll startup should include pre-opening wages plus admin support: Medical Director $350,000, Unit Manager $180,000, Billing and Reimbursement Manager $120,000, and other partial roles totaling $837,500 annually. Estimate it from headcount, salary quotes, and months paid before opening. That cash keeps coverage stable before revenue starts.
Initial Supplies
Initial supplies should cover sterile packs, neonatal medications, nutrition supplies, disposables, and pharmacy setup. Build the estimate from unit counts, par levels, and vendor quotes for the first weeks of care, not from a generic per-bed guess. If you underbuy here, the unit opens with staff in place but no usable inventory.
Keep It Separate
Split one-time readiness spend from recurring operating burn. Readiness includes hiring, onboarding, and stock on hand; ongoing burn includes salaries and consumables after opening. That split makes it easier to see whether the NICU is underfunded before day one or just running normal monthly volume.
Clinical Technology And Monitoring Integration Startup Expense
Clinical tech budget
For a NICU, this is care infrastructure, not office software. Budget $10,000 a month for the EHR base license, $3,000 for admin software, and EHR usage fees equal to 25% of Year 1 revenue. That stack supports documentation, billing, compliance, and alarm workflow, so it belongs in startup CAPEX planning.
What it covers
Estimate this cost from the number of interfaces and workflow links: central monitoring, bedside device feeds, EHR interfaces, nurse call, alarm management, medication administration, imaging connectivity, cybersecurity, and optional tele-neonatology. The base monthly floor is $13,000 before usage fees. Here’s the quick math: fixed software plus Year 1 activity-based fees.
Count each required interface
Price cybersecurity separately
Add tele-neonatology only if needed
How to control it
Keep the first build to the links that affect bedside care and charge capture, then phase the rest after go-live. Don’t bury software in general overhead, because that hides the real cost of clinical documentation and alarm handling. Ask for quotes by interface, device feed, and support month, not one lump sum.
Phase optional tele-neonatology later
Reject lump-sum quotes
Match builds to workflow needs
Budget rule
Use the 25% of Year 1 revenue fee as the scaling piece, then layer on the $13,000 monthly base. If your workflow needs extra interfaces for alarms, meds, or imaging, each one adds cost and must be priced before launch, not after the first patient arrives.