 Owner income$12.8M
Owner income$12.8MHow Much Outpatient Surgical Center Owners Make: $128M Before Reserves

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$12.8M  Net margin70.1%
Net margin70.1% Revenue for target pay$18.2M
Revenue for target pay$18.2M Business difficultyHard
Business difficultyHard


Key Takeaways
- Completed cases matter more than a full schedule.
- Procedure mix changes revenue, time, and supply cost.
- Labor and variable costs can erase margin fast.
- Fixed overhead is $423k monthly before owner pay.
Owner income$12.8MNet margin70.1%Revenue for target pay$18.2MBusiness difficultyHardWant to test your ASC owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, operating costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Outpatient Surgical Center model?
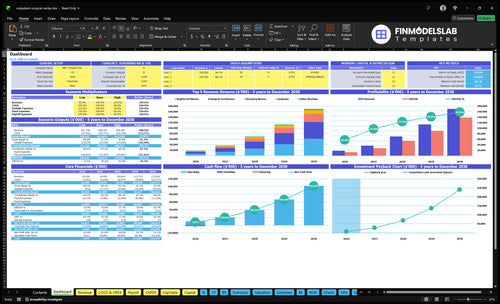
Yes — the Outpatient Surgical Center Financial Model Template should show the dashboard, revenue build, staffing, operating costs, EBITDA, and owner pay scenarios. It also tests case volume, payer mix, reimbursement, procedure mix, supplies, implants, payroll, debt service, and reserves; first-year numbers are $182M revenue, $128M EBITDA, and a 701% margin, with mature-year revenue at $1.701B. Open the model to check take-home.
Owner-income model highlights
- Owner pay scenarios
- Revenue, EBITDA, margins
- Volume and mix tests
What outpatient surgical center profit margin should owners expect?
Owners should expect a strong modeled margin in an Outpatient Surgical Center, but they need to watch cash to owners, not just EBITDA. In the first year, the model shows a 70.1% EBITDA margin after 15.5% variable costs, $507.6k fixed overhead, and $2.12M payroll; see What Is The Estimated Cost To Open And Launch Your Outpatient Surgical Center? for the setup cost side. By mid-model, margin moves to 78.8%, and mature-year margin reaches 83.0%, but labor, supplies, implants, anesthesia coverage, compliance, insurance, and equipment can still cut distributions fast.
Margin drivers
- 70.1% first-year EBITDA margin
- 78.8% mid-model margin
- 83.0% mature-year margin
- 15.5% variable costs in year one
Cash pressure points
- Labor can push cash down
- Supplies and implants add quick cost
- Anesthesia and compliance are hard to trim
- Insurance and equipment hit distributions
How much profit does an outpatient surgical center make?
An Outpatient Surgical Center makes about $128M in first-year EBITDA, $549M in the mid-model year, and $1,411M in the mature year under the provided assumptions; see What Is The Current Growth Trajectory Of Outpatient Surgical Center? for trajectory context. This is facility profit before debt, taxes, reserves, and ownership splits, not a surgeon’s clinical pay or owner take-home.
Profit view
- $128M first-year EBITDA
- $549M mid-model EBITDA
- $1,411M mature-year EBITDA
- EBITDA excludes financing and taxes
Owner cash
- Debt can cut distributions
- Taxes reduce take-home cash
- Reserves fund working capital
- Ownership splits decide payouts
How does ASC ownership structure change owner income?
Owner income at an Outpatient Surgical Center depends on how the cash is split. A surgeon-owner can receive clinical wages plus ownership distributions, while an investor-owner usually gets income based on ownership percentage and the distribution policy. In a multi-owner model, cash is often split after debt, reserves, and reinvestment are funded.
Surgeon-owner pay
- Clinical wages are separate cash.
- Distributions come on top.
- Same person can earn both.
- Model both streams separately.
Investor-owner split
- Ownership percentage drives payout.
- Distribution policy sets timing.
- Debt gets paid first.
- Reserves and reinvestment lower cash.
Want the six ASC income drivers?
1
150/moCase Volume
Year 1 totals 150 monthly treatment units, so unused operating room time drags take-home fast.
2
$2.23MStaffing Model
Year 1 payroll for surgeons, anesthesia, nurses, techs, billing, and admin is the biggest cost block, so staffing drives margin.
3
$1.8K-$6.3KReimbursement
Rates range from $1,800 anesthesia to $6,300 surgical services, so payer pressure can move income quickly.
4
3.5xProcedure Mix
Shifting more cases toward the $6,300 services lifts revenue per room hour faster than low-price cases.
5
10.5%Supply Control
Medical and sterilization supplies start at 10.5% of revenue in Year 1, so waste cuts straight into profit.
6
$42.3K/moFixed Overhead
Lease, utilities, insurance, software, and office costs stay on every month, so low volume hurts fast.
Outpatient Surgical Center Core Six Income Drivers
Case Volume And OR Utilization
OR Case Volume
When an outpatient surgical center fills the operating room (OR) with completed cases, it spreads fixed overhead across more revenue and lifts owner pay. The model starts at 3,504 units in year one, with surgeon capacity at 600% and nurse or technician capacity at 650%, so early profit still depends on turning rooms, not just booking them.
By mature year, modeled activity reaches 28,365 units and capacity rises to 850% to 900%. That higher density helps cover $423k per month in fixed overhead and leaves more cash for distributions. A full schedule does not pay the owner if cases cancel, underfill, or fail to close.
Track Completed Cases
Measure scheduled cases versus completed cases, plus surgeon and nurse or technician capacity. Here’s the quick math: more completed procedures lower fixed cost per case, while weak utilization pushes the same overhead onto fewer billable cases and cuts take-home income.
- Track completed cases daily.
- Watch cancellations and no-shows.
- Match staffing to case volume.
- Protect profitable case mix.
Use this driver to test whether the center can hold year-one volume at 3,504 units and keep scaling toward 28,365 units. If staffing stays ahead of completed cases, overtime and idle time eat margin fast; if the OR is full but cases do not complete, revenue quality drops anyway.
1
Procedure Mix And Case Economics
Case Mix Economics
Procedure mix changes what each room hour earns. In this model, first-year reimbursement runs from $1,800 for anesthesia-related activity to $5,500 for higher-priced cases, and mature-year prices rise to $2,080 to $6,300. That spread matters because the same staffed room can produce very different revenue, so owner pay depends on which cases fill the calendar, not just how full it looks.
The key inputs are case type, room time, supply use, implant cost, and payer rate. Orthopedic, ophthalmology, pain management, GI, and ENT cases need their own cost and reimbursement assumptions before anyone calls them high-margin. One expensive implant or long room time can erase the extra reimbursement fast.
Track Margin by Specialty
Track contribution by procedure, not just total volume. Here’s the quick test: reimbursement minus direct room, supply, and implant cost. If a case type looks strong on price but weak after supplies or implants, it lowers cash available for overhead and owner draw. Separate models by specialty keep the center from chasing revenue that doesn’t pay.
Manage this driver by setting a case-level dashboard with room minutes, supply spend, implant cost, and payer mix for each specialty. Review it monthly and reprice or renegotiate where the margin is thin. What this estimate hides is variation inside each specialty, so the same code can still behave differently across surgeons and payers.
2
Payer Mix And Contracted Reimbursement
Payer Mix And Reimbursement
Payer mix drives net revenue per case by shifting volume between commercial contracts, Medicare, self-pay, and collection rates. Because no payer split is provided, the model should keep this editable. First-year source reimbursement runs from $1,800 to $5,500 per case, and mature-year assumptions run from $2,080 to $6,300. Lower-paid cases cut cash available for owner pay.
Here’s the quick math: if the center lives near the low end, each case must do more work to cover the $423k monthly fixed overhead. If payer mix and collections move toward the high end, gross profit per case improves and the business gets to breakeven faster. One case can be busy and still be unprofitable.
Track the payer split every month
Build the forecast from payer type, contract rate, collection rate, and case count. Track commercial, Medicare, and self-pay separately, then compare actual net reimbursement per case to the model range. If collections slip or the mix shifts toward lower-paying payers, delay owner draws until cash clears.
- Average net reimbursement per case
- Commercial, Medicare, self-pay mix
- Collection rate by payer
- Cash collected versus billed
Test pricing and case selection against the range, not just against charges. A small drop in net reimbursement can wipe out a lot of profit when fixed costs stay flat. Watch cash, not just charges.
3
Staffing Model And Labor Cost
Labor Cost vs. Case Load
Staffing is a margin gate, not just a cost. In this outpatient surgical center, labor has to match booked cases safely, so empty room time, overtime, and overstaffing all hit owner take-home. The first-year team includes 2 surgeons, 2 anesthesiologists, 4 registered nurses, 4 surgical technicians, 2 recovery nurses, and 1 administrator.
Here’s the key input set: completed cases, hours per role, overtime, and per-diem coverage, meaning on-call temporary staff. Listed payroll is $212M in year one and $8405M in the mature year. If block schedules are uneven, labor rises before revenue does, and cash available for owner pay shrinks fast.
Track Labor Per Completed Case
Use labor cost per completed case as the main control. Compare scheduled hours to actual cases, then split overtime by role so you can see where coverage runs hot. If surgeons and anesthesia are staffed ahead of volume, the center pays for idle time, and margin slips even when the calendar looks full.
Set a weekly target for overtime and per-diem use, then document room-block fill rates by day. That lets you staff to the case mix, not just the roster. When coverage lines up with volume, more of each reimbursement dollar can reach operating profit and owner pay.
4
Supplies, Implants, And Variable Costs
Supplies, Implants, And Variable Costs
This driver covers medical and surgical supplies, implants, sterilization, billing and collections, and transaction fees. In year one, modeled variable cost is 155% of revenue: 90% supplies, 15% sterilization, 40% billing and collections, and 10% transaction fees. So a $5,500 case can carry $8,525 of variable cost before fixed overhead.
At mature scale, total variable cost falls to 118%, which still sits above revenue. That means owner pay depends on lowering implant spend, standardizing supply use, and improving collections without missing clinical quality or payer rules. One high-cost implant choice can wipe out profit from several routine cases.
Track Cost Per Case
Measure variable cost per completed case, not just total supply spend. Track reimbursement per case, implant cost, sterilization cost, billing collection rate, and transaction fees. If the mix shifts toward higher-priced procedures, test whether added reimbursement covers the extra direct cost or just looks better on the top line.
Protect clinical quality while you cut waste. Standardize t rays, negotiate implant pricing, and flag cases where supply use runs above the procedure benchmark. The best target is simple: lower cost per case without raising infection risk, cancellations, or denied claims.
- Track cost per completed case
- Separate supplies from implants
- Watch collections speed monthly
- Review procedure-level margins
5
Fixed Overhead, Debt Service, And Reserves
Fixed Overhead
Fixed overhead is the cash drag before owner pay. At $423k/month or $5.076M/year, the center must clear that amount before distributions. The named lines include $250k lease, $40k insurance, $35k utilities, and $30k professional services; the named items total $355k, so the rest sits in other fixed costs.
Debt service is not modeled here, so owner cash is operating profit - debt service - reserves. That means the center can look profitable on paper and still pay little to owners if loans are heavy or cash is held back for repairs, compliance, or slow collections. One line to watch: profit is not cash.
Track the Cash Hurdles
Measure fixed overhead per completed case every month. Use $423k ÷ completed cases, then add debt service and reserve funding so you see true owner cash. If case volume slips, overhead per case rises fast and the draw gets squeezed even when pricing holds.
- Track each fixed cost line.
- Separate debt from operations.
- Set a monthly reserve target.
- Review owner cash after collections.
Cut only what does not hurt compliance or throughput. Lease terms, service contracts, admin load, and reserve discipline matter most here. Keep distributions tied to trailing cash, not just booked profit, or owners can overdraw in a soft month.
6
Compare low, base, and high ASC owner-income scenarios
Owner income scenarios
Owner income changes fast here because staffing, capacity, and reserve needs move together. The low, base, and high cases show how EBITDA can shift as the center fills its schedule.
| Scenario | Low CaseRamp risk | Base CaseScale case | High CaseReserve risk |
|---|---|---|---|
| Launch model | This is the lower-earnings path in the first-year ramp. | This is the modeled middle path with steadier earnings. | This is the stronger earnings path if the center runs near full model capacity. |
| Typical setup | The center is still filling its schedule, with 2 surgeons, 2 anesthesiologists, 4 registered nurses, 4 surgical technicians, and 2 recovery nurses while billing and EHR fees stay high. | The center is operating at a mid-model pace with 7 surgeons, 6 anesthesiologists, 12 registered nurses, 12 surgical technicians, and 7 recovery nurses at 80.0% surgeon and anesthesiologist capacity. | The mature case uses 9 surgeons, 8 anesthesiologists, 15 registered nurses, 15 surgical technicians, and 9 recovery nurses at 85.0% surgeon and anesthesiologist capacity with lower fee drag. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | EBITDA ~$128MRamp case | EBITDA ~$549MScale path | EBITDA ~$1.411BCash stress |
| Best fit | Use this to stress-test the first year if referrals build slowly or staffing comes online in steps. | Use this as the core plan for budgeting, lender talks, and monthly tracking. | Use this to test upside if volume fills schedule blocks and reserve needs stay controlled. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Outpatient Surgical Center Porter's Five Forces Analysis
- Outpatient Surgical Center BCG Matrix
- Outpatient Surgical Center Business Model Canvas
- 7 Critical KPIs to Track for Your Outpatient Surgical Center
- Outpatient Surgical Center Business Plan Template in Pre-Written Word
- How to Increase Outpatient Surgical Center Profitability in 7 Practical Strategies
- How Much Does It Cost To Run An Outpatient Surgical Center Monthly?
- Outpatient Surgical Center Startup Costs For A 60-Month Launch Plan
- Outpatient Surgical Center Financial Model Template in Excel
- Start an Outpatient Surgical Center With a 12-24 Month Launch Plan
- How to Write an Outpatient Surgical Center Business Plan
- Outpatient Surgical Center Marketing Mix
- Outpatient Surgical Center Marketing Plan
- Outpatient Surgical Center Business Proposal
- Outpatient Surgical Center PESTEL Analysis
- Outpatient Surgical Center Pitch Deck Example Editable PPTX
- Outpatient Surgical Center Business SWOT Analysis
- Outpatient Surgical Center Value Proposition Canvas
Frequently Asked Questions
In the provided assumptions, the center produces about $128M of first-year EBITDA before debt, taxes, reserves, and ownership splits That starts from $182M revenue, 155% variable costs, $5076k fixed overhead, and $212M listed payroll Actual owner take-home may be lower because distributions are cash decisions, not just profit calculations