Outpatient Surgical Center Startup Costs For A 60-Month Launch Plan

This outline separates facility and equipment CAPEX from pre-opening expenses, working capital, and the total funding need for an ambulatory surgery center (ASC) The researched model runs Month 1 through Month 60 and shows $42,300 in monthly fixed overhead before payroll, supplies, financing, and buildout Cost ranges are planning assumptions only and will vary by specialty mix, state regulation, payer strategy, accreditation path, and facility size
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for an outpatient surgical center, not ongoing startup cash needs.
CAPEX limits This calculator excludes inventory, payroll runway, deposits, debt service, working capital, payer credentialing delays, financing fees, and Month 1 fixed overhead. Use the $25,000 lease, $2,000 maintenance, and $2,500 EHR base subscription only as operating references, not CAPEX.
What should the CAPEX tab show?
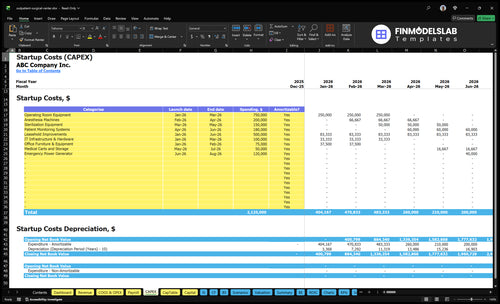
The Outpatient Surgical Center Financial Model Template CAPEX tab shows startup categories, timing, amounts, and depreciation/amortization; open it and adjust assumptions.
Screenshot checks
- CAPEX beside startup expenses
- Month 1 to 60
- Validate funding need inputs
How much does it cost to open an ASC?
An Outpatient Surgical Center cannot be priced as one clean number from the supplied data: What Is The Current Growth Trajectory Of Outpatient Surgical Center? supports operating-readiness costs, but not a vendor-backed all-in CAPEX number. Known opening cash should cover at least $42,300/month in fixed overhead and $2.185 million in Year 1 salaries, or $2.693 million before buildout, equipment, added staff, and working capital.
Known Cash Base
- $42,300 monthly fixed overhead
- $507,600 annual fixed overhead
- $2.185 million Year 1 salaries
- $2.693 million before CAPEX
Feasibility Drivers
- Set operating room count first
- Define specialty mix early
- Inspect facility shell condition
- Map accreditation path and timing
What hidden costs of opening an ASC are often missed?
If you're opening an Outpatient Surgical Center, the biggest misses are usually not the build-out itself but the cash you need before the first case: licensing, accreditation survey readiness, Medicare certification, payer contracting, credentialing delays, legal work, insurance, payroll, and opening supplies. For a related owner-income view, see How Much Does The Owner Of An Outpatient Surgical Center Usually Make?. Just the known monthly lines can hit $9,500 before volume starts, with $4,000 in insurance premiums, $3,000 in professional services, and $2,500 for the EHR base subscription, while Year 1 variable costs can run at 155% across supplies, sterilization, billing, and EHR transaction fees.
Upfront cash drains
- Licensing and survey readiness
- Medicare certification and payer contracting
- Credentialing delays before claims
- Legal and compliance work
Launch operating costs
- $4,000 insurance premiums
- $3,000 professional services
- $2,500 EHR base subscription
- Pre-opening payroll and ramp reserves
How should an outpatient surgical center funding plan be built?
Build the plan around the operating ramp, not just the build cost: lenders and investors will want a use-of-funds schedule, launch timeline, CAPEX budget, pre-opening payroll, and a working capital reserve, plus Month 1 through Month 60 projections. For an Outpatient Surgical Center, tie staffing and volume together by ramping from 2 surgeons in Year 1 to 9 in Year 5, 2 anesthesiologists to 8, 4 registered nurses to 15, 4 surgical technicians to 15, and 2 recovery nurses to 9, so cash collections can be tested against fixed overhead coverage.
Funding uses
- CAPEX budget for buildout and equipment
- Pre-opening payroll before first cases
- Working capital for early cash gaps
- Launch timeline from build to opening
Operating model
- Month 1 through 60 projections
- Payer mix by insurance and patient pay
- Procedure volume by month and year
- Staffing ramp tied to case volume
Calculate Fuding Needs
Startup Cost Summary
This table shows startup asset costs and excluded cash needs for an outpatient surgical center under low, base, and high planning cases.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| Leasehold Improvements | $500,000 | Build-out scope and finish quality | Yes |
| Operating Room and Anesthesia Equipment | $950,000 | Number of operating rooms and anesthesia setup | Yes |
| Sterilization and Patient Monitoring Equipment | $330,000 | Sterile processing and monitoring system scope | Yes |
| Clinical Technology and Office Hardware | $175,000 | EHR hardware, network gear, and office setup | Yes |
| Medical Carts, Storage, and Backup Power | $170,000 | Storage, transport carts, and generator size | Yes |
| Working Capital Reserve | $677,000 | Payroll, rent, insurance, and billing lag before cash turns | No |
Outpatient Surgical Center Core Five Startup Costs
Facility Buildout and Leasehold Improvements Startup Expense
Buildout scope
An outpatient surgical center needs OR-ready construction, HVAC, infection control, medical gas, sterile processing, recovery areas, nurse stations, accessibility, life-safety work, storage, and the right landlord delivery condition. This is a site- and code-dependent cost, so the budget should start with scope, not a blanket price.
Estimate inputs
Tie leasehold improvement estimates to square footage and OR count. Then layer in landlord delivery condition, local code scope, and trade work for medical gas, HVAC, and life safety. Use the operating anchors of $25,000 monthly lease, $3,500 utilities, and $2,000 maintenance only as runway inputs, not construction quotes.
Trim rework
Lock the room list before bids, confirm code scope early, and price medical work apart from generic tenant improvements. Don’t cut infection control or accessibility; that usually creates change orders and delays. The real savings come from fewer redesigns, cleaner landlord handoff terms, and a tighter scope letter.
Runway carry
Before opening, treat $25,000 lease, $3,500 utilities, and $2,000 maintenance and repairs as runway items while surveys, permitting, and construction finish. If the schedule slips, cash needs rise even when the buildout budget stays fixed.
Surgical Equipment and Clinical Assets Startup Expense
Clinical setup
This cost covers the reusable clinical assets that make rooms work: operating tables, surgical lights, anesthesia machines, monitors, sterilizers, instrument sets, specialty trays, recovery equipment, emergency equipment, and any imaging system you add. It is separate from disposable supplies, so do not bury gloves, drapes, drugs, or other consumables in CAPEX.
What drives the quote
Estimate this with units × unit price, then refine by specialty mix, number of ORs, imaging needs, and whether instruments are bought, leased, or shared. Here’s the quick math: more rooms and more complex cases mean more capital tied up in sterile sets, backup monitors, and recovery gear.
- Count every operating room
- Separate reusable from disposable
- Ask for lease and shared-use quotes
Keep cash tied to use
Keep spend tight by buying only the core set for your case mix, then add specialty trays after volume proves out. Don’t load CAPEX with supplies; use Year 1 medical and surgical supplies at 90% of revenue and sterilization and reprocessing supplies at 15% of revenue as operating-cost assumptions, not equipment cost.
- Start with the highest-use trays
- Lease high-cost imaging if needed
- Use vendor maintenance plans
Budget guardrail
This line item swings fast with the procedure mix. An orthopedics-heavy center needs more implants and specialty sets, while a lower-acuity center can keep the initial kit leaner. The right question is simple: what must be on hand for day one, and what can wait until case volume justifies it?
EHR, Billing, and Clinical IT Startup Expense
Core system
An outpatient surgical center needs the EHR for scheduling, clinical notes, and claim flow. Use $2,500 per month for the base subscription, plus 10% of Year 1 EHR software fees and 40% of Year 1 billing and collections fees. Keep setup and hardware separate so you can size the opening budget cleanly.
What it covers
This cost covers EHR setup, billing, clearinghouse setup, patient intake tools, phones, network gear, cybersecurity, and links to labs or anesthesia providers. Estimate it with monthly subscription × months of coverage, plus quoted setup fees and hardware quotes. That keeps case documentation and claims submission tied to the real workflow.
- Count users and locations
- Quote each integration
- Separate setup from monthly
How to control it
Start with the systems you need on day one, not every possible add-on. Fewer interfaces mean lower setup pain and fewer failure points, but don’t cut cybersecurity or billing tools that speed collections. The cleanest trim is in optional integrations; the risky trim is in anything that slows documentation, claims, or payment.
- Delay nonessential integrations
- Use one billing stack
- Keep security in scope
Budget lens
For a surgical center, this line item is not just software. It is the operating system for compliance, case documentation, scheduling, and collections speed, so underbudgeting here usually shows up later as slower billing, more rework, and delayed cash. Keep the monthly run rate visible from day one.
Licensing, Accreditation, Legal, and Compliance Startup Expense
Licensing Setup
This cost covers the pre-opening legal and regulatory work: state licensing, certificate of need where required, accreditation prep, Medicare certification, entity setup, policies and procedures, compliance consulting, architectural review, payer contracting support, and accounting setup. Requirements vary sharply by state and payer strategy, so the budget depends on location and the mix of payers you target.
Budget Inputs
Estimate this from scope, not a flat fee. Use the $3,000 monthly professional services cost as the recurring legal and accounting planning anchor, then add quoted work tied to surveys, credentialing, and payer contracts. The key inputs are state, whether CON applies, accreditation path, Medicare enrollment, and the months before first claims get paid.
- State rules and local reviews
- Payer mix and contract count
- Survey and credentialing timing
Keep It Lean
Cut cost by choosing the shortest compliant path. Reuse policy templates where allowed, narrow the payer list at launch, and separate must-have filings from optional consulting. Don’t skimp on survey prep or contract review; cheap mistakes can delay opening and cost more than the savings.
Cash Timing Risk
Delays in surveys, credentialing, or payer contracting raise working capital needs before collections start. If opening slips by even one month, the center still pays rent, payroll, and professional services before revenue begins. That timing risk matters more than the filing fee itself.
Pre-Opening Payroll, Supplies, Insurance, and Working Capital Startup Expense
Payroll bucket
Pre-opening payroll is working capital, not CAPEX. For Year 1 staffing, the anchor payroll is $2.12 million a year: 2 surgeons at $350,000 each, 2 anesthesiologists at $280,000, 4 registered nurses at $85,000, 4 surgical technicians at $60,000, 2 recovery nurses at $80,000, and 1 center administrator at $120,000.
Startup cash needs
This bucket also covers training, medical director coverage, malpractice and general liability insurance, initial drugs, disposables, linens, sterile supplies, and launch marketing. Here’s the quick math: a 3-month payroll reserve alone is about $530,000 before adding insurance, supplies, and pre-opening labor. That is the cash runway question, not a buildout question.
- Count months before first collections.
- Separate payroll from equipment.
- Reserve extra for payer delays.
Cost control
Keep this spend lean by staging hires, cross-training nurses and techs, and starting with only the staff needed for open cases. Don’t underbuy insurance or sterile supplies to save cash; that usually backfires fast. Use quotes for malpractice, general liability, and consumables, then set runway to cover slow ramp and delayed reimbursements.
- Hire in case volume order.
- Price insurance before launch.
- Track supply burn weekly.
Working capital plan
For an outpatient surgical center, this line item should hold the gap between opening day and steady collections. Build it from payroll weeks, insurance premiums, and opening consumables, then add buffer for credentialing or payer timing. If collections slip, the first pressure point is cash, not the operating room.
Compare 3 Startup Cost Scenarios
Startup Cost Scenarios
Lean, Base, and Full launch plans change cost fast because room count, staffing depth, and specialty mix drive both capex and monthly burn. The model also starts with $42,300 in fixed overhead and a 155% Year 1 variable cost load.
| Scenario | Lean LaunchPhysician-owned start | Base LaunchGrowth platform | Full LaunchMulti-specialty center |
|---|---|---|---|
| Launch model | A leased-shell start with one focused specialty mix, fewer rooms, and tight working capital. | A standard buildout with first-year staffing and a Month 1 through Month 60 operating model. | A larger center with more OR capacity, broader specialty mix, imaging needs, and deeper recovery coverage. |
| Typical setup | Keep the buildout light, staff to the first room set, and delay nonessential equipment. | Fund full core equipment, normal recovery coverage, and enough cash to absorb ramp-up. | Add equipment, more staff depth, higher reserves, and extra capacity for a wider case mix. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | $1.8M - $2.4MLower capital | $2.6M - $3.4MBalanced build | $3.8M - $5.0MHigher reserve |
| Best fit | Fits physician groups that want a smaller first site and can grow room count later. | Fits owners who want a stable launch with room to add volume without reworking the site. | Fits groups aiming for a wider referral base and a faster path to multi-specialty scale. |
Planning note: These scenario ranges are researched planning assumptions, not exact vendor quotes or lender terms.
Related Products
- Outpatient Surgical Center Porter's Five Forces Analysis
- Outpatient Surgical Center BCG Matrix
- Outpatient Surgical Center Business Model Canvas
- 7 Critical KPIs to Track for Your Outpatient Surgical Center
- Outpatient Surgical Center Business Plan Template in Pre-Written Word
- How to Increase Outpatient Surgical Center Profitability in 7 Practical Strategies
- How Much Does It Cost To Run An Outpatient Surgical Center Monthly?
- Outpatient Surgical Center Financial Model Template in Excel
- How Much Outpatient Surgical Center Owners Make: $128M Before Reserves
- Start an Outpatient Surgical Center With a 12-24 Month Launch Plan
- How to Write an Outpatient Surgical Center Business Plan
- Outpatient Surgical Center Marketing Mix
- Outpatient Surgical Center Marketing Plan
- Outpatient Surgical Center Business Proposal
- Outpatient Surgical Center PESTEL Analysis
- Outpatient Surgical Center Pitch Deck Example Editable PPTX
- Outpatient Surgical Center Business SWOT Analysis
- Outpatient Surgical Center Value Proposition Canvas
Frequently Asked Questions
Opening cash should cover CAPEX plus early operating costs before collections stabilize The researched model shows $42,300 in monthly fixed overhead before payroll, 155% Year 1 variable costs, and Year 1 staffing with 2 surgeons, 2 anesthesiologists, 4 registered nurses, 4 surgical technicians, and 2 recovery nurses Buildout and equipment still need separate vendor-backed estimates