 Time to Open6 monthsLaunch runway
Time to Open6 monthsLaunch runwayHow to Open a Pain Management Clinic in 4–9+ Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6 monthsLaunch runway  Launch Sequence7 stagesCompliance first
Launch Sequence7 stagesCompliance first Key BottleneckPayer credentialingApproval path
Key BottleneckPayer credentialingApproval path First Revenue StepScheduled consultsCoverage verified
First Revenue StepScheduled consultsCoverage verified


Opening a pain management clinic in the United States commonly takes 4–9+ months, but credentialing, provider availability, buildout, and state rules can stretch that timeline The core steps are entity setup, provider licensing alignment, facility setup, clinical protocols, controlled-substance safeguards if prescribing, payer enrollment, EHR and billing setup, hiring, referral outreach, and soft launch In the researched Year 1 plan, the clinic starts with 1 interventional physician, 1 physical therapist, 1 nurse practitioner, 1 physician assistant, and 1 clinical psychologist at 65% capacity Here’s the quick math: Year 1 modeled revenue at 65% capacity is about $146,445/month before billing lag and denials
Time to Open6 monthsLaunch runwayLaunch Sequence7 stagesCompliance firstKey BottleneckPayer credentialingApproval pathFirst Revenue StepScheduled consultsCoverage verifiedLaunch timeline
Short web summary of the launch plan; the XLSX export contains the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Legal / compliance
- Form entity
- Board review
- Malpractice policy
- HIPAA policies
- DEA filing
Facility / buildout
- Lease signing
- Floor plan
- Buildout work
- IT install
- Safety inspection
Clinical / protocols
- Intake forms
- Care pathways
- Prescribing protocols
- Chart templates
Staffing / hiring
- Physician hire
- Provider hire
- PT recruit
- Psychologist hire
- Front desk hire
- Team training
Payer / billing
- Payer list
- Credentialing
- Contract review
- Billing setup
- Claims test
Referrals / launch
- Primary care outreach
- Ortho outreach
- Neurology outreach
- Soft opening
Have you tested the launch plan before opening the Pain Management Clinic?
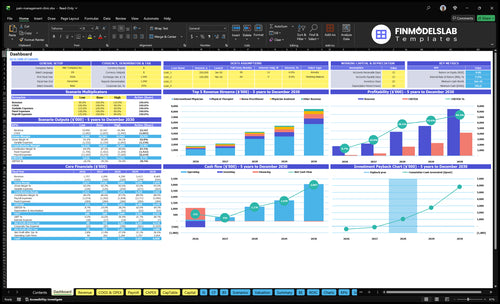
The Pain Management Clinic Financial Model Template shows revenue, costs, cash needs, assumptions, and break-even logic; at 65% capacity, Year 1 monthly revenue is about $146,445.
Model highlights
- Interventional treatment: $1,500
- PT, NP, PA, psychology: $120-$180
- Variable costs: 14%
- Cash gap before collections
What are the requirements to open a pain management clinic?
To open a Pain Management Clinic, you need licensed providers, the right legal entity, state medical board clearance, facility compliance, malpractice coverage, HIPAA-ready records, payer credentialing, clinical protocols, and controlled-substance safeguards if prescribing. With over 50 million US adults living with chronic pain, demand is real, but readiness depends on provider, documentation, and payer setup, as covered in What Is The Most Critical Metric For Evaluating The Success Of Pain Management Clinic?. This is general US guidance, not legal advice.
Legal readiness
- Confirm physician ownership rules by state
- Form the appropriate business entity
- Appoint medical director and supervision plan
- Verify provider licenses and scope rules
Operating setup
- Secure malpractice insurance before launch
- Set HIPAA, EHR, and billing systems
- Complete payer credentialing and eligibility checks
- Add DEA registration where applicable
What mistakes create the biggest pain clinic launch risks?
The biggest launch risk for a Pain Management Clinic is opening before payer approvals, billing tests, and prior authorization workflows are working. Here’s the quick math: with fixed costs starting at $15,000/month for rent plus $2,500/month for utilities, delay burns cash fast, so don’t go live until intake, documentation, and controlled-substance safeguards are signed off. Weak referral ties, undertrained staff, and EHR or billing errors can turn a clinical launch into a denial problem, not a care problem.
Big launch risks
- Start before payer approval
- Skip prior authorization steps
- Undertrain intake and charting staff
- Miss controlled-substance policy gaps
Best launch fixes
- Run billing tests first
- Verify payer status early
- Stage services by readiness
- Document prescribing safeguards
How do pain management clinics get their first patients?
Pain Management Clinic gets its first patients from clinically appropriate referrals, not broad traffic alone. Build outreach with primary care, orthopedics, neurology, spine specialists, physical therapy, workers’ compensation channels where relevant, hospital discharge networks, insurance directory visibility, and local search; first revenue is scheduled, billable visits with verified coverage, not website leads. If you’re also sizing the launch, see How Much Does It Cost To Open A Pain Management Clinic?
Referral sources
- Start with primary care referrals.
- Work orthopedics and neurology.
- Include spine and physical therapy.
- Use hospital and insurance directories.
Intake checks
- Confirm the referral reason.
- Verify payer eligibility.
- Check prior authorization needs.
- Plan for 65% Year 1 capacity.
Confirm the clinic is ready before scheduling first patients
Launch readiness checklist
Use this go-live approval checklist before opening the pain management clinic.
Compliance
- Ownership structure reviewedCritical
Confirms physician ownership rules before contracts and capital go live.
- State licenses verifiedCritical
Shows every treating clinician can practice in the launch state.
- Malpractice policy boundCritical
Protects the clinic before any patient visit or procedure starts.
- HIPAA policies approvedHigh
Keeps patient data handling in line with privacy rules.
Facility
- Lease and build-out signedCritical
Locks the site before equipment and staffing spend move forward.
- ADA access clearedHigh
Patients need safe, compliant access from the first operating day.
- Exam and procedure rooms readyCritical
Supports diagnosis and treatment without crowding or delays.
- Infection control supplies stockedHigh
Cuts safety risk for injections, wound care, and room turnover.
Systems
- EHR configuredCritical
The charting system must work before the first patient is seen.
- Billing rules testedCritical
Billing errors can block cash and delay revenue from day one.
- Payer enrollment confirmedCritical
Needed if the clinic will bill insurers instead of cash-pay only.
- Cash-pay limits setMedium
Defines what can launch before payer approvals clear.
Staffing
- Year 1 roles staffedCritical
Year 1 needs the five clinical roles fully covered before opening.
- Intake team trainedHigh
Intake mistakes can slow visits and break the first revenue flow.
- Prior auth process testedHigh
This matters if insured patients need approvals before treatment.
- Referral scheduling trainedHigh
Referral flow keeps new patients moving into visits without gaps.
Care flow
- Pain protocols approvedCritical
Standard care paths keep treatment consistent across providers.
- Consent forms signed offCritical
Patients must accept risks and treatment terms before care starts.
- Documentation standards setHigh
Clean notes support billing, follow-up care, and audits.
Finance
- Runway covers fixed costsCritical
Monthly fixed overhead starts near $23.7k before variable and wage costs.
- Launch volume matches capacityHigh
Year 1 volume must fit the staffed schedule or service slips fast.
- Go-live signoff completeCritical
No launch should happen until compliance, systems, and cash checks pass.
Which launch drivers decide whether the clinic opens cleanly?
1Compliance Gate
License gateMissing licenses, DEA registration, or state-rule alignment can block opening entirely.
2Staffing Ready
5 rolesSigned coverage for five clinical roles keeps day-one care stable and reduces rescheduled referrals.
3Billing Stack
6% revCredentialing, claims, and denial tracking speed cash collection after consults turn into billable visits.
4Facility Ready
$17.5K/moFinished rooms, equipment, and storage cut cancellations and keep patient flow safer.
5Referral Flow
65% capActive referrals and local listings help fill schedules and move the clinic toward 65% capacity.
6Runway Check
6 moCash has to cover rent, staffing starts, billing lag, and denied claims before volume lands.
Regulatory, Licensing, and Controlled-Substance Compliance
Compliance Gate
For a pain management clinic, launch compliance is binary: if licenses, DEA registration where needed, or state-rule alignment are missing, the door stays shut. Day-one readiness starts with documented provider licensure, medical board review, malpractice coverage, HIPAA policies, prescribing protocols, and chart standards that match the clinic’s actual scope.
The risk is highest when ownership, supervision, or controlled-substance rules are checked late. If those pieces are off, you can lose opening time, block prescribing, or force a service reset after patients are already scheduled. Use professional legal and compliance review before you commit to staffing, templates, and patient start dates.
Front-Load the Review
Start with a written scope check: what services you will offer, what each provider can do, and whether controlled substances are part of the model. Then verify the full packet against state law and payer rules, because those rules drive what must be approved before opening. One clean file is better than five verbal assurances.
Build a launch folder with licenses, malpractice proof, HIPAA policies, prescribing rules, storage and monitoring steps if controlled substances are used, and charting standards. If any item is pending, treat it as a launch blocker, not an admin task. That keeps opening dates realistic and reduces audit pain later.
- Confirm each provider license.
- Verify DEA needs by scope.
- Document supervision and ownership.
- Test chart and prescribing workflows.
- Store policies in one launch file.
1
Provider and Clinical Staffing Readiness
Staffing Ready on Day One
For a pain management clinic, staffing readiness is what turns approvals into bookable visits. The Year 1 model starts with 1 interventional physician, 1 physical therapist, 1 nurse practitioner, 1 physician assistant, and 1 clinical psychologist. If coverage, credentialing packets, schedules, supervision rules, care pathways, and training are not signed off, referrals get pushed and opening slips.
The main bottleneck is usually physician or advanced-practice provider availability. If payer credentialing, EHR templates, or procedure support are late, day-one capacity drops and fewer rescheduled referrals turn into a real launch risk. This model depends on coordinated handoffs, so one missing role can slow the whole clinic.
Lock Coverage Before Scheduling
Build the launch order around what must be in place before the first patient is booked. Start with signed coverage, then confirm supervision rules, then load care pathways and documentation into the EHR. Train intake staff on referral handling and only open the calendar after each role is credential-ready.
- Verify payer credentialing for each clinician.
- Test EHR templates before launch.
- Document procedure support if offered.
- Match schedules to supervision rules.
- Train intake and charting before booking.
If one clinician is late, the schedule tightens fast because this clinic runs on coordinated visits, not solo slots. Clean staffing readiness gives stable day-one capacity and reduces last-minute referral reschedules.
2
Payer Credentialing, Billing, and Revenue Cycle
Payer Credentialing and Cash Setup
Credentialing is a cash gate, not paperwork. A pain management clinic can see patients before payer approvals are done, but it may not get paid on time. That creates a day-one cash problem, especially when referred consults start coming in before payer applications, provider credentialing, and prior authorizations are live.
The operational inputs are provider licenses, payer contracts, billing system setup, CPT coding workflow, claim submission testing, denial tracking, and the patient balance process. These pieces need to be mapped before the first visit so the clinic can collect cleanly from referral through payment.
Year 1 assumes billing service fees at 4% of revenue and electronic health record (EHR) subscriptions at 2%. Here’s the quick math: if approvals lag, the clinic still carries lease, staffing, and training costs, but cash collections slip. The bottleneck is opening before the payer side is live.
Test the revenue cycle before day one
Build the billing path in order: payer enrollment, provider credentialing status, eligibility checks, prior authorization rules, CPT coding, claim submission, denial workflow, and patient balance steps. Assign one owner for each step and document who clears errors. One clean test claim is better than ten live visits with broken billing.
- Confirm all payer applications are submitted
- Check every provider’s credentialing status
- Test claim submission before opening
- Train staff on denials and balances
What this protects: faster conversion from referred consults to collected revenue, fewer write-offs, and less cash strain in the first weeks after launch.
3
Facility, Equipment, and Procedure Readiness
Facility Readiness
If the clinic opens before rooms, flow, and equipment are set, day-one care slows fast. For a pain management clinic, readiness means exam rooms, procedure space if offered, patient flow, ADA access, medication storage, infection control, IT, phones, scheduling, equipment installation, and vendor training. The model carries $15,000/month lease and $2,500/month utilities from Month 1 through Month 60, so a late buildout burns cash before revenue starts.
The gate is simple: match the site to the service menu. If you plan procedures, you also need any required inspections, staffing in place, and payer readiness; if you do not, the space can stay leaner. Weak setup drives cancellations, slow room turnover, and unsafe patient flow, which hurts early visits and creates compliance risk.
Match Scope to Space
Start with the service model, then size the space. A clinic that only runs consults needs a different build than one that adds procedures on day one. Map room count, equipment placement, storage, and IT before signing off on the final layout, because lease costs start at $15,000/month and utilities at $2,500/month even if the space is not ready.
- Verify ADA access and patient flow.
- Install phones, scheduling, and IT.
- Train vendors before opening.
- Confirm medication storage and infection control.
- Finish inspections, if required.
- Test equipment and room turnover.
4
Referral Pipeline and First-Patient Generation
First-Patient Referral Flow
Referral flow is what keeps a pain clinic from opening to empty chairs. Active referral conversations with primary care, orthopedics, neurology, spine, physical therapy, workers’ compensation contacts where relevant, hospital discharge teams, insurance directories, and local search need to be live before day one. Without that pipeline, even strong clinical staffing won’t turn into booked consults.
The target is a cleaner ramp to Year 1 at 65% capacity, not a launch built on hope. Web traffic is not demand; referred, clinically appropriate patients are. If records intake, coverage checks, and response-time standards are late, first appointments slip and fixed costs like $15,000 rent and $2,500 utilities start burning cash before revenue catches up.
Pre-Open Referral Setup
Build the intake path before opening: referral form, chart request process, insurance coverage check, and appointment script. Assign one person to answer referrals fast and log every source. That keeps patients from dropping while the clinic is still new. One slow handoff can send a referrer to the next practice.
- Referral form ready
- Records intake assigned
- Coverage check before booking
- Response-time standard set
- Appointment script tested
Test the handoff with real cases from each source: PCP, specialist, discharge, and directory lead. Make sure the front desk, clinical team, and billing side know who calls back, who reviews records, and who schedules first. If those steps are not timed, day-one slots stay open and the first month looks weaker than the market actually is.
5
Financial Runway and Launch-Volume Assumptions
Runway Before Volume
This driver matters because the model tests whether the pain clinic can open and keep operating on day one, not just whether it looks profitable on paper. At 65% capacity, monthly revenue is about $146,445 from 5 clinical roles, so the opening plan has to support real patient flow, not a theoretical schedule.
Here’s the quick math: direct and variable costs are 14% of revenue in Year 1, but fixed commitments still include a $15,000/month lease and $2,500/month utilities. The launch breaks if the team hires, signs space, or stocks supplies before referrals and payers can support volume.
Cash First, Then Capacity
Build runway for the launch lag: credentialing, billing delay, staff start dates, rent, utilities, supplies, and denied claims. The founder should tie cash needs to the opening date and first 90 days, because a fee-for-service clinic can look busy and still run short on cash if collections lag.
- Confirm payer approvals before staffing.
- Match lease start to ramp timing.
- Test claims and denial workflows.
- Hold cash for launch-month supplies.
One line: if referrals and payer cash do not support the planned volume, opening early only speeds up burn.
6
Related Products
- Pain Management Clinic Porter's Five Forces Analysis
- Pain Management Clinic BCG Matrix
- Pain Management Clinic Business Model Canvas
- 7 Critical KPIs for Scaling a Pain Management Clinic
- Pain Management Clinic Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Pain Management Clinic Profitability
- Estimating Monthly Running Costs for a Pain Management Clinic
- Pain Management Clinic Startup Costs: $520K+ Known CAPEX
- Pain Management Clinic Financial Model Template in Excel
- How Much Does a Pain Management Clinic Owner Make at $146K/Month?
- How to Write a Pain Management Clinic Business Plan in 7 Steps
- Pain Management Clinic Marketing Mix
- Pain Management Clinic Marketing Plan
- Pain Management Clinic Business Proposal
- Pain Management Clinic PESTEL Analysis
- Pain Management Clinic Pitch Deck Example Editable PPTX
- Pain Management Clinic Business SWOT Analysis
- Pain Management Clinic Value Proposition Canvas
Frequently Asked Questions
Start with licensing and payer readiness before marketing The practical sequence is entity setup, state medical board review, provider credentialing, facility setup, EHR and billing, staff training, referral outreach, and soft launch Use 4–9+ months as a planning range The Year 1 model assumes 5 clinical roles operating at 65% capacity