 Time to Open12-24+ monthsLaunch runway
Time to Open12-24+ monthsLaunch runwayHow to Open a Patient-Specific Implant Company in 12–24+ Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open12-24+ monthsLaunch runway  Launch Sequence7 stagesScope first
Launch Sequence7 stagesScope first Key BottleneckRegulatory gateApproval path
Key BottleneckRegulatory gateApproval path First Revenue StepFirst caseCase approval
First Revenue StepFirst caseCase approval


You’re building a regulated medical device operation, not just a custom fabrication shop A practical US patient-specific implant launch plan covers FDA strategy, QMS readiness, imaging-to-design controls, validated manufacturing, supplier qualification, surgeon access, and a first-year model with 3,000 planned units and $1289 million in modeled revenue Detailed startup cost, funding, valuation, and owner income work should sit in separate planning resources
Time to Open12-24+ monthsLaunch runwayLaunch Sequence7 stagesScope firstKey BottleneckRegulatory gateApproval pathFirst Revenue StepFirst caseCase approvalLaunch timeline
This is a short web summary of the launch plan, and the XLSX export carries the detailed Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10
Regulatory strategy
- Intended use
- Pathway review
- Submission plan
- Design controls
QMS and docs
- QMS blueprint
- Document control
- SOP drafts
- Record training
Facility and equipment
- Cleanroom layout
- Printer install
- Finishing station
- Scanner setup
- Sterilizer install
Imaging to CAD
- Image intake
- Segmentation build
- CAD review
- File transfer
Validation and suppliers
- Supplier qualify
- Material verify
- Process validate
- Sterilize cycle
- Packaging check
- Release criteria
Staffing and launch
- Hire core team
- Case training
- Surgeon outreach
- Hospital credentialing
- First cases
Why test the launch plan in the model before day one?
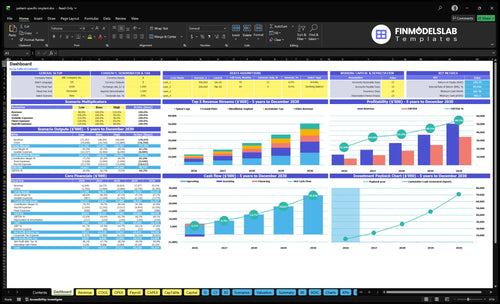
The screenshot in the Patient-Specific Implant Manufacturing Financial Model Template shows revenue, costs, cash needs, assumptions, and break-even logic; open the model.
Launch model highlights
- 3,000-unit Year 1 plan
- $1.289M revenue mix
- 50% factory allocations
- Runway gaps from delays
What launch mistakes block a custom implant manufacturer?
Patient-Specific Implant Manufacturing usually stalls when teams sell before QMS readiness, skip validation, or launch with weak DICOM-to-CAD controls. A plant can be machine-ready and still blocked by an unqualified supplier, and first revenue can still lag if hospital purchasing is not signed. Freeze intended use, lock design controls, and validate the process before you take orders.
Big launch blockers
- Selling before QMS is ready
- Weak DICOM-to-CAD review controls
- Unqualified critical material suppliers
- Missing lot traceability and approvals
Launch checks to run
- Validate segmentation and CAD review
- Run IQ/OQ/PQ on equipment
- Confirm sterilization and packaging evidence
- Train staff and test the financial model
How long does it take to launch a patient-specific implant company?
Patient-Specific Implant Manufacturing usually takes 12–24+ months to launch, not a fixed opening date. The clock starts with the FDA pathway and QMS buildout, then moves through facility setup, equipment qualification, process and sterilization validation, supplier readiness, hospital contracting, and first clinical use. Year 1 volume of 3,000 units and $12.89 million revenue only fit after those gates are cleared.
What sets the pace
- Regulatory path comes first
- QMS must be built
- Facility and equipment need qualification
- Imaging-to-design must validate
Where delays hit
- Unclear intended use slows review
- Weak docs cause rework
- Biocompatibility gaps delay launch
- Hospital approval can lag
How do you get first customers for custom implants?
First customers for Patient-Specific Implant Manufacturing usually come from surgeon champions, not broad ads. Start with What Are The Operating Costs Of Patient-Specific Implant Manufacturing? and build one qualified clinical pathway with documented case selection, compliant product info, and a clear manufacturing release. The first order depends on trust, traceability, regulatory status, and reliable delivery.
Get the first case
- Start with a surgeon champion
- Match one clear clinical need
- Document case selection
- Use compliant product information
Clear the hospital path
- Complete vendor credentialing
- Set up purchasing early
- Prepare value analysis review
- Align reimbursement and delivery timing
Confirm whether the implant business is ready to open
Launch readiness checklist
Use this go-live approval checklist before opening to confirm the implant manufacturing launch is ready.
Regulatory
- FDA path confirmedCritical
The pathway and counsel memo must be signed before launch orders or sales start.
- Registration and listing filedCritical
Filing proof and device scope should match the final implant line.
- Go-live regulatory signoff readyHigh
Final approval should confirm no open regulatory blockers.
QMS
- QMS document set approvedCritical
The document set must be controlled before any production release.
- Design controls activeCritical
Design inputs, reviews, and risk files keep custom units traceable.
- Complaint and CAPA liveHigh
Complaint handling and CAPA must be active before first cases ship.
Digital flow
- DICOM intake validatedCritical
Image checks protect intake quality before any custom design work starts.
- CAD review checklist approvedHigh
The review should lock landmarks, dimensions, and file security rules.
- Surgeon signoff workflow clearHigh
Surgeon approval must happen before fabrication to avoid wrong anatomy.
Production
- Machine and process qualifiedCritical
Qualification proves the printer and finishing steps work the same way each run.
- Sterilization pathway validatedCritical
Validated sterilization protects patient safety and release timing.
- Packaging and biocompatibility clearedCritical
Packaging and material evidence must support the final implant claims.
Supply chain
- Titanium powder supplier qualifiedHigh
Powder quality and lead times must be stable before launch volume starts.
- Polymer, resin, and packaging approvedHigh
Approved vendors keep custom parts, guides, and packaging on spec.
- Sterilization and shipper approvedHigh
Sterilization and shipping partners must meet release and handling rules.
- Core staff assignedCritical
You need clear owners for quality, regulatory, engineering, validation, and sales.
- Surgeon onboarding completedHigh
Surgeons need a clean path to review cases and place first orders.
- Hospital purchasing path clearedCritical
Hospital buying and credentialing must work before first revenue can land.
- 3,000-unit model testedCritical
The model should tie 3,000 Year 1 units to $12.89M revenue and runway.
- Go-live commercial signoff readyHigh
Commercial signoff should confirm cash, contracts, and first orders are ready.
Which launch drivers matter most?
1Regulatory Gate
GateRegulatory path and quality system are the launch gate, so production can start without resets.
2Imaging Flow
File lockValidated imaging-to-design rules keep each patient file controlled and cut rework before release.
3Process Validation
IQ/OQ/PQEquipment and material controls prove repeatable output for planned Year 1 volume.
4Sterile Supply
Supply holdSterilization, packaging, and supplier checks block release holds and support hospital trust.
5Hospital Access
3,000 unitsSurgeon and hospital access convert validated implants into orders, and Year 1 assumes 3,000 units.
6Quality Systems
Audit readyTraining, documentation, and post-market systems speed issue response and keep audits cleaner.
Regulatory Pathway and QMS Readiness
Regulatory Pathway First
If the FDA pathway and device classification are not clear, this business cannot open on time. For patient-specific implants, the launch gate is a defined intended use, a submission strategy, and an ISO 13485-style QMS that can handle document control, design controls, risk management, labeling, traceability, complaint handling, CAPA, and production release records.
This is the step that keeps you from building a plant before you can legally ship from it. With a Year 1 plan of 3,000 units, even one regulatory reset can push first revenue, burn cash, and make hospital review harder because the file is not clean.
Lock the QMS Before Buildout
Before you buy equipment, verify intended use, classification logic, and submission path with regulatory counsel and current FDA guidance. Then assign trained quality staff to own the core SOPs, supplier files, and validation evidence so the launch date is based on facts, not hope.
- Freeze document control early.
- Define design review and release steps.
- Collect supplier and material evidence.
- Test complaint and CAPA handling.
- Keep production release records audit-ready.
If the QMS is thin, every change turns into a restart. That slows first-day shipping, adds rework, and can block hospital review even when the implant itself is ready.
1
Imaging-to-Design Workflow Validation
Imaging-to-CAD Workflow Control
This launch driver matters because each implant starts with a patient file, not a stock part. If DICOM intake, segmentation, CAD modeling, and surgeon review are not locked down, manufacturing can’t start on time and day-one output will slip.
The risk is simple: undocumented design changes or inconsistent segmentation create reworks, delay production file release, and weaken traceability. In cranial plate planning, imaging, CAD, approval, and final release all have to match before a case can move forward.
Lock the File-Release Gate
Before opening, verify the full path from imaging intake to production-ready CAD: intake rules, segmentation protocol, anatomical landmarks, design checks, revision history, and surgeon approval. One clean workflow beats a fast one that keeps changing.
Also assign who can edit, who can approve, and who can release the file. Use secure records and a validated software process so every patient-specific file has clear ownership, clear version control, and no surprise redesigns after the case is already in motion.
- DICOM intake rules before case start
- Segmentation protocol for consistent models
- Surgeon sign-off before release
- Revision history kept on every file
- Secure records for traceability
2
Manufacturing Process Validation and Equipment Readiness
Process Validation and Equipment Readiness
Repeatability across patient-specific parts is the launch gate here. Before first sale, the line needs equipment installation, IQ/OQ/PQ, material controls, build settings, post-processing, inspection, dimensional verification, lot traceability, and clear production release rules. If any one step is weak, you can make parts but not release them with confidence, and day-one shipments slip.
This also drives cash. The disclosed factory mix already puts 12% to quality control, 15% to indirect production labor, 8% to machine maintenance, 5% to utilities, and 10% to sterilization validation, or 50% of revenue before other costs. If equipment is not qualified and inspection is not calibrated, those dollars fund delay instead of output.
Qualify Before Release
Before opening, lock the sequence: install the machine, complete IQ/OQ/PQ, then verify build parameters, post-processing, and inspection tools. Train technicians, collect supplier material certificates, and write the release checklist so quality review can sign off each lot. No release criteria, no shipment.
If validation slips, planned Year 1 volume stays on paper. A missed qualification lot, late maintenance plan, or uncalibrated inspection tool can force rework, hold inventory, and push first revenue out while labor and overhead keep running.
- Calibrate inspection tools first.
- Document lot traceability daily.
- Assign maintenance ownership now.
- Run one full validation lot.
3
Sterilization, Packaging, Biocompatibility, and Suppliers
Sterile Barrier and Supplier Readiness
This driver can block opening fast. If the implant does not have a defined sterilization method, validated medical device packaging, and enough ISO 10993 biocompatibility evidence, you can’t release product with confidence. For a patient-specific implant business, that means delays in first shipment, more release holds, and weaker hospital trust on day one.
The risk is bigger when titanium alloy powder, PEEK polymer filament, biocompatible resin, or medical grade packaging arrive late or lack material certifications. One weak supplier can slow the whole launch.
Lock the release path before first build
Before opening, verify the sterilization route, package validation, and shelf-life assumption for each implant line. Confirm supplier qualification, backup vendors where needed, and shipping logistics so the sterile barrier still holds after transit. If any material certificate is missing, treat it as a launch risk, not a paperwork task.
Assign one owner to track incoming lots, certificates, and packaging test status. Keep the launch file tight: sterilization method, ISO 10993 evidence, material certifications, validated packaging, and approved suppliers. That is what keeps day-one release from stalling.
- Confirm sterilization method early
- Validate packaging before production
- Collect material certificates
- Qualify backup vendors now
- Test shipping and shelf life
4
Surgeon, Hospital, and Commercial Access Readiness
Hospital Access to First Orders
This driver decides whether a surgeon’s interest turns into a purchase order. A willing surgeon is not enough if the hospital has not cleared vendor credentialing, the value analysis committee (VAC) path, reimbursement review, and delivery rules. That is the gap between a validated implant and a first hospital order, so launch timing depends on access, not just product readiness.
Year 1 assumes 3,000 units, or about 250 units a month on a straight-line run rate. If validated product files, regulatory documents, insurance, quality records, and customer service are not ready, the hospital can block the order even when the surgeon wants to start. That pushes revenue out and leaves production capacity underused.
Pre-Clear the Order Path
Map each target account before opening. Confirm the surgeon champion, the defined clinical need, case selection criteria, compliant materials, and who signs off on buying. The quick test is simple: can one case move from surgeon request to approved vendor status to shipment without a manual scramble?
- Confirm credentialing for each hospital.
- Prep VAC packet and clinical rationale.
- Attach reimbursement notes early.
- Lock delivery and service commitments.
- Keep product files ready for review.
Keep one launch file per account with product files, regulatory paperwork, insurance, quality records, and a named service contact. If any piece is missing, the hospital can pause the order after the surgeon has already committed. That is the fastest way to miss day-one revenue and create avoidable rework.
5
Staffing, Training, Documentation, and Post-Market Systems
Staffing, Training, and Post-Market Control
For patient-specific implants, people are the control system. Machines can make parts, but they cannot own design release, lot records, complaint handling, or Medical Device Reporting awareness. If regulatory/quality leadership, biomedical engineering, design engineering, manufacturing, and validation support are not assigned before first cases, opening slips and day-one work turns into firefighting.
The readiness check is simple: do you have SOPs, a training matrix, document control, and management review in place before the first patient file enters production? With a 3,000-unit Year 1 plan, weak staffing causes missed records, slower complaint response, and messy audits, which can shake surgeon trust fast.
Assign Owners Before First Build
Name one accountable lead for quality, one for engineering, one for production, and one for post-market follow-up. Then tie each role to training records, CAPA (corrective and preventive action), complaint intake, lot release, and the surgeon feedback loop. If a task has no owner, it will not stay on schedule when first orders start.
- Approve SOPs before first job.
- Complete the training matrix.
- Test complaint intake and escalation.
- Set document control and lot records.
- Schedule management review now.
What this hides: if a complaint lands before the team is trained, response time slows and the audit trail weakens. That can delay release decisions, hold up field fixes, and push cash needs up because rework and follow-up take staff away from shipping.
6
Related Products
- Patient-Specific Implant Manufacturing Porter's Five Forces Analysis
- Patient-Specific Implant Manufacturing BCG Matrix
- Patient-Specific Implant Manufacturing Business Model Canvas
- What Are The 5 Core KPIs For Patient-Specific Implant Manufacturing Business?
- Patient-Specific Implant Manufacturing Business Plan Template in Pre-Written Word
- How Increase Patient-Specific Implant Manufacturing Profits?
- What Are The Operating Costs Of Patient-Specific Implant Manufacturing?
- Patient-Specific Implant Manufacturing Startup Costs With $49k Monthly Overhead
- Patient-Specific Implant Manufacturing Financial Model Template in Excel
- Patient-Specific Implant Owner Income at $129M Year 1 Revenue
- How To Write A Business Plan For Patient-Specific Implant Manufacturing?
- Patient-Specific Implant Manufacturing Marketing Mix
- Patient-Specific Implant Manufacturing Marketing Plan
- Patient-Specific Implant Manufacturing Business Proposal
- Patient-Specific Implant Manufacturing PESTEL Analysis
- Patient-Specific Implant Manufacturing Pitch Deck Example Editable PPTX
- Patient-Specific Implant Manufacturing Business SWOT Analysis
- Patient-Specific Implant Manufacturing Value Proposition Canvas
Frequently Asked Questions
Start with device scope, FDA pathway, and QMS design before buying production equipment The planning case assumes 12–24+ months to open and Year 1 volume of 3,000 units Build the DICOM-to-CAD workflow, validate manufacturing, qualify sterilization and suppliers, and line up surgeon and hospital access before first commercial release