 Time to Open3-6 monthsSetup window
Time to Open3-6 monthsSetup windowStart a Pelvic Floor Physical Therapy Practice in 3–6 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open3-6 monthsSetup window  Launch Sequence8 stagesLicense first
Launch Sequence8 stagesLicense first Key BottleneckCredentialing gateApproval path
Key BottleneckCredentialing gateApproval path First Revenue StepBooked evalsReferral live
First Revenue StepBooked evalsReferral live


You’re opening a specialty physical therapy clinic where readiness matters before volume This pelvic floor PT launch plan covers licensure, treatment-room setup, compliant intake, referral outreach, scheduling, and first-revenue planning over a 60-month model period Use the checklist to confirm opening-month readiness before you book evaluations
Time to Open3-6 monthsSetup windowLaunch Sequence8 stagesLicense firstKey BottleneckCredentialing gateApproval pathFirst Revenue StepBooked evalsReferral live12-week launch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11
Legal / compliance
- License review
- Entity setup
- Compliance policies
- Consent forms
- Charting standards
Location / buildout
- Lease signed
- Room layout
- Buildout prep
- Soundproof finish
- Inspection punchlist
Equipment / supplies
- Equipment quotes
- Table install
- Biofeedback setup
- Ultrasound setup
- Supply stock
EMR / billing
- EMR select
- Templates build
- Credentialing forms
- Cash-pay setup
- Claim testing
Referrals / marketing
- Referral list
- Outreach scripts
- Clinician visits
- Lead tracking
- Launch offers
Hiring / opening ops
- PT hiring
- Coordinator onboarding
- Team training
- Soft opening
- First month review
Why test a Pelvic Floor Physical Therapy model before opening?
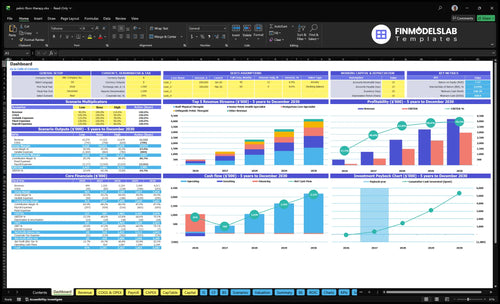
The dashboard and model tabs in the Pelvic Floor Physical Therapy Financial Model Template show revenue, costs, cash needs, assumptions, and break-even logic. Year 1 assumes 1 Senior Pelvic Health Specialist at 120 monthly treatments, $195 price, and 65% utilization; 1 Staff Physical Therapist at 140 monthly treatments, $165 price, and 60% utilization; and 1 Postpartum Care Specialist at 130 monthly treatments, $175 price, and 55% utilization. That’s about 234 treatments and $416k monthly revenue at assumed utilization; charts cover visit ramp, collections timing, payroll timing, contribution, and runway. This validates assumptions, not clinical demand by itself.
What the model highlights
- Visit ramp by month
- Billing lag and collections
- Therapist capacity by role
- Runway to break-even
What do you need to open a pelvic floor PT clinic?
To open a Pelvic Floor Physical Therapy clinic, you need launch readiness: an active state physical therapy license, scope and direct-access verification, entity formation, a 10-digit National Provider Identifier, malpractice insurance, HIPAA workflows, consent forms, pelvic exam policies, EMR, scheduling, billing, and private treatment space; see How Do I Launch Pelvic Floor Physical Therapy Business?. Specialty pelvic health training supports care quality and trust, but it’s not a universal legal certification requirement.
Must-Haves
- Hold active state PT licensure
- Verify state pelvic exam scope
- Form entity and get NPI
- Set HIPAA, consent, billing workflows
Year 1 Check
- Plan around 3 clinical roles
- Model about 234 monthly treatments
- Use private, one-on-one rooms
- Check payer and direct-access rules
How do you get first patients for a pelvic floor PT clinic?
Get your first patients by building trust before opening day: start with OB-GYNs, urogynecologists, urologists, colorectal surgeons, midwives, doulas, postpartum providers, fitness pros, and primary care groups, and support that with local search and education. For the cost side, see What Are Operating Costs For Pelvic Floor Physical Therapy?; your Year 1 load should be planned around about 234 monthly treatments across 3 clinical roles.
Trust sources first
- Start referral outreach pre-open.
- Prioritize OB-GYN and urogynecology.
- Include doulas and midwives.
- Use direct-access education where allowed.
Track what fills the schedule
- Build local service pages.
- Make booking clear and easy.
- Track referrals by source.
- Watch evaluation, conversion, and cancellations.
What is the biggest pelvic floor PT clinic launch mistake?
The biggest launch mistake in Pelvic Floor Physical Therapy is opening before the operating system is ready. That means payer status, documentation templates, pelvic exam consent, room privacy, scheduling rules, referral flow, and patient communication are still shaky. If onboarding or payer setup slips, hold insurance-heavy scheduling and start with a clear cash-pay workflow so trust doesn’t break on day one.
Launch gates
- Confirm payer status first.
- Finish documentation templates.
- Lock pelvic consent workflow.
- Check room privacy before opening.
Go-live checks
- Build a thin referral pipeline.
- Set scheduling rules clearly.
- Train patient communication scripts.
- Use a launch readiness gate.
Confirm the clinic is ready before seeing pelvic floor patients
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Compliance
- State PT licenses activeCritical
Active licenses are needed before any patient care starts.
- Entity and NPI issuedCritical
The clinic needs a legal entity and billing identity to open.
- Malpractice policy boundCritical
Coverage should be live before the first visit or consult.
Clinic setup
- Private treatment room readyHigh
Privacy matters for pelvic care and patient trust.
- Accessible table installedHigh
The room needs safe transfers and easy patient access.
- Cleaning process documentedHigh
Clear cleaning steps reduce infection risk and handoff errors.
Records and payments
- EMR templates builtHigh
Templates speed charting and keep notes consistent.
- Claims and payment vendor testedHigh
Payment flow must work before insurance or cash visits begin.
- Patient payment policy approvedHigh
Patients need clear rules on copays, self-pay, and refunds.
Staffing and scope
- Opening schedule staffedCritical
The first schedule should cover the Senior Pelvic Health Specialist, Staff PT, and Postpartum Specialist.
- Pelvic scope rules trainedCritical
Staff need clear scope lines before seeing complex cases.
- Consent and exam policy signedCritical
Written consent and exam rules protect patients and staff.
Referral intake
- Referral list builtHigh
Outreach should cover OB-GYN, urogynecology, urology, colorectal, midwife, doula, postpartum, fitness, and primary care.
- Intake forms testedHigh
Forms must collect the right history before the first visit.
- Benefits verification flow readyMedium
Insurance visits can stall if benefits checks are not ready.
Cash and signoff
- Cash runway model checkedCritical
The plan should cover the $830k minimum cash need at Month 2.
- First month budget approvedHigh
Early spend needs to fit the buildout, staff, and equipment plan.
- Go-live signoff completeCritical
Do not open if documentation, privacy, payer status, or patient flow is incomplete.
Want the six launch drivers that decide opening readiness?
1Licensure
License gatePrevents unsafe openings and cleaner claims by locking licensure, consent, privacy, and scope before bookings start.
2Care Scope
Focused scopeMakes referrals clearer by defining pelvic floor, postpartum, pain, and incontinence care from day one.
3Room Setup
Private roomsReduces opening-week friction by readying private rooms, tables, linens, cleaning, and front-desk flow.
4Billing Flow
Claims-readySpeeds first collections by lining up payer enrollment, coding, payment policies, and cash-pay steps.
5Referral Engine
Pre-openFills the schedule faster by building referral ties and search visibility before the lease opens.
6Staffing Plan
3 cliniciansSets first-week capacity so visits, templates, and admin coverage match about 234 monthly treatments.
Licensure and Compliance Readiness
Licensure and compliance readiness
You can’t safely open pelvic floor physical therapy until the clinic is legally and clinically ready. Before the first booking, confirm state PT licensure, business registration, National Provider Identifier (NPI), malpractice insurance, HIPAA policies, informed consent, pelvic exam documentation, and scope-of-practice boundaries. This is the gate between a launch date and a launch delay.
The hard part is that direct-access and payer rules vary by state. If templates, consent, and privacy workflows are built after appointments start, the clinic gets claim rework, patient confusion, and avoidable risk on day one. Safer opening starts with the paperwork already in place.
Lock the legal stack before booking
Verify the 7 core items in order, then assign one owner for payer rules and one for clinical scope. No visit should be bookable until the intake packet, privacy flow, and charting template are signed off. That keeps opening realistic and protects first-revenue claims.
- Check licensure status first.
- Confirm payer rules by state.
- Test consent before live booking.
- Use a pelvic exam note template.
- Review HIPAA and privacy steps.
Run one mock visit end to end: schedule, consent, exam note, privacy handoff, and claim-ready chart. If any step breaks, fix it before marketing starts. That reduces denial risk and closes patient communication gaps from day one.
1
Care Model and Specialty Scope
Define the Care Scope
This launch driver matters because referrals need to know exactly who to send. If the service list is fuzzy, bookings slow, patients get routed wrong, and day-one operations start with mismatched visits instead of the right pelvic health cases.
The scope should stay tight: pelvic floor dysfunction, postpartum recovery, pelvic pain, urinary incontinence, bowel dysfunction, pregnancy-related care, and related musculoskeletal issues. Year 1 staffing should reinforce that focus with a Senior Pelvic Health Specialist, Staff Physical Therapist, and Postpartum Care Specialist.
Lock the Referral List
Before opening, turn the scope into a one-page intake guide, visit menu, and referral script. That keeps clinical training, documentation, and patient education aligned so the first appointments match what the team can actually treat.
Here’s the quick check: each role should know what it treats, what it does not treat, and when to refer out. If scope control slips, the clinic can miss the assumed 234 monthly treatments target because visits fill with the wrong cases and the team spends more time reworking plans than seeing patients.
- Define visit types before booking starts.
- Train staff on scope boundaries.
- Standardize patient education materials.
- Document referral fit and exclusions.
- Keep outcomes claims factual only.
2
Location and Treatment-Room Setup
Private Room and Workflow Setup
Pelvic floor PT needs private treatment rooms, accessible exam or treatment tables, and a clean changing and draping flow to open on time. If the room layout is weak, first-day visits slow down, patient comfort drops, and staff spend time fixing setup instead of treating. The lease or room access has to be locked before equipment testing starts.
The launch kit also includes supplies, linens, cleaning protocols, and front-desk flow. The assumptions put clinical supplies and linens at 40% of Year 1 revenue, so this is a real launch cash item. Add biofeedback or therapy equipment only where it fits the care model; buying gear too early can strain cash and still leave the room not ready for patients.
Sequence the room build first
Before booking visits, verify that each room supports privacy, mobility, and simple turnover. Test the path from check-in to treatment, including changing, draping, cleaning, and exit flow. If that path breaks, the first week turns into delays and rescheduling instead of steady care.
- Confirm room access before ordering equipment.
- Set linen and cleaning restock levels.
- Train front desk on patient flow.
- Test setup with a full visit.
Keep the first open-day setup simple. If the room works with the current tables, supplies, and cleaning steps, then add specialty equipment only after the team proves the core workflow runs smoothly.
3
Payer, Billing, and Cash-Pay Workflow
Billing must be live at opening
First revenue depends on payer enrollment, claims setup, and patient payment rules more than booked visits. For a pelvic floor PT clinic, insurance-heavy launch paths need benefits verification, coding support, documentation templates, and collections steps before the first eval. Cash-pay paths need posted prices, point-of-sale collection, receipts, and patient messaging ready on day one.
At the disclosed Year 1 role prices of $195, $165, and $175, weak billing readiness can turn full schedules into delayed cash. The bottleneck is credentialing and claims readiness; if those slip, you can open the doors but still miss first collections and strain working capital.
Lock the cash path first
Before opening, map each visit type to the exact payment path: cash, insurance, or hybrid. Then test the full chain: eligibility check, charge capture, claim submission, patient balance collection, and receipt delivery. Don’t book volume until templates, codes, and payment policies are set.
- Confirm payer enrollment status
- Write payment and refund rules
- Test same-day collection flow
- Train staff on claim handoff
What this estimate hides: if claims are not ready, first-month cash depends on patient collections only, so even good demand may not cover payroll timing. Build the opening budget around billing lag, not just visit counts.
4
Referral and Patient Acquisition Engine
Build demand before opening
Referral trust has to exist before the first visit is booked. For pelvic floor physical therapy, the launch depends on outreach to OB-GYN, urogynecology, urology, colorectal, midwifery, doula, postpartum, fitness, and primary care channels, plus local search and simple booking. If that work starts after the lease is signed, the clinic can open with empty slots instead of steady demand.
The real target is about 234 monthly treatments at Year 1 assumed utilization. One line: no referrals, no day-one volume. That means the founder needs patient-facing education, workshop dates, direct-access education, and a clear booking path ready before opening month, or the clinic risks slow ramp, weak cash flow, and underused capacity.
Start outreach early
Map the referral list, then work it before launch. Track each source, who owns the relationship, when they were contacted, and what follow-up is due. The key inputs are outreach scripts, educational handouts, workshop plans, local search setup, and a simple way to book patients without friction.
Use a pre-open checklist and test it against the opening date. If referral partners only hear about the clinic after the space is ready, first-patient demand will lag. That delay can leave the schedule thin in month one, even if clinical setup is complete.
- Build referral contacts before lease completion.
- Publish local search pages early.
- Set workshop dates before opening.
- Make booking fast and simple.
- Assign one owner to follow-up.
5
Staffing, Capacity, and Scheduling
Schedule the first week before marketing starts
The launch risk here is simple: if visit lengths, eval slots, and follow-up cadence are not set before booking opens, the clinic can’t use its staff cleanly. With 1 Senior Pelvic Health Specialist, 1 Staff Physical Therapist, and 1 Postpartum Care Specialist, the Year 1 plan assumes 120, 140, and 130 monthly treatment capacity, then 65%, 60%, and 55% utilization, or about 234 monthly treatments.
That schedule only works if the intake flow, EMR templates, cancellation rule, and admin coverage are ready on day one. If those pieces are late, the first week turns into slot gaps, double booking, and patient wait-time issues, which hurts experience and makes capacity look higher than it really is.
Lock the slots before you open
Build the template first, then add patients. Define evaluation length, follow-up cadence, and same-day admin coverage before any outreach goes live, so the book matches real labor. Here’s the quick math: 120 + 140 + 130 = 390 possible monthly treatments, and at the stated utilization rates the launch plan supports 233.5, rounded to 234.
- Set eval and follow-up lengths.
- Fix the cancellation policy.
- Test EMR templates before opening.
- Assign front-desk coverage by hour.
What this estimate hides: if demand lands faster than staffing or room time, the clinic needs a waitlist and tighter visit spacing, not more marketing. If the schedule is loose, utilization falls first, and then cash timing slips.
6
Related Products
- Pelvic Floor Physical Therapy Porter's Five Forces Analysis
- Pelvic Floor Physical Therapy BCG Matrix
- Pelvic Floor Physical Therapy Business Model Canvas
- What Are The 5 KPIs For Pelvic Floor Physical Therapy Business?
- Pelvic Floor Physical Therapy Business Plan Template in Pre-Written Word
- How Increase Profits Pelvic Floor Physical Therapy?
- What Are Operating Costs For Pelvic Floor Physical Therapy?
- Pelvic Floor Physical Therapy Startup Costs: $1755K CAPEX Plan
- Pelvic Floor Physical Therapy Financial Model Template in Excel
- How Much Pelvic Floor Physical Therapy Owners Make: $115k Plus Profit
- How To Write A Pelvic Floor Physical Therapy Business Plan?
- Pelvic Floor Physical Therapy Marketing Mix
- Pelvic Floor Physical Therapy Marketing Plan
- Pelvic Floor Physical Therapy Business Proposal
- Pelvic Floor Physical Therapy PESTEL Analysis
- Pelvic Floor Physical Therapy Pitch Deck Example Editable PPTX
- Pelvic Floor Physical Therapy Business SWOT Analysis
- Pelvic Floor Physical Therapy Value Proposition Canvas
Frequently Asked Questions
Yes, a licensed physical therapist can open a pelvic floor physical therapy clinic, subject to state practice rules, business registration, malpractice coverage, and payer requirements The launch plan should also include a private treatment room, HIPAA workflows, pelvic exam consent, and documentation A practical opening range is 3–6 months when space, systems, and referrals are ready