 Owner income$115k
Owner income$115kHow Much Pelvic Floor Physical Therapy Owners Make: $115k Plus Profit

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$115k  Net margin23% → 71%
Net margin23% → 71% Revenue for target pay≈$491k
Revenue for target pay≈$491k Business difficultyHard
Business difficultyHard


Key Takeaways
- Completed visits drive revenue, not booked appointments.
- Every $10 per visit shifts annual revenue materially.
- Staffing utilization must rise as overhead stays fixed.
- Keep reserves for taxes, payroll, and growth.
Owner income$115kNet margin23% → 71%Revenue for target pay≈$491kBusiness difficultyHardWant to test your owner income case
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the model?
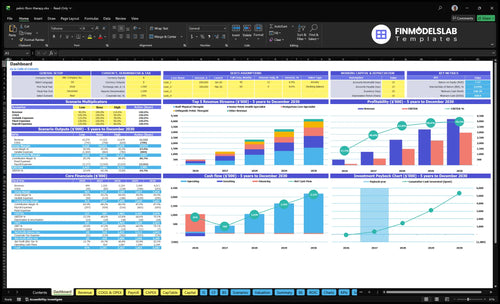
This screenshot shows dashboard, revenue assumptions, staffing, visit capacity, expenses, owner pay, reserves, and scenarios in the Pelvic Floor Physical Therapy Financial Model Template; open it to test cases.
Owner-income model highlights
- Owner pay is built in
- Revenue scales by visits
- Scenarios test cash risk
What affects pelvic floor PT practice profit margin
If you’re pricing Pelvic Floor Physical Therapy, the margin story starts with operating costs, and What Are Operating Costs For Pelvic Floor Physical Therapy? shows why a high visit price doesn’t equal profit. Gross margin is 93% in Year 1 and 94% in Year 5 before payroll, but supplies, linens, records, billing, marketing, and continuing education still take 10% of revenue in Year 1 and 7% in Year 5. With fixed overhead at $10,450 per month, a 10% drop in completed Year 1 visits cuts revenue by about $499k and contribution by about $414k.
Margin layers
- Gross margin starts at 93%.
- Year 5 gross margin is 94%.
- Payroll comes after gross margin.
- Owner take-home is lower again.
Profit risks
- $10,450 monthly fixed overhead.
- 10% Year 1 revenue goes to overhead items.
- 7% of revenue in Year 5.
- Cancelled visits hit contribution fast.
How much revenue does a pelvic floor PT practice need to pay the owner
If the owner wants $115k pay, Pelvic Floor Physical Therapy needs about $368k in annual revenue before the missing payroll items are counted. At the Year 1 modeled run rate of $499k, that leaves about $131k of cushion; if the owner target rises to $200k, required revenue is about $470k.
Break-even math
- $10,450 monthly fixed overhead
- 170% Year 1 variable burden
- $65k Practice Manager salary
- $115k owner salary target
What the cushion means
- $499k modeled Year 1 revenue
- $131k cushion vs. break-even
- $470k revenue for $200k owner pay
- Still excludes labor, taxes, debt
Is owning a pelvic floor PT practice profitable compared with being employed
Yes, owning a How Do I Launch Pelvic Floor Physical Therapy Business? practice can beat employment, but only if visit volume, pricing, utilization, and cost control hold up. The model shows $499k in Year 1 revenue and about $109k profit before associate payroll, coordinator pay, taxes, debt, and reserves, plus a modeled $115k Clinic Director and Lead PT salary. That means ownership only wins if total economic return beats salary plus risk.
Owner upside
- $499k Year 1 revenue base
- $109k pre-omission profit potential
- $115k modeled clinical salary
- 21.8% profit before omitted costs
Owner risk
- Fund patient acquisition
- Manage payroll and benefits
- Cover rent and billing
- Absorb cancellations and cash swings
Want the six owner income drivers
1
2.8K-21.4KVisit Volume
These are scenario examples, not forecasts; completed visits rise from 2,802 in Year 1 to 21,420 in Year 5, and that is the main income engine.
2
$178-$197Visit Revenue
Average revenue per visit rises from about $178 in Year 1 to about $197 in Year 5, so each slot earns more.
3
HighPayer Mix
A better payer mix lifts collected revenue per visit, which protects margin without adding labor.
4
45%-85%Utilization
Clinician utilization rises from 45% to 85% across roles, so fuller schedules spread payroll over more visits.
5
$10.45K/moOverhead
Fixed overhead is about $10,450 a month, so every extra dollar of gross profit has a direct path to take-home.
6
1-6 FTEStaffing Model
The team scales from 1 to 6 full-time equivalent roles, so hiring ahead of demand can squeeze cash and margins.
Pelvic Floor Physical Therapy Core Six Income Drivers
Completed Visit Volume
Completed Billable Visits
Owner income follows completed billable visits, not booked appointments. In this model, Year 1 runs at about 2,335 visits per month, and Year 5 at about 1,785 visits per month, so small drops in fill rate or adherence hit revenue fast.
Here’s the quick math: a 10% Year 1 volume miss means about $499k less revenue before variable cost savings. Booked isn’t paid. Cancellations, referral flow, and treatment-plan follow-through all change how much cash the owner can draw.
Protect Visit Completion
Track the gap between scheduled and completed visits each week. Use reminders, waitlists, and referral follow-up to keep the calendar full, and watch no-show rate, same-week rebooking, and plan adherence so volume loss shows up early.
- Track completed visits by clinician
- Measure cancellation and no-show rate
- Follow up referrals fast
- Use waitlists to backfill openings
1
Average Revenue Per Visit
Average Revenue Per Visit
Average revenue per visit is the cash collected per completed session, not the posted rate. In Year 1, the blended figure is about $178 and about $197 in Year 5. It moves with payer mix, deductibles, collections, and session length, with source prices of $195, $165, and $175 across visit types.
Here’s the quick math: across 2,802 Year 1 visits, every $10 change in visit revenue changes annual revenue by about $28,020. That cash then flows into profit and owner pay after labor and overhead, so small changes in realized collections can move take-home income fast.
Measure Realized Visit Revenue
Track cash collected per completed visit by payer, clinician, and visit type. Split cash pay, in-network, out-of-network, and hybrid cases so you can see what lifts the blended average without guessing from list price.
- Compare collected cash, not list price.
- Watch deductibles and denials monthly.
- Test session length against revenue.
- Review by clinician and payer mix.
If the blended average slips, owner income usually follows unless volume or margin rises enough to cover the gap.
2
Payer Mix
Payer Mix
Payer mix is the share of visits paid by cash pay, in-network, out-of-network, or hybrid plans. In pelvic floor physical therapy, it changes pricing control, referral volume, billing workload, and when cash arrives. Cash pay can simplify collections, but insurance can expand demand. Owner income tracks blended visit revenue, not the posted rate.
The model’s blended visit revenue is $178 in Year 1 and $197 in Year 5, so mix matters to take-home pay. Insurance can add allowed amounts, denials, documentation, and payment timing risk, while cash pay may limit demand in some markets. Strong care does not fix a weak payer mix.
Track Revenue By Payer
Model each payer path separately and track visits by payer, collection rate, denial rate, and days to collect. Here’s the quick math: completed visits times collected revenue per visit sets cash flow, and payer mix decides how much lands fast versus late. That timing can change the owner’s draw even when volume stays flat.
Keep payer strategy separate from clinical quality. Test cash pay, in-network, out-of-network, and hybrid cases as planning assumptions, then compare the impact on referral flow and admin load. If insurance grows referrals but adds too much billing drag, the clinic can look busy while owner pay stays tight.
3
Clinician Utilization And Staffing
Clinician Utilization And Staffing
Utilization is the share of paid clinician capacity that turns into completed visits. In Year 1, the model assumes 55% to 65% utilization across active roles, then rises to 85% in Year 5 as staffing grows from 3 therapists to 16 therapists. If utilization stays low, payroll grows faster than visit revenue, and owner take-home gets squeezed.
Here’s the quick math: more staff only helps if schedules stay full. Hiring specialized pelvic health therapists can slow expansion because recruiting and ramp-up take time, so the clinic may carry paid hours that do not yet produce enough visits. Also, separate owner labor from employee labor, or profit will look better than the cash that is actually available to pay the owner.
Track Paid Hours, Not Just Headcount
Measure utilization by role, not as one blended number. Track paid hours, completed visits, cancellation rate, and time to fill new openings so you can see where capacity is leaking. If a therapist is hired but not generating visits, that is a margin problem, not a staffing win.
Use a simple rule: forecast revenue only after loading associate clinician payroll fully, plus taxes and any paid time off. Keep owner pay separate from employee pay. One clean view of the schedule can protect cash flow better than adding another clinician too early.
- Track utilization by clinician
- Watch cancellations and open slots
- Load associate payroll fully
- Hire to demand, not hope
4
Operating Overhead
Fixed Overhead
Operating overhead is the clinic’s fixed bill stack: $10,450 per month or $125,400 per year for lease and maintenance, liability insurance, electronic health record and practice management software, utilities, legal and accounting, janitorial, and office telecom. These costs hit before owner pay, so weak visit volume cuts profit fast.
The model also carries variable overhead of 8% marketing, 2% continuing education, 4% supplies and linens, and 3% records and billing processing—17% total. The model’s fixed cost per completed visit falls from about $4,475 in Year 1 to about $585 in Year 5, and rent hurts most when utilization is low.
Track Overhead by Visit
Track overhead against completed visits, not booked visits. Here’s the quick math: fixed overhead stays at $10,450/month, so every empty slot spreads that cost over fewer visits and leaves less cash for owner draw. As utilization rises, fixed cost per visit drops and take-home income improves.
Watch three inputs each month: completed visits, fixed spend, and variable spend as a share of collections. Keep lease size, software, and admin costs aligned to volume, and review marketing, supplies, and billing fees when the schedule softens. If utiliz ation slips, overhead stays flat but cash flow tightens before profit reaches the owner.
5
Reserves, Debt, And Reinvestment
Reserves, Debt, and Reinvestment
Net profit is not the same as spendable owner income. A profitable clinic still has to hold cash for taxes, payroll buffer, continuing education, equipment, marketing, debt service, and growth, so owner distributions should come after reserve decisions and the explicit $115k owner salary.
The model shows revenue rising from $499k in Year 1 to $421M in Year 5, so working capital needs can grow fast. If onboarding takes longer than planned, cash reserve pressure rises before profit shows up in the bank, and owner pay needs to wait.
Fund reserves before owner draws
Track cash by purpose, not as one pile. Separate tax reserve, payroll buffer, debt service, and reinvestment cash so you know what is truly free for distributions. One clean rule: if the next month’s bills and the next payroll cycle are not covered, the owner draw is too high.
- Forecast collections, not booked visits.
- Ring-fence cash for taxes.
- Keep payroll and debt covered.
- Delay draws until reserves fund.
Use slower onboarding and delayed collections in the forecast. That shows whether growth is funding itself or eating the bank balance. If growth requires more clinicians, equipment, or marketing, reinvest first and pay the owner from leftover cash after debt and reserves are safe.
6
Compare lean, base, and high pelvic floor PT owner income scenarios
Owner income scenarios
Owner income moves with visit volume, price per visit, staffing mix, and fixed clinic overhead. The same clinic can look very different from Year 1 to Year 5.
| Scenario | Low CaseLean case | Base CaseBase case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the lower earnings path with tighter volume and a smaller support team. | This is the modeled middle path with stronger throughput and a fuller therapist mix. | This is the stronger earnings path with the highest visit load and the best spread of fixed costs. |
| Typical setup | About 2,802 annual visits at roughly $178 per visit drive about $499k of revenue, with lean staffing and a $10,450 monthly fixed base. | About 12,570 visits at roughly $185 per visit drive about $2.324M of revenue, with broader staffing and more support labor. | About 21,420 visits at roughly $197 per visit drive about $4.211M of revenue, with the largest team and tighter cost spread. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $109kOwner pool | $169kCore plan | $336kUpside plan |
| Best fit | Use this to stress test a slow ramp, thinner referral flow, or delayed hiring. | Use this as the main operating case for budgeting and hiring. | Use this to test what happens if demand stays strong and the clinic keeps filling capacity. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Pelvic Floor Physical Therapy Porter's Five Forces Analysis
- Pelvic Floor Physical Therapy BCG Matrix
- Pelvic Floor Physical Therapy Business Model Canvas
- What Are The 5 KPIs For Pelvic Floor Physical Therapy Business?
- Pelvic Floor Physical Therapy Business Plan Template in Pre-Written Word
- How Increase Profits Pelvic Floor Physical Therapy?
- What Are Operating Costs For Pelvic Floor Physical Therapy?
- Pelvic Floor Physical Therapy Startup Costs: $1755K CAPEX Plan
- Pelvic Floor Physical Therapy Financial Model Template in Excel
- Start a Pelvic Floor Physical Therapy Practice in 3–6 Months
- How To Write A Pelvic Floor Physical Therapy Business Plan?
- Pelvic Floor Physical Therapy Marketing Mix
- Pelvic Floor Physical Therapy Marketing Plan
- Pelvic Floor Physical Therapy Business Proposal
- Pelvic Floor Physical Therapy PESTEL Analysis
- Pelvic Floor Physical Therapy Pitch Deck Example Editable PPTX
- Pelvic Floor Physical Therapy Business SWOT Analysis
- Pelvic Floor Physical Therapy Value Proposition Canvas
Frequently Asked Questions
The model shows explicit owner compensation of $115,000 per year for the Clinic Director and Lead PT role Practice revenue is about $499,000 in Year 1 and $421 million in Year 5 Any owner distribution depends on full payroll, taxes, debt, reserves, and reinvestment, so don’t treat profit as personal cash