 Time to Open6 monthsLaunch runway
Time to Open6 monthsLaunch runwayHow To Open A Pulmonary Function Testing Center In 4–9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open6 monthsLaunch runway  Launch Sequence7 stagesValidate demand
Launch Sequence7 stagesValidate demand Key BottleneckPayer setupCredentialing delay
Key BottleneckPayer setupCredentialing delay First Revenue StepBooked PFTsPFT appointments
First Revenue StepBooked PFTsPFT appointments


Key Takeaways
- Validate referral partners before finalizing the lease.
- Signed protocols and oversight prevent opening-month compliance delays.
- Calibration, staffing, and mock tests protect launch quality.
- Billing setup must be ready before first patient visits.
Time to Open6 monthsLaunch runwayLaunch Sequence7 stagesValidate demandKey BottleneckPayer setupCredentialing delayFirst Revenue StepBooked PFTsPFT appointmentsLaunch timeline
This is a short web summary of the launch plan; the XLSX export contains the detailed Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9
Licensing and compliance
- License checklist
- Policy pack
- Safety plan
- Inspection signoff
Facility buildout
- Space layout
- Buildout bids
- Construction work
- Punch list
Equipment procurement
- Spec sheet
- Vendor quotes
- Purchase orders
- Calibration setup
Staffing and training
- Role plan
- Recruit staff
- Hire coordinator
- Mock testing
Payer credentialing
- Payer list
- File applications
- Claims setup
- Approval follow-up
Referral outreach
- Referral list
- Outreach calls
- Demo visits
- Schedule patients
Why pressure-test the Pulmonary Function Testing Center model before opening?
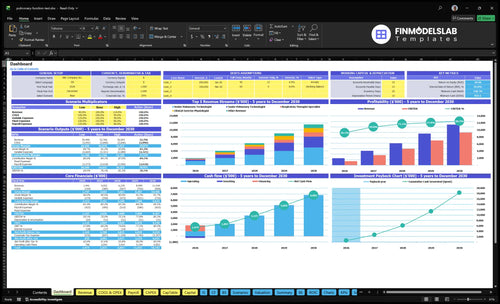
The Pulmonary Function Testing Center Financial Model Template maps revenue, costs, cash needs, assumptions, and break-even logic, so open the model.
Financial model highlights
- 484 monthly tests
- $161,760 monthly revenue
- $19,550 fixed overhead
- 19% variable load
- Watch staffing capacity
- Flag referral ramp
How long does it take to open a pulmonary function testing center?
A Pulmonary Function Testing Center usually takes 4 to 9 months to open, and the clock is driven by lease and buildout, equipment delivery and validation, staff hiring, payer credentialing, and referral setup. The biggest delays are often payer files, missing calibration logs, weak referral demand, or hiring gaps. First revenue starts with booked reimbursable appointments, not just an open door.
What sets the pace
- 4 to 9 months is the usual window.
- Lease and buildout can stretch timelines.
- Equipment validation needs clean logs.
- Payer credentialing can block billing.
What to do early
- Start payer enrollment early.
- Order long-lead equipment before marketing.
- Hire senior pulmonary technologists first.
- Run workflow rehearsals before opening month.
What do you need to start a pulmonary function testing center?
To start a Pulmonary Function Testing Center, you need medical oversight, state-specific healthcare compliance review, validated testing equipment, trained technicians, payer setup, and clean referral-to-report workflows before opening; this How To Launch Pulmonary Function Testing Center? guide fits that launch order. Demand is real: the Centers for Disease Control and Prevention reports about 16 million US adults have chronic obstructive pulmonary disease and about 27 million people have asthma, but revenue starts only when test orders, reimbursement, and reporting are ready.
Core setup
- Form the entity and bank account
- Review state healthcare rules first
- Secure clinical space and infection control
- Set signed physician oversight protocols
Opening readiness
- Validate spirometry and calibration supplies
- Train technicians and medical interpreters
- Set HIPAA, OSHA, EHR, and billing workflows
- Schedule reimbursable referrals before launch
What launch mistakes hurt a pulmonary function testing center?
For a Pulmonary Function Testing Center, the biggest launch mistake is opening before payer approval and signed referral interest are in place; that can turn busy days into unpaid work. Millions of Americans need faster breathing tests, but demand on paper is not the same as reimbursable bookings. If equipment, staffing, payer files, and referral intake do not line up, hold the launch.
Launch mistakes
- Open before payer approval.
- Count demand without signed referrals.
- Skip dry runs and mock visits.
- Use weak calibration workflows.
Readiness checks
- Run mock patient visits.
- Test claim submission logic.
- Confirm physician interpretation review.
- Hold launch if reimbursable appointments are not ready.
Confirm what must be ready before seeing PFT patients
Launch readiness checklist
Use this go-live approval checklist to confirm the pulmonary function testing center is ready before opening.
Regulatory
- Entity registration confirmedCritical
The clinic needs a legal entity before contracts, banking, and payer work can move forward.
- Clinic permits clearedCritical
Local clinic permissions must be in place before patient testing starts.
- Privacy and safety policies readyCritical
Written privacy and workplace safety rules reduce launch risk and staff confusion.
Clinical
- Medical director assignedCritical
A named clinical lead is needed for oversight, interpretation workflow, and escalation.
- Interpretation workflow signedCritical
Tests cannot go live without a clear read, review, and escalation path.
- Referral criteria documentedHigh
Clear referral rules keep ordering providers aligned on who should be tested.
Equipment
- Testing systems installedCritical
Spirometry and related systems must work before the first patient is booked.
- Calibration logs readyCritical
Calibration proof protects test accuracy and supports audit review.
- Service contracts activeHigh
Service coverage keeps the body plethysmograph, modules, and IT systems online.
Staff
- Technologists hiredCritical
The Year 1 plan needs senior, junior, and specialist coverage from day one.
- Staff competency trainedCritical
Training should cover test steps, infection control, and patient handling.
- Coverage schedule setHigh
The roster must match the forecasted staffing plan and avoid first-week gaps.
Payer
- Payer enrollment activeCritical
Without payer enrollment, tests may be delayed or unpaid.
- Claims workflow testedCritical
Billing must handle coding, submission, and follow-up before opening.
- Denial checks setHigh
Denial review protects cash and helps catch missing authorization or coding errors.
Finance
- Cash runway reviewedCritical
The model shows minimum cash of $837k in Month 2, so runway must be funded.
- Year 1 model approvedCritical
Use Year 1 utilization, 19% variable load, and $19,550 overhead to test launch risk.
- Go-live signoff completeCritical
Final signoff should confirm compliance, staffing, equipment, payer, and billing are ready.
Want to see the six launch drivers for a PFT lab?
1Referral Demand
484/moNamed referral partners and weekly outreach are the main gate to reaching 484 monthly tests in Year 1.
2Clinical Compliance
Signed SOPsSigned protocols, privacy steps, and interpretation rules reduce rework and keep first claims cleaner.
3Equipment Readiness
Cal logsCalibration logs, service contacts, and stocked disposables protect report quality and avoid opening-day delays.
4Qualified Staffing
2-1-1 mixYear 1 needs 2 seniors, 1 junior, 1 specialist, and 1 assistant to keep tests accurate and steady.
5Billing Readiness
4% feesPayer enrollment, CPT setup, and clean templates shorten the cash gap after the first reimbursable tests.
6Day-One Workflow
55-70%Dry runs, timed rooms, and clear handoffs keep day-one capacity usable without slowing reports.
Referral Demand Validation
Referral Demand Gate
For a pulmonary function testing center, demand is the first go/no-go. If you sign a lease before you have named referral partners, expected order types, a scheduling path, and first-month appointment targets, you can open on time and still sit idle. The real risk is simple: equipment is ready, but test orders are not, so the ramp to 484 monthly tests at utilization slows fast.
That gap hits cash and day-one service. Rent, staff, calibration, and reporting costs start immediately, but revenue only starts when pulmonologists, primary care groups, allergists, sleep practices, occupational medicine, and employer health programs send work. A physician liaison making weekly referral visits before launch is the cleanest way to prove volume before doors open.
Pre-Open Referral Proof
Validate demand before you finalize the lease if you can. Get written or named commitments, the test types each source will send, and the booking rules for urgent versus routine orders. If the first month’s schedule target is vague, the launch plan is too. Here’s the quick check: can staff book real patients, not just “interest”?
- Named referral partners
- Expected order types
- Scheduling process
- First-month appointment targets
- Weekly pre-launch referral visits
What this hides: a strong pipeline still needs follow-through. If referral intake is slow or no one owns outreach, opening day can look busy on paper but thin in the schedule. That pushes out utilization and leaves the clinic paying for unused capacity.
1
Clinical Compliance And Medical Oversight
Clinical Oversight Readiness
For a pulmonary function testing center, opening can slip if the medical director, physician interpretation workflow, and written testing protocols are not locked before day one. You need clear turnaround rules, because delayed reports slow treatment decisions and create first-month rework.
This driver also covers Health Insurance Portability and Accountability Act (HIPAA) privacy safeguards, Occupational Safety and Health Administration (OSHA) procedures, infection control, and state healthcare rules. If documentation does not match payer rules, billing gets messy; the Year 1 model already carries 4% of revenue for billing and claims processing, so avoid adding preventable correction work.
Lock the Workflow Before the First Patient
Before opening, get signed protocols, privacy steps, staff training logs, and an incident escalation path in one place. Then run a dry test from referral intake to signed report so the team can catch gaps in charting, cleaning, or review steps before real patients arrive.
- Confirm physician review timing.
- Document privacy handling steps.
- Train staff on escalation rules.
- Test payer-ready templates.
The risk is not just compliance trouble; it is delayed reporting, denied claims, and opening-month rework. With modeled role utilization at 55% to 70%, the clinic needs fast, repeatable workflows so paid capacity is not lost to manual fixes.
2
Equipment And Calibration Readiness
Equipment and Calibration Readiness
This launch driver matters because a pulmonary function testing center cannot open on time without spirometry, lung volume, and diffusing capacity of the lungs for carbon monoxide testing gear set up and validated. If bronchodilator testing is offered, that adds another setup step. The opening risk is simple: equipment can sit in the room, but if calibration, validation, or service support is incomplete, you still cannot test patients safely on day one.
Here’s the quick check: you need documented calibration logs, maintenance contacts, staff competency signoff, and successful mock tests before first patient flow starts. Missing a calibration syringe, testing gas, filters, or other disposables can block opening just as much as a late delivery. Year 1 supply planning should assume 65% disposable medical supplies and 35% testing gas and calibration kits, so cash and reorders are not an afterthought.
Pre-Open Equipment Checks
Build the launch sequence around what must be in the room, tested, and documented before scheduling the first visit. That means equipment delivery confirmed, service contracts active, consumable inventory on hand, and staff able to run mock tests without help. If validation fails, you delay opening; if disposables are short, you may open but lose patient slots and frustrate referring clinicians.
Use a simple readiness list and close each item before setting a first-day schedule.
- Confirm delivery for all test systems.
- Verify calibration and maintenance logs.
- Stock filters, gas, syringes, supplies.
- Sign off staff competency on each test.
- Run mock tests and fix errors.
That setup supports reliable patient flow and cleaner reports from day one, which is the real opening requirement here.
3
Qualified Staffing And Competency
Staffing And Competency
A pulmonary function testing center can’t open cleanly without the right team on day one. The Year 1 plan calls for 2 senior pulmonary technologists, 1 junior pulmonary technologist, 1 respiratory therapist specialist, 0 clinical exercise physiologists, and 1 testing assistant, for 760 monthly tests before utilization. If experienced staff are missing, capacity drops and first-patient days get messy.
The real launch risk is not headcount alone; it’s competency. Readiness means competency signoff, strong patient instruction, tight quality control habits, and a clean interpretation handoff process. If these are weak, you get more retests, slower room turnover, and delayed reports, which hurts the clinic’s first weeks and can push opening back.
Hire, Train, Verify
Before opening, confirm each role can run a full test cycle and explain patient prep clearly. Document signoff for instruction, calibration checks, and QC steps, then run mock days with all 5 staff roles in place. One clean dry run is better than a rushed opening with gaps in handoff or test quality.
Sequence hiring around the hardest seat first: experienced technologists and the respiratory therapist specialist. That lowers the chance of launch delays from hard-to-hire staff and protects day-one throughput. If training is still open when the first referrals arrive, expect slower intake, more retests, and a weaker start.
4
Payer Credentialing And Billing Readiness
Payer Credentialing and Billing Readiness
If you open before payer enrollment, Current Procedural Terminology setup, and documentation rules are live, you can see patients but still stall on cash. For a pulmonary function testing clinic, the launch risk is billing lag, not just clinical delay, because claims must match referral orders, test notes, and payer rules from day one.
The year-one model assumes 4% of revenue goes to billing and claims processing fees, so the setup has to be clean before the first reimbursable test. Readiness is approved payer participation or a clear cash-pay and out-of-network policy, plus a tested claim workflow. That shortens the cash-flow gap after launch and cuts denial rework.
Set billing before the first patient
Start payer enrollment early, then lock the billing map: test codes, referral order rules, chart templates, claim submission steps, denial follow-up, and payment timing. Keep the team aligned on what gets documented before the test, during the test, and at sign-off so claims can move without manual fixes.
- Verify payer status before opening.
- Test claims with sample encounters.
- Use clean documentation templates.
- Train staff on referral order rules.
- Set denial prevention checks early.
Here’s the quick math: if billing isn’t ready, the clinic can still operate clinically, but cash can lag after the first reimbursable tests. The real bottleneck is seeing patients before claims can be submitted cleanly, which puts pressure on working capital right when patient volume starts.
5
Operating Workflow And Day-One Capacity
Day-One Workflow
Opening on time depends on whether the clinic can move each patient through referral intake, order review, scheduling, pre-test instructions, contraindication checks, room turnover, cleaning, calibration, test performance, physician interpretation, reporting, and follow-up without breaking the chain. With Year 1 modeled utilization at 55% to 70% by role and 0 clinical exercise physiologist staff, the launch risk is schedule congestion, not demand.
One slow step can block the next patient and shrink usable capacity even when rooms and equipment are ready. The day-one test is simple: can the team finish a timed visit, issue the report, and send follow-up communication fast enough to keep the schedule moving without losing accuracy.
Timed Dry Runs
Run full dry runs before the first patient day and time every handoff. Use clear staff roles, real appointment slots, and the same sequence you will use live so you can catch delays in intake, cleaning, calibration, and report turnaround before they hit patients.
- Assign one owner per workflow step.
- Time each appointment from intake to report.
- Set report turnaround rules before opening.
- Build buffer for room turnover.
6
Related Products
- Pulmonary Function Testing Center Porter's Five Forces Analysis
- Pulmonary Function Testing Center BCG Matrix
- Pulmonary Function Testing Center Business Model Canvas
- What 5 KPIs Should Pulmonary Function Testing Center Track?
- Pulmonary Function Testing Center Business Plan Template in Pre-Written Word
- How Increase Profitability Pulmonary Function Testing Center?
- What Are Operating Costs Of Pulmonary Function Testing Center?
- Pulmonary Function Testing Center Startup Costs: $263K CAPEX Plan
- Pulmonary Function Testing Center Financial Model Template in Excel
- How Much a Pulmonary Function Testing Center Owner Can Make at 484 Tests/Month
- How To Write A Pulmonary Function Testing Center Business Plan?
- Pulmonary Function Testing Center Marketing Mix
- Pulmonary Function Testing Center Marketing Plan
- Pulmonary Function Testing Center Business Proposal
- Pulmonary Function Testing Center PESTEL Analysis
- Pulmonary Function Testing Center Pitch Deck Example Editable PPTX
- Pulmonary Function Testing Center Business SWOT Analysis
- Pulmonary Function Testing Center Value Proposition Canvas
Frequently Asked Questions
Start by validating physician referral demand, then line up clinical space, equipment, staff, payer setup, and medical oversight A practical launch often takes 4 to 9 months The Year 1 planning case uses 2 senior technologists, 1 junior technologist, 1 respiratory therapist specialist, and 1 testing assistant to support about 484 modeled monthly tests at utilization