 Owner income$1.15M
Owner income$1.15MHow Much a Pulmonary Function Testing Center Owner Can Make at 484 Tests/Month

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$1.15M  Net margin59.1%
Net margin59.1% Revenue for target pay$1.94M
Revenue for target pay$1.94M Business difficultyMedium
Business difficultyMedium


Key Takeaways
- Completed tests drive revenue, with break-even near 169 monthly.
- Each test adds about $271 after variable costs.
- A $25 reimbursement shift moves revenue $12,100 monthly.
- Collections and staffing discipline protect owner take-home.
Owner income$1.15MNet margin59.1%Revenue for target pay$1.94MBusiness difficultyMediumWant to test your PFT lab profit calculator?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
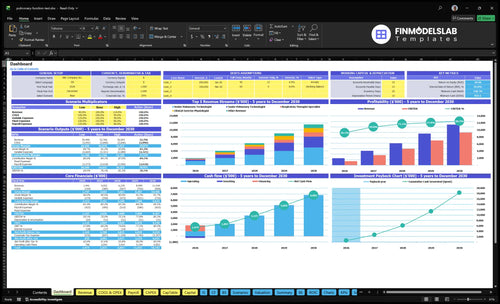
How do you check owner income in the Pulmonary Function Testing Center model?
This screenshot ties test volume, reimbursement, staffing, overhead, and reserves to revenue, gross profit, operating profit, and owner pay capacity in the Pulmonary Function Testing Center Financial Model Template; open the model to review the assumptions.
Owner-income model highlights
- Owner pay capacity
- Break-even tests
- Margin assumptions
Can a pulmonary function testing center owner make $100k?
Yes, a Pulmonary Function Testing Center can make $100k/year for the owner under the provided Year 1 model; see How To Launch Pulmonary Function Testing Center? for launch context. Here’s the quick math: $100k/year is $8,333/month, and with $271 contribution per completed test against $45,633/month in fixed costs plus listed payroll, owner-pay break-even is about 200 tests/month versus base volume of 484 tests/month.
Owner-Pay Math
- $100k/year target owner pay
- $8,333/month required draw
- $271 contribution per completed test
- 200 tests/month break-even with owner pay
Key Caveats
- 484 tests/month base volume
- Excludes reserves, taxes, and debt
- Excludes startup costs and reinvestment
- Added wages raise needed volume
Is a pulmonary function testing center profitable?
A Pulmonary Function Testing Center can be profitable, but only if utilization and collections cover the fixed clinical base. In the provided Year 1 case, 484 tests/month support $194M revenue and $102M operating profit before exclusions, and break-even is about 169 tests/month before owner pay. The simple risk is idle capacity: if rooms, staff, and equipment sit quiet, profit drops fast.
Profit drivers
- 484 tests/month supports scale.
- 169 tests/month is break-even.
- Collection quality protects cash flow.
- Higher utilization spreads fixed costs.
Operating risks
- Owner-run models mix labor and profit.
- Manager-run models need tighter referrals.
- Idle rooms weaken standalone viability.
- Staff and equipment must stay busy.
How much revenue does a pulmonary function testing center make?
A Pulmonary Function Testing Center can make about $161,760/month in Year 1 from 484 completed tests, or about $1.94M/year. By Year 2, revenue can rise to $337,680/month from 982 tests, and Year 3 can reach $519,180/month from 1,404 tests.
Here’s the quick math: collected revenue averages about $334/test, but the real number shifts with payer contracts, referral sources, no-shows, test mix, and collections. Revenue is not owner income, because variable costs, fixed overhead, payroll, reserves, taxes, and debt still come out.
Main revenue drivers
- Completed tests drive sales.
- Year 1 reaches $161,760/month.
- Year 2 reaches $337,680/month.
- Year 3 reaches $519,180/month.
What cuts into cash
- No-shows lower completed volume.
- Payer contracts change collected dollars.
- Test mix changes revenue per visit.
- Overhead and payroll still get paid.
Want to see the main PFT clinic profit drivers?
1
484 vs 169Test Volume
At 484 tests a month versus 169 at break-even, each extra completed test pushes more revenue past fixed costs and into owner income.
2
$334/testCollected Reimbursement
Average collected pay per test sets the top line, and payer mix can lift or cut take-home fast.
3
$26.1KStaff Productivity
With $26,083 of listed payroll, idle hours and underused labor hit margin hard, while tighter scheduling protects income.
4
$19.6KFixed Overhead
The $19,550 monthly overhead sets the cash floor, so lease and admin control matter even when volume is strong.
5
169/moReferral Pipeline
A steady referral flow keeps slots filled, and concentration in a few sources raises no-show and volume risk.
6
4% feeBilling Collections
Billing fees and slower cash collections trim realized income, even when tests are booked and completed.
Pulmonary Function Testing Center Core Six Income Drivers
Completed Test Volume
Completed Test Volume
If the calendar looks full but the tests do not get completed, income does not move. For a pulmonary function testing (PFT) center, the real driver is completed, billable tests, not scheduled visits. At 484 completed tests/month in Year 1, the center is well above the 169 tests/month break-even line before owner pay.
Here’s the quick math: at a $334 average revenue per test and 19% variable cost, each extra completed test adds about $271 in contribution. No-shows, cancellations, room capacity, and technician availability reduce usable volume, so income rises only when more scheduled visits become paid tests.
Measure Show Rate, Not Just Schedule Fill
Track scheduled visits, completed tests, and same-day cancellations every week. The key input is the conversion from booked slots to billable tests, because that is what spreads fixed overhead and payroll across more revenue. If completions slip, owner cash drops fast even when the schedule still looks busy.
Manage the bottlenecks that cut volume: technician coverage, room time, and patient no-shows. A simple target is to keep completions safely above 169 tests/month, since every test above that point adds about $271 before owner pay. That makes fill rate a direct profit lever, not just an ops metric.
- Track booked-to-completed conversion.
- Watch no-shows by referral source.
- Match staffing to peak test hours.
- Limit idle room time.
1
Average Collected Reimbursement
Average Collected Reimbursement
This driver is the cash collected per completed pulmonary function test, not the billed charge. Year 1 uses about $334/test on 484 tests/month, with service prices ranging from $120 for testing assistant work to $550 for clinical exercise physiologist work.
Payer mix, Medicare share, commercial contracts, patient responsibility, and collections performance move the average. Here’s the quick math: a $25 change in collected reimbursement across 484 monthly tests changes revenue by $12,100/month before cost effects, so owner pay can swing fast even when volume stays flat.
Track Cash per Test
Measure collected cash by payer, test type, and claim status. If one payer or service line drags the average below $334/test, the clinic may still look busy while take-home income falls. The real input set is simple: completed tests, mix of payers, contract rates, patient balances, and denial rates.
- Cash collected per test
- Medicare versus commercial mix
- Patient responsibility collected
- Denied or underpaid claims
Push hard on clean claims and patient collection at the point of service. A small lift in collected reimbursement drops straight into gross margin, and with fixed staff and rent already in place, that extra cash is what funds owner draw.
2
Staffing Productivity
Staffing Productivity
Staffing productivity is the share of paid clinical time that turns into billable PFT work. In Year 1, the model assumes 2 senior pulmonary technologists at 65%, 1 junior technologist at 60%, 1 respiratory therapist specialist at 55%, and 1 testing assistant at 70%. That matters because the clinic carries labor cost before every room is full, so weak utilization cuts margin and lowers what the owner can take home.
The overhead pressure is real: listed payroll adds $26,083/month for the medical director, clinic manager, physician liaison, and patient coordinator roles. If staffing stays underused, profit gets squeezed even when demand exists. Here’s the quick math: higher completed-test throughput spreads the same payroll across more billable volume, while low room fill leaves more cost sitting idle.
Track Utilization by Role
Measure tests per paid clinical hour and watch each role’s fill rate against its target: 65%, 60%, 55%, and 70%. Also track no-shows, open slots, and same-week rebookings, because empty capacity hits margin fast. If a role runs below plan, reduce idle time, tighten scheduling, or match staff hours to referral flow so payroll turns into collected revenue.
Use a simple rule: if payroll rises faster than completed tests, owner pay falls. The key input is not headcount alone; it’s paid time that lands on billable tests. When admin support like the $26,083/month payroll block is kept aligned with actual volume, the clinic protects cash flow and leaves more room for owner draw.
3
Fixed Overhead and Equipment
Fixed Overhead Floor
A pulmonary function testing center starts with a $19,550/month fixed overhead floor before owner pay. That includes $12,500 lease, $2,800 equipment maintenance, $1,200 software, $1,500 liability insurance, $950 utilities and biohazard waste, and $600 admin costs. Equipment price matters, but monthly carrying costs and financing obligations decide how fast cash gets eaten.
Here’s the quick math: at 169 tests/month, fixed overhead is about $116 per test; at 484 tests/month, it drops to about $40 per test. So income improves when volume spreads the same rent and service bills across more completed tests, and it weakens fast if utilization slips.
Track Fixed Cost per Test
Track fixed overhead by line item each month, then divide by completed tests. Watch lease, maintenance, software, insurance, utilities, and admin separately so you can see which cost is drifting. If a vendor hike or equipment repair lifts the floor, owner take-home falls unless test volume rises with it.
- Use completed tests, not scheduled visits.
- Recast cost per test monthly.
- Flag lease or maintenance jumps fast.
- Model financing before buying equipment.
What this estimate hides: downtime, calibration gaps, and low room use. If the clinic stays near the 169-test break-even line, every fixed dollar matters; above that line, each added test turns more of the overhead into profit and cash for the owner.
4
Referral Pipeline
Referral Pipeline
Referral pipeline is what turns open clinic capacity into billable PFT volume. At a Year 1 run rate of $161,760/month in collected revenue, physician liaison outreach runs at 5% of revenue, or about $8,088/month, plus a $75,000 annual liaison salary. That spend only helps if pulmonology, primary care, occupational health, and pre-op channels keep tests coming in.
The risk is concentration. If one referral source drives most of the schedule and then drops off, completed tests can slide toward the 169-test monthly break-even line. Spread referrals across several sources so one lost relationship does not crush utilization, margin, or the owner’s draw.
Track source mix, not just total referrals
Measure referrals by source, completed tests by source, and referral-to-test conversion. That tells you which channels actually pay for the 5% outreach spend and the $75,000 liaison role. One clean rule: if a source is over 40% of volume, treat it as a cash-flow risk, not a strength.
- Track monthly volume by source
- Watch conversion from referral to test
- Flag cancellations by source
- Grow weak channels before one fails
If liaison activity rises but completed tests do not, owner income drops because fixed costs stay put while revenue stalls. Forecast the schedule by source, then test which channels fill rooms fastest and with the fewest no-shows.
5
Billing Collections
Billing Collections
Billing collections decide how much testing turns into cash. On $161,760 of revenue, Year 1 billing and claims processing fees are about 4%, or $6,470/month. That cost sits on top of the bigger issue: owner income follows collected cash, not gross charges.
Even a small leak matters. A 1% collection miss equals about $1,618/month or $19,411/year. Documentation, prior authorization, coding accuracy, claim follow-up, and patient collections drive denial risk and cash timing, so weak billing can shrink pay even when test volume looks fine.
Track Cash, Denials, and Days to Collect
Measure collected revenue per test, denial rate, and days in accounts receivable. Here’s the quick math: if collections drop by 1%, cash falls by about $19.4k/year, before any cost changes. That is money that would have supported overhead, debt service, and owner draw.
Keep the process tight on the front end and the back end. Use clean documentation, confirm authorization before service, code the right test, and follow unpaid claims fast. One clean rule helps: if it is not collected, it does not pay the owner.
- Track collected cash, not billed charges
- Watch denials by payer
- Review patient balances weekly
- Fix missing auth before testing
6
Compare lean, base, and high PFT lab profit scenarios
Owner income scenarios
Owner income moves with test volume, price per test, staffing mix, and fixed clinic costs. This model turns profitable early, but higher utilization drives the real upside.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | This is the lower earnings path, with Year 1 ramp and partial clinic use. | This is the modeled middle path, with Year 2 scale and steadier throughput. | This is the stronger earnings path, with Year 3 utilization and fuller clinic loading. |
| Typical setup | About 484 tests a month at about $334 per test, with 19% variable costs, listed payroll, and EBITDA near $1.15M. | About 982 tests a month at about $344 per test, with 17.8% variable costs, listed payroll, and EBITDA near $2.84M. | About 1,404 tests a month at about $370 per test, with 16.7% variable costs, listed payroll, and EBITDA near $4.68M. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $1.1M - $1.2MYear 1 ramp | $2.8M - $2.9MYear 2 scale | $4.6M - $4.7MUpside case |
| Best fit | Use this if referrals build slowly or the clinic stays under full utilization. | Use this as the budget case for steady referral flow and stable staffing. | Use this to test what happens if referral volume stays strong and capacity keeps rising. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distribution guidance.
Related Products
- Pulmonary Function Testing Center Porter's Five Forces Analysis
- Pulmonary Function Testing Center BCG Matrix
- Pulmonary Function Testing Center Business Model Canvas
- What 5 KPIs Should Pulmonary Function Testing Center Track?
- Pulmonary Function Testing Center Business Plan Template in Pre-Written Word
- How Increase Profitability Pulmonary Function Testing Center?
- What Are Operating Costs Of Pulmonary Function Testing Center?
- Pulmonary Function Testing Center Startup Costs: $263K CAPEX Plan
- Pulmonary Function Testing Center Financial Model Template in Excel
- How To Open A Pulmonary Function Testing Center In 4–9 Months
- How To Write A Pulmonary Function Testing Center Business Plan?
- Pulmonary Function Testing Center Marketing Mix
- Pulmonary Function Testing Center Marketing Plan
- Pulmonary Function Testing Center Business Proposal
- Pulmonary Function Testing Center PESTEL Analysis
- Pulmonary Function Testing Center Pitch Deck Example Editable PPTX
- Pulmonary Function Testing Center Business SWOT Analysis
- Pulmonary Function Testing Center Value Proposition Canvas
Frequently Asked Questions
Using the provided Year 1 assumptions, operating profit is about $102M before reserves, taxes, debt, startup costs, and owner distributions That comes from 484 completed tests per month, $334 average collected revenue per test, and $194M annual revenue Actual owner take-home depends on reserves, debt service, reinvestment, and any costs not separately modeled