 Time to Open1 monthSetup window
Time to Open1 monthSetup windowHow To Launch Radiofrequency Ablation Clinic?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open1 monthSetup window  Launch Sequence8 stagesLicense first
Launch Sequence8 stagesLicense first Key BottleneckCredentialing gatePayer approval
Key BottleneckCredentialing gatePayer approval First Revenue StepAuthorized caseClaim ready
First Revenue StepAuthorized caseClaim ready


You’re opening a procedure business, not just a medical office, so launch readiness has to cover licensing, facility setup, equipment, staffing, payer setup, and referrals This radiofrequency ablation (RFA) clinic launch plan uses a Month 1 to Month 60 model period, with Year 1 starting at 1 cardiac electrophysiologist, 1 interventional pain physician, 1 nurse practitioner, 2 registered nurses, and 1 radiology technician The practical next step is to validate Month 1 readiness before scheduling the first reimbursable procedure
Time to Open1 monthSetup windowLaunch Sequence8 stagesLicense firstKey BottleneckCredentialing gatePayer approvalFirst Revenue StepAuthorized caseClaim readyLaunch timeline
This short web summary shows the launch workstreams, and the XLSX export contains the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10
Licensing / compliance
- Apply permits
- Secure malpractice
- Physician credentialing
- Complete accreditation
- Waste plan signoff
Facility buildout
- Finalize room layout
- Complete buildout
- Install sterilization suite
- Set patient flow
- Power backup check
- Procedure room signoff
Equipment / IT
- Order RFA system
- Set up EHR
- Install mapping system
- Validate C-arm
- Test billing software
Staffing / training
- Hire core team
- Train procedure staff
- Run mock cases
- Set call coverage
- Readiness checklists
Payer setup
- Submit payer packets
- Load fee schedules
- Test claim edits
- Confirm payment cycle
Referral marketing
- Build referral list
- Meet referral sources
- Launch patient intake
- Schedule first cases
- Open go-live review
Why does a Radiofrequency Ablation Clinic need a model before launch?
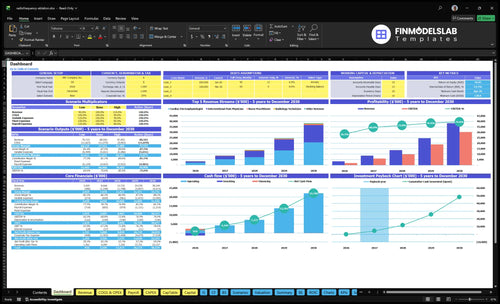
This screenshot shows revenue, costs, cash needs, and breakeven logic; open the Radiofrequency Ablation Clinic Financial Model Template.
Financial model highlights
- Staffing sets $386k overhead
- $285k monthly revenue
- 45/50/40-50 capacity mix
- 45% variable costs total
- Payer timing shifts runway
- Procedure ramp sets breakeven
How long does it take to open an RFA clinic?
There isn’t a guaranteed opening date for a Radiofrequency Ablation Clinic; it depends on lease signing, room buildout, equipment delivery, physician credentialing, payer enrollment, hiring, and inspection readiness. The model starts operations in Month 1, but it does not give a pre-opening week count. The biggest bottlenecks are payer credentialing, prior authorization, equipment validation, and clinical protocol approval, and cardiac ablation can take longer than a pain-only rollout.
What slows opening
- Lease and buildout set timing.
- Equipment delivery can slip launch.
- Credentialing blocks early revenue.
- Protocol approval must clear first.
Month 1 fixed items
- $185k rent is live.
- $42k maintenance starts.
- $98k malpractice starts.
- $15k EHR starts.
What mistakes create RFA clinic launch risks?
The biggest launch risks for a Radiofrequency Ablation Clinic are simple: start only when credentialing, equipment, prior authorizations, billing, staff training, and emergency drills are ready, or you’ll get idle physicians, canceled cases, denied claims, and unsafe patient flow. Here’s the quick math: with $185k rent, $98k malpractice, and $42k equipment maintenance each month, delays burn $325k monthly before the first case. No first cases until the readiness gate is passed.
Launch mistakes
- Underestimate credentialing time
- Order RFA equipment late
- Open without referral demand
- Miss prior authorization workflows
Day-one failure points
- Weak emergency protocols
- Late staff training
- Incomplete billing setup
- Test staff, equipment, documentation
How do you get patients for an RFA clinic?
Get patients for a Radiofrequency Ablation Clinic by starting with clinically appropriate referrals from orthopedic, spine, neurology, primary care, and cardiology networks, then add payer directories, local search, and patient education; for profit math, see How Increase Radiofrequency Ablation Clinic Profits? Keep patient acquisition and referral marketing near 3% of revenue in Year 1, then 2% by Year 4 and Year 5. First revenue should come from an authorized, documented, reimbursable procedure, not an unverified consult pipeline.
Referral routes first
- Build specialist referral lanes
- Use payer directories next
- Publish simple patient education
- Track 3% Year 1 spend
Fast intake wins
- Collect records before visits
- Check imaging fast
- Verify benefits and prior auth
- Schedule only reimbursable cases
Build a launch-gating checklist for opening an RFA clinic
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Regulatory
- Entity and licensure verifiedCritical
Confirms the clinic can operate and bill without licensure gaps.
- Medical director structure approvedCritical
Keeps clinical oversight clear before the first procedure.
- Malpractice policy boundCritical
Protects the balance sheet if a claim or procedure is challenged.
- Controlled-substance rules reviewedHigh
This avoids storage, prescribing, or logging errors if those drugs are used.
- Accreditation path documentedHigh
Shows the clinic knows what proof is needed before opening and payer review.
Facility
- Procedure rooms clearedCritical
Room layout must support safe ablation workflow and access.
- Recovery space readyHigh
Patients need a monitored recovery path before discharge.
- Sterile flow approvedCritical
Clean flow cuts infection risk and inspection issues.
- Waste and utilities setHigh
Waste pickup and utilities must support daily operations.
Equipment
- RFA generator installedCritical
Core ablation gear has to work before the first case.
- Catheter reorder points setHigh
Stock levels prevent delays when case volume rises.
- Imaging and monitors testedCritical
Imaging and monitoring must pass a live test.
- Maintenance contract activeHigh
Service coverage keeps downtime from stopping procedures.
Staffing
- Month 1 core staff hiredCritical
Year 1 staffing starts at 1 electrophysiologist, 1 pain physician, 1 NP, 2 RNs, and 1 tech.
- Clinical competencies signedCritical
Signed skills show the team can work safely before live cases.
- Emergency drills completedHigh
Drills reduce delay if a patient decompensates.
- Scheduling coverage builtHigh
Coverage avoids bottlenecks in clinic hours.
Revenue
- Referral intake liveCritical
Patient intake must route referrals without manual chaos.
- Payer enrollment filedCritical
Claims cannot start until payer enrollment is in process or done.
- Pricing and authorizations setHigh
Preauth and price checks stop denials at the front end.
- Claims workflow testedCritical
Test claims show coding and claim edits are working.
Finance
- Opening cash runway checkedCritical
Cash needs to cover the Month 4 low point in the model.
- First-month spend approvedHigh
Spend approval keeps capex and payroll inside plan.
- Go-live signoff completeCritical
Final signoff confirms the team, site, and billing are ready.
Want the six main RFA clinic launch drivers?
1Compliance and Credentialing
License gateLicensure, malpractice, and payer setup let referrals convert into reimbursable cases instead of denied claims.
2Procedure-Room Readiness
Room readyA ready room supports safe first cases, smoother inspections, and fewer launch delays.
3Equipment and Vendor Setup
Vendor liveInstalled generators, kits, and training keep scheduled procedures from getting canceled at go-live.
4Clinical Staffing and Workflow
6-person teamThe Year 1 team supports safe throughput, documentation, and reimbursement without hiring after referrals arrive.
5Referral Pipeline and Intake
3% revReferral flow and intake turn outside interest into authorized cases, not empty calendars.
6Billing and Revenue Cycle
5% revLive coding and claims rules protect cash timing after the first procedure.
Compliance and Credentialing
Compliance and Credentialing
For a radiofrequency ablation clinic, this is the gate to opening on time. You need active physician licensure, malpractice coverage, payer credentialing, a medical director structure, approved procedure scope, facility compliance, and an authorization workflow before first-day cases can safely run and bill.
Here’s the quick math: Month 1 carries $9,800 for malpractice, $1,200 for accreditation fees, and $1,500 for EHR and practice management. Those costs support state rules, payer contracts, clinical documentation, and safety protocols. If referrals open before payers and physicians are ready, expect canceled cases and denied claims.
Verify before referral launch
Before opening, confirm every licensure and payer file is live, not just submitted. Lock the medical director agreement, define procedure scope for pain and cardiac cases, and test the authorization path with a real packet so the clinic can bill from day one.
- Confirm state licensure and malpractice certificates.
- Complete payer credentialing and contract status.
- Document scope, safety, and documentation rules.
- Assign one owner for billing readiness.
Use one checklist for compliance, one for billing edits, and one for safety sign-off. If any piece slips, delay referral intake instead of filling the schedule with work that cannot be performed, documented, or paid.
1
Procedure-Room Readiness
Procedure-Room Setup
This driver decides whether the clinic can safely do procedures on day one, not just whether the room looks finished. The room has to support treatment workflow, imaging or guidance where needed, sterilization, recovery, emergency access, storage, patient privacy, utilities, and medical waste handling. If any one of those breaks, first-case scheduling slips.
Here’s the quick math: $18,500 in monthly clinical rent plus $2,800 for utilities and medical waste disposal means $21,300/month starts before the first procedure. A room that passes visual inspection but fails patient flow, sterile handling, or emergency access can still block opening and trigger rework, extra cash burn, and delayed revenue.
Pre-open room walk-through
Verify the room against the actual procedure sequence, not a floor plan. Check lease terms, buildout, equipment placement, staff movement, and emergency protocols together, because one bad layout can slow turnover or make a compliant procedure impossible. The room should support a clean path from intake to procedure to recovery without crossing dirty and clean traffic.
Document the setup before launch: utilities live, waste pickup in place, storage secured, privacy tested, and emergency access clear. Then run a full case simulation with the team and the exact equipment that will be used. If the mock flow breaks, fix it before opening so the first scheduled patient does not become the test case.
- Confirm sterile and clean paths.
- Test recovery-area handoff flow.
- Clear emergency access routes.
- Place equipment for safe movement.
- Verify waste pickup and storage.
2
Equipment and Vendor Setup
Equipment and Vendor Setup
For this clinic, launch readiness means the scheduled case can actually happen. The room needs an installed RFA generator, probes, electrodes, grounding pads, sterile kits, monitoring equipment, and imaging support where needed, plus a signed maintenance agreement and trained staff. If any of those are late, first cases slip even if the schedule is full.
The cost side is real from day one: $4,200/month for equipment maintenance contracts, 12% of revenue for disposable RFA catheters and kits in Year 1, and 25% for sterile supplies and gases. Here’s the quick math: equipment is not just a setup item, it is a live operating expense that must be in cash flow before opening.
Lock Vendor Timing Before Opening
Verify delivery dates, installation, clinical validation, and staff training before you publish the first procedure calendar. The reorder process should be written, assigned, and tested so consumables do not run out midweek. Late consumables or untrained staff are the main bottlenecks, and they usually show up as canceled procedures, not small delays.
- Confirm vendor delivery windows in writing.
- Test each device before first case.
- Train staff on setup and turnover.
- Set reorder points for kits and gases.
- Match imaging support to booked cases.
3
Clinical Staffing and Workflow
Day-One Clinical Staffing
This clinic cannot open on time if the procedure team and support staff are hired after referrals start. Day-one readiness means a scheduled cardiac electrophysiologist, interventional pain physician, nurse practitioner, 2 registered nurses, and 1 radiology technician, plus front desk, billing, and patient navigation that can document, coordinate, and close the loop.
The Month 1 admin payroll alone is about $584k per year, or $48.7k per month, from the $350k medical director, $95k clinic manager, $55k patient navigator, and 2 medical assistants at $42k each. If those roles are late, capacity drops, patient safety weakens, and reimbursement support gets messy because charts and follow-up are incomplete.
Hire Before Referrals Arrive
Lock the workflow before opening: who books, who checks records, who preps the room, who handles emergency response, and who runs follow-up. Here’s the quick test: a referral should move from intake to scheduled procedure to coded chart without a missing owner. If any handoff is vague, first-day volume will bottleneck fast.
- Assign one owner per handoff.
- Train emergency response before first case.
- Confirm billing support is live.
- Rehearse follow-up and documentation.
4
Referral Pipeline and Intake
Referral Intake Flow
Opening on time depends on turning referrals into booked, billable cases on day one. The gate is not demand alone; it’s records collection, benefits checks, prior authorization, and a clean handoff to scheduling. If those steps are slow, the room sits empty even when orthopedic, spine, neurology, primary care, and cardiology partners are sending patients.
Year 1 assumes patient acquisition and referral marketing at 3% of revenue, so weak intake can cap first-patient flow fast. The risk is interest without complete charts or payer approval, which delays a reimbursable procedure and pushes back utilization from day one.
Set the referral path first
Before opening, verify each source can send the right packet: referral agreement, patient education, intake script, records request, payer directory listing, local search presence, and follow-up scheduling. One clean path beats a lot of scattered leads. Train staff to ask for the missing chart, coverage details, and authorization status before a slot is held.
- Test records intake before launch
- Confirm authorization timing by payer
- Assign one owner per referral source
- Track no-chart and no-auth cases
5
Billing and Revenue Cycle
Billing and Revenue Cycle
Cash starts only after a clean, authorized case. For this clinic, the first revenue step is an authorized, documented RFA procedure, not just a completed procedure. If payer contracts, prior authorization rules, coding, and claim edits are not live, you can still treat patients but lose cash timing, which hurts opening runway fast.
The launch risk is simple: doing procedures before billing rules are ready creates denied claims, slow payments, and avoidable rework. Plan billing and claims processing at 5% of revenue in Year 1, then 4% by Years 4 and 5. That cost is small, but the timing risk is not. One bad week of claims can push first cash receipts well past day one.
Build the claim path before the first case
Load payer contracts, prior authorization rules, coding workflow, documentation standards, claim submission, denial management, collections tracking, and daily charge capture before opening. That means every scheduled RFA has the right notes, code set, and auth file ready before the patient enters the room.
- Test one mock RFA claim end to end.
- Confirm auth before scheduling procedures.
- Assign same-day charge entry ownership.
- Set denial follow-up within 24 hours.
What this setup prevents: performing procedures before billing rules are live. That mistake can delay cash, raise denial rates, and force staff to chase missing documentation after the fact. If the clinic cannot turn a completed procedure into a clean claim on day one, it is not ready to open at full speed.
6
Related Products
- Radiofrequency Ablation Clinic Porter's Five Forces Analysis
- Radiofrequency Ablation Clinic BCG Matrix
- Radiofrequency Ablation Clinic Business Model Canvas
- What Are The 5 KPIs For Radiofrequency Ablation Clinic?
- Radiofrequency Ablation Clinic Business Plan Template in Pre-Written Word
- How Increase Radiofrequency Ablation Clinic Profits?
- What Are Operating Costs For Radiofrequency Ablation Clinic?
- Radiofrequency Ablation Clinic Startup Costs: $134M+ CAPEX Plan
- Radiofrequency Ablation Clinic Financial Model Template in Excel
- How Much RFA Clinic Owners Make: $16M Year 1 EBITDA
- How Do I Write A Business Plan For Radiofrequency Ablation Clinic?
- Radiofrequency Ablation Clinic Marketing Mix
- Radiofrequency Ablation Clinic Marketing Plan
- Radiofrequency Ablation Clinic Business Proposal
- Radiofrequency Ablation Clinic PESTEL Analysis
- Radiofrequency Ablation Clinic Pitch Deck Example Editable PPTX
- Radiofrequency Ablation Clinic Business SWOT Analysis
- Radiofrequency Ablation Clinic Value Proposition Canvas
Frequently Asked Questions
Start by proving the clinic can operate safely and bill cleanly The Month 1 model needs 1 cardiac electrophysiologist, 1 interventional pain physician, 1 nurse practitioner, 2 registered nurses, and 1 radiology technician Then confirm licensure, malpractice coverage, facility readiness, RFA equipment, payer enrollment, referral intake, and billing before the first procedure