 Owner income$161k
Owner income$161kHow Much RFA Clinic Owners Make: $16M Year 1 EBITDA

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$161k  Net margin56.5%–79.0%
Net margin56.5%–79.0% Revenue for target pay$285k
Revenue for target pay$285k Business difficultyHard
Business difficultyHard


A radiofrequency ablation clinic owner can make a strong income if procedure volume, reimbursement, and staffing are well matched In this researched model, Year 1 collections are about $285k per month, with about $134k in monthly operating profit before debt, taxes, reserves, and reinvestment By Year 5, modeled monthly collections reach about $319M and operating profit reaches about $251M per month These are planning assumptions, not promised owner take-home
Owner income$161kNet margin56.5%–79.0%Revenue for target pay$285kBusiness difficultyHardWant to test your own RFA clinic profit?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or advice on owner distributions.
Want to see the Radiofrequency Ablation Clinic model?
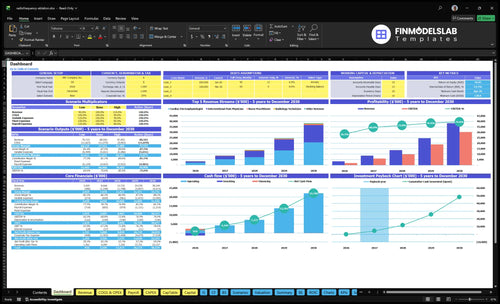
It shows revenue, margin, EBITDA, and owner income, plus scenario charts, in the Radiofrequency Ablation Clinic Financial Model Template.
Owner-income model highlights
- Owner take-home output
- Revenue and margin
- Year 1-5 scenarios
How many RFA procedures are needed to pay the owner?
RFA procedure volume depends on owner pay, reimbursement per case, margin, fixed overhead, payroll, and reserves. Here’s the quick math: required monthly procedures = (target profit + fixed costs + payroll) ÷ contribution per procedure, so lower contribution means more cases. In Year 1, the model starts with 25 cardiac treatments, 60 pain physician treatments, and only 45% to 50% capacity for core physicians.
What sets the need
- Target owner pay drives the goal.
- Reimbursement per case sets cash in.
- Fixed overhead raises break-even.
- Reserves add to the hurdle.
What the model says
- Use contribution per procedure.
- Start with 25 cardiac treatments.
- Start with 60 pain physician treatments.
- Core physicians run at 45% to 50% capacity.
What affects radiofrequency ablation clinic profit margin?
Profit margin in a Radiofrequency Ablation Clinic is mostly a function of payer mix, reimbursement per procedure, and how well the clinic controls labor, disposables, and denials. Year 1 is tight: COGS at 145% plus billing and marketing at 80% leaves little room, but by Year 5 it improves to 118% and 60%; here’s the quick math, the move is getting core physician capacity from about 45% to 90%. For a deeper operator view, see How Increase Radiofrequency Ablation Clinic Profits?
Cost drivers
- Payer mix sets cash collected.
- Reimbursement per procedure caps revenue.
- Disposable RFA catheters and kits hit margin fast.
- Physician compensation rises with procedure load.
Margin levers
- Fluoroscopy or imaging access protects throughput.
- Equipment maintenance and rent stay fixed.
- Billing and denial performance lift collections.
- Staff utilization improves as capacity nears 90%.
How much revenue does a radiofrequency ablation clinic need to pay the owner?
A Radiofrequency Ablation Clinic needs about $285k in monthly collections before the owner should expect distributions; see How Increase Radiofrequency Ablation Clinic Profits? for the profit levers. That leaves about $134k monthly operating profit before debt, taxes, reserves, and reinvestment.
Revenue floor
- Target collections: $285k/month
- Cover provider pay first
- Fund disposables and sterile kits
- Hold reserves before distributions
Cost load
- Variable and COGS: 225% modeled
- Fixed overhead: $386k
- Known payroll: about $487k
- Profit before financing: $134k/month
Want the six RFA clinic income drivers?
1
$3.4M-$38.2MProcedure Volume
More cases are the main growth engine, and revenue scales from $3.42M in Year 1 to $38.24M in Year 5.
2
$95-$17KPayer Mix
The case mix runs from low-price pain work to high-price cardiac work, so average reimbursement can move EBITDA fast.
3
$445KProvider Pay
The $350K medical director and $95K clinic manager salary base must be covered before owner cash starts to climb.
4
45%-90%Facility Use
Higher room and equipment use spreads rent, maintenance, and software costs across more cases, so underuse hits margin hard.
5
$177K-$493KStaffing Costs
Support staff climb from 4 FTE to 11 FTE, and supplies add more drag if volume ramps too slowly.
6
4%-5%Billing Collections
Claims processing falls from 5% of revenue to 4%, and that one-point swing drops straight to EBITDA.
Radiofrequency Ablation Clinic Core Six Income Drivers
Procedure Volume and Schedule Utilization
Billable Procedure Volume
More completed, billable procedures are what turn a specialty clinic into owner income. Year 1 assumes 25 cardiac electrophysiologist treatments at 45% capacity and 60 interventional pain physician treatments at 50% capacity. By Year 5, that rises to 30 and 80 treatments with utilization near 85% to 90%. Consults help fill the funnel, but they do not pay the bills until they convert.
Here’s the quick math: if rooms, imaging access, providers, and staff are not tightly scheduled, revenue stalls even when demand exists. Low utilization leaves fixed costs spread over too few cases, so owner draw gets squeezed. The key inputs are completed procedures, capacity, and consult-to-procedure conversion. Empty slots are lost margin.
Fill the Schedule, Not Just the Funnel
Track booked slots, completed procedures, cancellations, and no-shows by provider and room. Separate consult volume from paid cases so the forecast does not overstate cash. If cardiac volume stays at 45% capacity, or pain stays at 50%, the clinic is underusing fixed assets and staff. The target is tighter block scheduling, faster turn times, and fewer open gaps.
- Measure consult-to-procedure conversion weekly.
- Track utilization by room and provider.
- Watch cancellations and same-week fills.
- Schedule imaging and staff to case blocks.
1
Payer Mix and Reimbursement
Payer Mix Drives Cash per Case
Payer mix and reimbursement decide how much cash each radiofrequency ablation case actually brings in, so this driver can change owner take-home faster than volume alone. In Year 1, model prices are $15,500 for cardiac electrophysiologist treatments and $3,200 for interventional pain physician treatments; by Year 5, they rise to $17,000 and $3,650. That spread matters because one payer shift can move collections, margin, and draw.
Use commercial, Medicare, authorization, denial, and patient-balance assumptions as planning inputs, not billing promises. If reimbursement slips or denials rise, the clinic can still do the same number of procedures and collect less cash, which squeezes operating profit and delays owner pay. The real question is net cash per paid case, not posted charge per case.
Track Net Collection per Procedure
Build the model around gross charge, allowed amount, denial rate, patient balance, and days in A/R. For example, if cardiac cases are priced at $15,500 in Year 1 and pain cases at $3,200, you need to know how much of that is expected cash after payer rules and collection lag. That is what funds payroll, rent, and owner distributions.
- Track paid rate by payer.
- Review denial reasons weekly.
- Separate commercial from Medicare.
- Test patient collection timing.
- Reforecast after contract changes.
Keep the pricing plan tied to actual collections, not just scheduled procedures. If Year 5 pricing reaches $17,000 and $3,650, but authorization or denial friction grows, the lift may never reach the owner’s bank account. One clean rule: measure what was collected per completed case, then compare it to the assumed price.
2
Provider Compensation and Owner Clinical Role
Provider Pay and Owner Draw
If the owner performs procedures, provider compensation is the swing cost between clinic profit and take-home pay. The key split is wages vs. distributions: procedure pay to clinicians is an operating cost, while owner profit is what stays after payroll, medical oversight, and clinic overhead.
In this model, known Year 1 payroll is about $584k, plus a $350k annual Medical Director and a $95k Clinic Manager. That means even strong procedure volume can leave little owner draw if staffing runs hot, and compliance rules still control who can own, supervise, and bill.
Separate Clinical Pay from Profit
Track owner procedures, hired-provider pay, medical director fees, and clinic manager cost separately. Here’s the quick math: owner income equals procedure margin after clinical payroll, then minus fixed oversight costs. If the owner mixes wage income with profit distributions, it gets hard to see whether the clinic is actually paying for itself.
Build the forecast around provider utilization, not just consultations. Use a simple monthly check on staffed hours, billable procedures, and payroll against the $584k Year 1 base. If staffing rises faster than paid cases, margin drops fast and owner pay gets squeezed even when revenue looks busy.
3
Facility, Equipment, and Financing Utilization
Facility and Equipment Fixed Load
Facility, equipment, and financing costs set the floor your clinic has to clear before owner pay starts. Here’s the quick math: disclosed fixed monthly costs total $380.6k from $185k rent, $42k equipment maintenance, $98k malpractice, $15k EHR and practice management software, $28k utilities and waste, $600 office supplies, and $12k accreditation, before generators, imaging access, buildout, and financing. When the schedule is light, these costs still hit cash flow.
The key driver is utilization, meaning how fully the rooms, equipment, and staff are used. Low volume spreads the same overhead across fewer paid procedures, so break-even rises and the owner’s draw falls fast. Track monthly billable procedures, downtime, and the full fixed cost pool; consultations do not pay the rent.
Track Fixed Cost per Billable Case
Use fixed cost per procedure as the main check. Divide monthly fixed costs by paid cases, then compare that number to case contribution margin. If volume slips, ask whether the issue is room time, equipment uptime, or payer mix. Keep separate monthly lines for rent, maintenance, malpractice, software, utilities, supplies, accreditation, and financing so you can see what must be covered every month.
Test schedule density by site and provider, and forecast the break-even case count before adding leases or equipment. A short month with the same overhead can erase owner pay even when revenue looks decent. The goal is simple: keep each fixed dollar tied to more completed, billable procedures.
4
Clinical Labor, Supplies, and Case Costs
RFA Case Cost Pressure
Owner pay gets squeezed when each radiofrequency ablation (RFA) case carries too much supply and labor. In this model, disposable catheters and kits equal 120% of revenue in Year 1 and 100% in Year 5, and medical gases plus sterile supplies add another 25% and 18%. That means case-level spend can run above collections before overhead.
Here’s the quick math: suppl y cost alone is 145% of revenue in Year 1 and 118% in Year 5 before staffing. So even if bookings look strong, long case duration, sedation support, recovery flow, inventory waste, and overtime can wipe out owner draw. One slow room day can turn a busy schedule into thin cash.
Track Cost per Case
Measure cost per completed case by procedure type, not just monthly spend. Track case duration, sedation hours, recovery time, overtime, and kit use against each billable procedure so you can see where margin leaks. If a case runs long or needs extra staff, the extra labor should be visible in the file, not hidden in payroll.
- Cases by procedure type
- Kit and catheter usage
- Gases and sterile supplies
- Sedation and recovery labor
- Overtime hours by week
- Expired or unused inventory
Set a weekly review for waste, turnover time, and stock counts. Tight inventory control, shorter room time, and disciplined staffing protect gross margin and keep more cash available for owner pay. If staffing runs high when volume is soft, the clinic can look busy and still pay the owner less.
5
Billing Performance and Cash Collections
Billing Speed and Cash Collection
This driver covers authorizations, chart support, clean claims, denials, patient balances, and days in accounts receivable—the time between a procedure and cash in the bank. In this RFA clinic model, billing and claims processing is 50% of revenue in Year 1 and 40% in Year 5, while referral marketing is 30% in Year 1 and 20% in Year 5, so slow collections can squeeze owner draw even when procedures are booked.
Here’s the quick math: if claims are held up, revenue may be earned but not collected, and the clinic still has to fund payroll, rent, supplies, and provider pay. The key inputs are procedure count, payer mix, authorization rate, denial rate, patient balance collection, and billing labor. Don’t assume any code or payment rate is guaranteed.
Track Clean Claims and A/R Weekly
Use weekly reporting on clean claim rate, denial rate, patient collection rate, and days in A/R. If authorizations or documentation slip, cash lags fast, and owner pay gets stuck behind unpaid claims. Keep every procedure tied to complete notes, correct coding, and fast patient billing so the clinic collects closer to the time of service.
Watch the cash split by source: procedure payments, patient balances, and referral spend. If referral marketing stays near 30% of Year 1 revenue, it can drain cash before collections catch up; by Year 5, the model drops that to 20%. A tighter billing workflow does not raise billed revenue by itself, but it can raise usable cash, which is what pays the owner.
6
Compare low, base, and high RFA clinic owner income scenarios
Owner income scenarios
Income moves with procedure volume, collections, and fixed staffing. Early slack bites hard because overhead is heavy, but scale lifts earnings fast once utilization and pricing hold.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | Lower utilization and weaker collections keep owner income under the modeled first-year run rate. | Modeled first-year operations deliver the core case for pre-tax owner income. | Later-stage scale and fuller capacity lift owner income well above the opening-year run rate. |
| Typical setup | Rooms run below plan, denials stay high, and fixed payroll and facility costs still hit the P&L. | Volume follows Year 1 assumptions, with $3.42M revenue and $1.93M EBITDA before debt and tax. | By Year 5, revenue reaches $38.24M and EBITDA reaches $30.22M as utilization and staffing scale. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Below Year 1 EBITDALow income band | About $1.9M annualBase income band | About $30.2M annualHigh income band |
| Best fit | Use this to stress-test a soft launch or slow referral ramp. | Use this for planning lender talks and annual budgets. | Use this to test upside from strong referrals and smooth staffing. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. They are pre-tax and before debt, reserves, reinvestment, and owner distribution policy.
Related Products
- Radiofrequency Ablation Clinic Porter's Five Forces Analysis
- Radiofrequency Ablation Clinic BCG Matrix
- Radiofrequency Ablation Clinic Business Model Canvas
- What Are The 5 KPIs For Radiofrequency Ablation Clinic?
- Radiofrequency Ablation Clinic Business Plan Template in Pre-Written Word
- How Increase Radiofrequency Ablation Clinic Profits?
- What Are Operating Costs For Radiofrequency Ablation Clinic?
- Radiofrequency Ablation Clinic Startup Costs: $134M+ CAPEX Plan
- Radiofrequency Ablation Clinic Financial Model Template in Excel
- How To Launch Radiofrequency Ablation Clinic?
- How Do I Write A Business Plan For Radiofrequency Ablation Clinic?
- Radiofrequency Ablation Clinic Marketing Mix
- Radiofrequency Ablation Clinic Marketing Plan
- Radiofrequency Ablation Clinic Business Proposal
- Radiofrequency Ablation Clinic PESTEL Analysis
- Radiofrequency Ablation Clinic Pitch Deck Example Editable PPTX
- Radiofrequency Ablation Clinic Business SWOT Analysis
- Radiofrequency Ablation Clinic Value Proposition Canvas
Frequently Asked Questions
In this model, owner take-home potential starts from operating profit, not revenue Year 1 revenue is about $342M, and EBITDA is about $160M before debt, taxes, reserves, and reinvestment Year 5 modeled EBITDA reaches about $3011M, but that assumes major provider growth and high utilization