 Time to Open3-6 monthsSetup window
Time to Open3-6 monthsSetup windowHow To Start A Remote Patient Monitoring Business In 90 To 180 Days

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open3-6 monthsSetup window  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckContracting gateProvider coverage
Key BottleneckContracting gateProvider coverage First Revenue StepBillable enrollmentsBilling ready
First Revenue StepBillable enrollmentsBilling ready


Key Takeaways
- HIPAA readiness comes before any pilot or patient data.
- Platform and device choices drive launch speed and reliability.
- Training and alert workflows protect day-one operations.
- Signed provider contracts turn compliance into enrolled patients.
Time to Open3-6 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckContracting gateProvider coverageFirst Revenue StepBillable enrollmentsBilling readyRemote patient monitoring launch timeline
Short web summary of the launch plan; the XLSX export contains the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8
Legal / compliance
- Draft BAA pack
- Review HIPAA rules
- Approve consent forms
- Check privacy flow
- Clear launch signoff
Platform / devices
- Select device stack
- Configure data flow
- Build EHR link
- Set security tools
- Receive device inventory
Clinical / staffing
- Write care protocols
- Hire support staff
- Train monitoring team
- Define escalation rules
Provider sales
- Build target list
- Start outreach
- Run workflow demos
- Close provider contracts
- Confirm referral flow
Billing / finance
- Set billing setup
- Map payer codes
- Test claims flow
- Review cash runway
Patient onboarding / pilot
- Write intake scripts
- Set shipping process
- Enroll pilot patients
- Launch pilot review
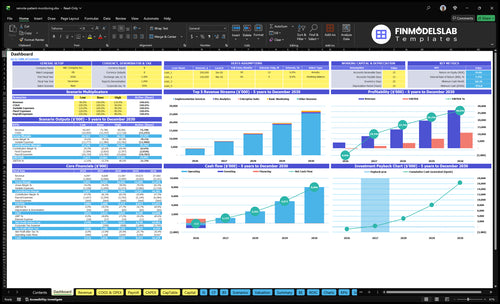
Can the Remote Patient Monitoring model support your launch timing?
Yes—this Remote Patient Monitoring Financial Model Template maps launch timing, cash needs, and breakeven; open the model.
Launch timing checks
- Pricing: $85 to $195
- Marketing: $850,000 Year 1
- Cash low: Month 7
- Breakeven: Month 8
- Payback: 23 months
How long does it take to launch remote patient monitoring?
For Remote Patient Monitoring, plan on 90 to 180 days to launch; anything faster needs a narrow pilot, a ready provider partner, a selected device stack, and finished HIPAA workflows. The biggest delays usually come from platform selection, BAAs, EHR workflow alignment, provider contracting, device logistics, billing setup, and clinical staffing. The capex schedule runs from Month 1 to Month 6, and the financial model shows breakeven in Month 8, so launch slippage raises cash risk fast.
What delays launch
- Platform selection takes time.
- BAAs must be signed first.
- EHR alignment slows setup.
- Provider contracting adds weeks.
What must happen in order
- HIPAA workflow before patient data.
- Device testing before enrollment.
- Billing workflow before claims.
- Clinical escalation before monitoring starts.
How do you get clients for remote patient monitoring?
If you’re getting clients for Remote Patient Monitoring, sell to provider organizations first: clinics, physician groups, chronic care practices, home health agencies, and value-based care groups. For startup cost context, see What Is The Estimated Cost To Open And Launch Your Remote Patient Monitoring Business? Revenue starts with a signed provider agreement and then billable enrolled patients, not a promise of reimbursement. Year 1 assumes 2 sales FTE, a $850,000 marketing budget, and CAC of $2,800, improving to $2,000 by Year 5.
Workflow fit
- Find eligible patients fast
- Handle consent and setup
- Monitor, escalate, and document
- Pass off billing cleanly
Sales math
- Target provider organizations, not patients
- Separate acquisition from enrollment
- Count revenue after a signed agreement
- Track CAC from $2,800 to $2,000
What do you need to start a remote patient monitoring business?
To start a Remote Patient Monitoring business, you need launch controls first: Health Insurance Portability and Accountability Act compliance, Business Associate Agreements, provider contracts, patient consent, eligible enrolled patients, billing setup, clinical protocols, devices, software, and staffed support. Before monitoring starts, get state legal review because licensing depends on service model and clinical scope, and use What Is The Most Crucial Metric For Remote Patient Monitoring Success? to pressure-test the operating metric.
Launch Controls
- Sign provider agreements first
- Execute BAAs with partners
- Collect documented patient consent
- Confirm state licensing needs
Operating Stack
- Use HIPAA-ready RPM software
- Support connected medical devices
- Staff 3 clinical support roles
- Price at $85, $135, or $195 monthly plus $2,500 setup
Confirm what must be ready before opening day
Launch readiness checklist
Use this go-live approval checklist to confirm the service is ready before opening.
Compliance
- Entity and operating docs completeCritical
The business needs a clean legal base before contracts, banking, and vendor setup.
- HIPAA policies approvedCritical
Written rules keep staff handling protected health data the same way.
- BAA templates signedCritical
No BAA means no safe vendor or provider data sharing.
- Cyber coverage boundHigh
Cyber risk is real here, so coverage should start before launch.
- Consent language approvedCritical
Patients must sign clear consent before monitoring starts.
Technology
- HIPAA-ready platform chosenCritical
The system must handle protected health data before any patient data moves.
- Connected devices testedCritical
Device data has to flow into the platform without drops.
- Dashboards and alerts workHigh
Staff need live views and alerts or they will miss issues.
- Integrations map verifiedHigh
Test links to records and billing before first patient onboarding.
Devices
- Device sourcing securedCritical
Devices must be locked before demand starts or shipments slip.
- Inventory counted and taggedHigh
Track every device so lost stock does not delay activation.
- Fulfillment path testedCritical
Test the path from order to patient use before launch.
- Return replacement rules setMedium
Define swaps and returns now to avoid service gaps and extra cost.
Clinical
- Escalation rules approvedCritical
No escalation rule means alerts can sit unanswered and patient risk rises.
- Monitoring hours setHigh
The team needs one clear monitoring window and backup coverage.
- Documentation standards loadedHigh
Notes must be consistent so billing, audits, and handoffs stay clean.
- Provider contracts signedCritical
Without provider contracts, you cannot bill or route clinical oversight cleanly.
Team
- Year 1 team staffedCritical
Staffing needs 1 CEO, 4 engineers, 3 clinical support, 2 sales, 2 CS, and 2 ops.
- Clinical staff trainedCritical
Clinical staff need the escalation, charting, and patient follow-up playbook.
- Sales and CS assignedHigh
Sales and success must own first outreach, onboarding, and renewal handoffs.
- Ops coverage scheduledHigh
Ops must cover device flow, support queues, and day-one issue handling.
Cash
- Pricing model approvedCritical
The launch needs clear prices at $85, $135, and $195 per month before sales start.
- Assumptions reconciledCritical
Use 18% Year 1 device cost, 8% cloud cost, and Month 8 breakeven in the model.
- CAC target acceptedHigh
CAC starts at $2,800 and trends to $2,000, so spend must fit the payback plan.
- Cash dip coveredCritical
The model hits a $455k cash low, so funding must cover the early hole.
- Go-live signoff completeCritical
No launch until compliance, tech, staffing, and billing all have one owner.
Which launch drivers control the opening date?
1Compliance Readiness
90-180 daysNo pilot starts until BAAs, HIPAA policies, and consent rules are in place.
2RPM Stack
$200K devicesA ready device stack cuts onboarding failures and keeps data flowing on day one.
3Clinical Workflow
14 FTEDefined escalation rules and trained staff reduce alert overload and protect retention.
4Provider Contracts
$850K budgetYear 1 sales spend and 2 sales FTE support clinic signings, but contracts still set first revenue timing.
5Billing Workflow
Month 8Clear billing ownership and audit trails speed clean claims after enrollment.
6Patient Onboarding
Month 7 lowStrong onboarding and follow-up reduce drop-offs and keep billable patients active.
Compliance Readiness
HIPAA Launch Gate
For remote patient monitoring, compliance is the first gate. Do not collect patient data until signed Business Associate Agreements (BAAs), HIPAA policies, secure data transmission, patient consent language, documentation standards, and breach response are live. If any of those are late, the launch slips because the platform cannot legally or safely receive readings from day one.
The biggest risk is simple: data starts flowing before controls do. That can freeze provider contracting, delay the pilot, and force rework on privacy, access controls, vendor review, and the service model. The legal review has to happen before patient onboarding, not after.
Sequence the control stack
Start with the platform vendor and provider contracts, then confirm access controls, secure transmission, and consent workflow. Put the privacy policy, security policy, and breach response in writing, and test the documentation path for each patient record before opening.
No pilot until the BAAs and consent workflow are complete. Assign one owner to collect signed contracts, one to verify vendor readiness, and one to check cyber liability coverage and service-model review. That keeps the launch clean and lowers delay risk.
- Verify signed BAAs first
- Test consent before enrollment
- Confirm secure data transmission
- Review vendors and access
- Hold pilot until controls live
1
RPM Platform And Device Stack
Device Stack Readiness
For remote patient monitoring, the platform and device stack is what makes day one work. You need a HIPAA-ready platform with supported devices, dashboards, alerts, patient enrollment tools, secure data transmission, integrations, and device fulfillment. If devices do not pair cleanly or data does not flow, onboarding slows and patients start with gaps.
Here’s the quick math: the plan calls for $85,000 of device testing equipment from Month 2 to Month 4 and $200,000 of initial device inventory from Month 3 to Month 5. Year 1 also assumes 18% medical device costs and 8% cloud costs. The bottleneck is simple: unsupported devices or weak data flow create failed enrollments and delay first-revenue patients.
Test Before You Stock
Start with a locked device list and prove each device can transmit clean data into the dashboard before inventory lands. Build the workflow around device testing, inventory planning, logistics, troubleshooting scripts, and data QA so the launch team knows what ships, who handles failures, and how bad readings get flagged.
- Confirm supported devices first
- Test pairing and data flow
- Map fulfillment and replacement steps
- Write scripts for common setup issues
- Run data QA before patient enrollment
If onboarding takes longer than planned, the hit shows up fast: more support tickets, more device swaps, and fewer patients fully live on day one. Tight device QA and a clear logistics flow reduce those failures and keep the opening date realistic.
2
Clinical Monitoring Workflow
Clinical Monitoring Readiness
Remote patient monitoring cannot open safely until the monitoring hours, alert thresholds, escalation rules, and care team roles are locked. If those rules are loose, the team gets hit with alert volume before anyone knows who responds, when to notify the provider, or how to document the note. That slows day-one care and can create billing gaps.
The Year 1 staffing plan is 3 clinical support staff at $75,000 each plus 2 customer success managers at $85,000 each, or $395,000 per year. That only works if provider workflow and billing documentation are already set, because weak handoffs turn every alert into manual work and raise retention risk.
Set The Alert Path Before First Patient
Before opening, test the escalation playbook on real cases: high blood pressure, missed readings, and out-of-range glucose. Define patient risk categories, provider notification rules, and audit-ready notes so staff act the same way every time. Here’s the quick math: $395,000 in Year 1 clinical staffing only works if one trained team can absorb the alert load without delays.
Use a short launch checklist: confirm who reviews alerts, who documents, who calls the provider, and who closes the loop with the patient. Train before acceptance, not after. If the team is still learning while alerts are live, response time slips, and that can hurt first-day operations, payment support, and patient trust.
3
Provider Contracts
Signed Provider Agreements
For remote patient monitoring, signed clinic or physician agreements are the first revenue gate. Until the contract matches the care workflow, you may have a compliant setup but still no enrolled patients, so opening on time does not equal opening with revenue.
The main risk is delay. EHR workflow alignment and contracting often move slower than device or software setup, so the launch slips even when the platform is ready. With a modeled 2 sales FTE plan and $850,000 in Year 1 marketing spend, a $2,800 CAC only works if signatures turn into live patient starts fast.
Lock the Pilot Terms Early
Before launch, get one clear operating sheet signed by each partner. It should cover target specialty, value proposition, pilot scope, eligible patient criteria, workflow map, data-sharing terms, and billing responsibilities. That keeps the sales team, clinical team, and billing team from building three different versions of the same launch.
- Map the EHR handoff.
- Assign billing ownership.
- Define who enrolls patients.
- Test consent and data access.
If the provider will not confirm workflow steps and billing ownership, do not set patient start dates yet. Weak contract language turns into day-one confusion, slower enrollment, and cash burn before the first billable patient is live.
4
Billing And Reimbursement Workflow
RPM Billing Workflow
If you launch without a clear billing owner, you can still enroll patients but miss the first claims. RPM billing is an operational dependency, not a reimbursement promise, so the launch has to cover consent, device data, clinical notes, patient eligibility, payer rules, provider agreement, and the revenue cycle handoff.
Use the common Medicare RPM code set as your workflow map: 99453, 99454, 99457, and 99458. The weak spot is incomplete documentation, which slows first clean claims after enrollment and can delay cash even when patients are active.
Set Billing Ownership Before Day One
Before opening, write one billing SOP that names who checks eligibility, who tracks time, who reviews notes, who signs off, and who follows denials. Test the audit trail and the revenue cycle handoff before the first patient ships a device. That keeps day-one operations from turning into a billing backlog.
Track only the inputs that drive a clean claim: consent, device data, clinical notes, and provider agreement. If any one is missing, the claim can stall even though care is already happening.
- Confirm payer rules per patient.
- Capture time every billing cycle.
- Link notes to each RPM code.
- Route denials the same day.
5
Patient Onboarding And Retention
Onboarding That Turns Enrollment Into Active Data
When remote patient monitoring opens, the risk isn’t just enrollment; it’s getting a usable reading on day one. Consent captured, device set up, patient trained, troubleshooting live, and engagement cadence defined have to be ready before launch, or first revenue stays stuck in a pilot that never becomes a billable active patient.
The cost mix is tight. With 35% logistics cost and 18% medical device cost, 53% of revenue is already tied to fulfillment and hardware before labor or software. If devices do not sync or patients stop using them, staff will spend launch week fixing failures instead of retaining enrolled patients.
Test the full patient path before go-live
Before opening, verify the path from enrollment to first data point in this order: consent captured, device shipped or set up, patient trained, and data flowing. Build the day-one scripts for welcome calls, device pairing help, refill or replacement requests, missed-reading outreach, and escalation handoff so staff do not improvise under pressure.
- Track first reading within 24 hours.
- Assign one owner for device issues.
- Test replacement workflow before launch.
- Confirm outreach after missed readings.
If onboarding runs late or data does not sync, the business can be open and still not be operational. That means fewer billable enrolled patients, slower cash flow, and more drop-offs after the pilot.
6
Related Products
- Remote Patient Monitoring Porter's Five Forces Analysis
- Remote Patient Monitoring BCG Matrix
- Remote Patient Monitoring Business Model Canvas
- 7 Critical KPIs for Remote Patient Monitoring Success
- Remote Patient Monitoring Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Remote Patient Monitoring Profitability
- Operating Budget: Analyzing Monthly Costs for Remote Patient Monitoring
- Remote Patient Monitoring Startup Costs: $650K CAPEX Plan
- Remote Patient Monitoring Financial Model Template in Excel
- How Much Can A Remote Patient Monitoring Owner Make At $12450 PMPM?
- How to Write a Remote Patient Monitoring Business Plan
- Remote Patient Monitoring Marketing Mix
- Remote Patient Monitoring Marketing Plan
- Remote Patient Monitoring Business Proposal
- Remote Patient Monitoring PESTEL Analysis
- Remote Patient Monitoring Pitch Deck Example Editable PPTX
- Remote Patient Monitoring Business SWOT Analysis
- Remote Patient Monitoring Value Proposition Canvas
Frequently Asked Questions
Start with the operating model, then build the compliance and provider workflow around it Plan 90 to 180 days for setup, with HIPAA policies, BAAs, RPM software, connected devices, clinical protocols, provider contracts, billing workflow, and a pilot The model assumes Year 1 pricing of $85, $135, and $195 per monitored patient plan