 Owner income$16.7k
Owner income$16.7kHow Much Can A Remote Patient Monitoring Owner Make At $12450 PMPM?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$16.7k  Net margin67.7%
Net margin67.7% Revenue for target pay$236.6k
Revenue for target pay$236.6k Business difficultyHard
Business difficultyHard


You’re modeling owner take-home before the patient base is stable, so this page uses the first-year pricing mix, cost structure, staffing plan, and cash runway assumptions to estimate income The clearest owner-pay input is $200,000 CEO salary, but true owner draw depends on collections, reserves, and active billable patients This is not payroll, tax, legal, compliance, personal guarantee, or exact Medicare reimbursement advice
Owner income$16.7kNet margin67.7%Revenue for target pay$236.6kBusiness difficultyHardWhat owner pay can your RPM patient panel support?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Remote Patient Monitoring model?
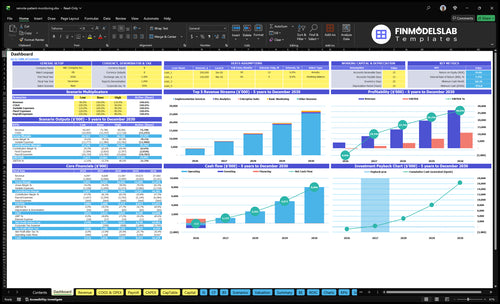
Open the Remote Patient Monitoring Financial Model Template to see owner income, cash trough, payback, gross margin, and patient economics. Tabs cover ramp, pricing mix, costs, scenarios, reserves, and cash flow.
Key model signals
- $12,450 PMPM proxy
- 677% gross margin
- $237,000 load incl. CEO pay
- -$455,000 minimum cash
Which remote patient monitoring revenue model supports better owner income?
Provider-contracted PMPM fees are usually the cleanest way to model owner income in Remote Patient Monitoring because the monthly revenue per active patient is easier to track when contract terms and collections are clear. Reimbursement-share models can raise upside, but denials, timing gaps, and compliance risk can shrink take-home pay. Care-management bundles can support higher account value, but they also need more clinical labor and support, so validate payment terms, billing duties, and reserves with signed contracts and qualified advisors.
Best for planning
- PMPM ties income to active patients
- Monthly cash is easier to model
- Clear contracts reduce payment surprises
- 24/7 support stays in the cost base
Higher upside, more risk
- Reimbursement-share can boost upside
- Denials can slow cash collection
- Bundles can lift account value
- More labor can reduce owner margin
What profit margin can a remote patient monitoring business earn?
Remote Patient Monitoring can show very high gross margin, starting at 677% in year 1 and improving to 765% in the mature year under the provided assumptions. That is not operating margin, because payroll, marketing, rent, insurance, legal, tools, and admin still hit profit first; for the launch-cost side, see What Is The Estimated Cost To Open And Launch Your Remote Patient Monitoring Business?. Owner take-home improves when clinical labor productivity rises and device cost falls.
Year 1 margin
- 677% gross margin starts the model
- Includes device, cloud, shipping, processing
- Not the same as operating margin
- First-year payroll is $1.435 million
What lifts take-home
- Mature gross margin reaches 765%
- Marketing is $850,000
- Fixed overhead is $564,000
- Lower device cost boosts owner take-home
How much can a remote patient monitoring business owner make?
A Remote Patient Monitoring owner can target a $200,000 CEO salary, or about $16,667 per month before tax, but that’s not a guaranteed owner draw. The real answer depends on active billable patients, collections, staffing, marketing spend, reserves, and the core metric explained here: What Is The Most Crucial Metric For Remote Patient Monitoring Success?.
Owner Pay Math
- $200,000 annual CEO salary target
- $16,667 monthly before tax
- $124.50 PMPM pricing proxy
- About $84 contribution per patient
Draw Comes Last
- Fund payroll first
- Cover fixed overhead
- Pay marketing and debt service
- Protect the Month 7 cash trough
Want the six RPM income drivers in one view?
1
$84Billable Patients
More active billable patients is the biggest take-home lever because each one adds about $84 of contribution before fixed overhead.
2
$125 PMPMPMPM Mix
A better mix of plans and services lifts monthly revenue per patient, so every new patient pays back more of the sales and support load.
3
32.3%Patient Data
When patients engage and transmit clean data, rework stays down and variable cost can stay near 32.3% of revenue.
4
16 FTEClinical Output
Higher clinician productivity keeps support growth behind revenue, which protects margin as the team scales from 3 to 16 FTE.
5
26%-19%Cost Control
Tight device and cloud control matters because those costs start near 26% of revenue and can fall to 19% by year 5.
6
$2.8K CACProvider Growth
Acquisition only works if CAC stays near $2,800, since $850,000 of first-year marketing and the -$455,000 cash low leave little room for waste.
Remote Patient Monitoring Core Six Income Drivers
Active Billable Patient Count
Active Billable Patients Drive Owner Pay
Owner income scales with active billable patients, not just sign-ups. Enrolled means signed up, active means still using the device, transmitting means sending usable readings, and billable means the patient meets the billing rule. At the disclosed first-year assumption of $124.50 PMPM and 67.7% contribution margin, each active billable patient adds about $84 a month before payroll, overhead, marketing, and reserves.
Here’s the quick math: 2,817 active billable patients cover about $237,000 in monthly first-year operating load before reserves. So the owner’s draw depends on keeping patients transmitting and billable, not just enrolled. Low device use, missed readings, or slow reactivation pushes the needed census higher and squeezes cash.
Track Billable Status, Not Just Enrollment
Measure the count that actually bills. A patient can be enrolled but still fail to create cash if readings stop or the device sits idle. Each lost active billable patient removes about $84 per month of contribution, so the gap hits owner pay fast.
- Track enrolled, active, transmitting, billable
- Watch onboarding completion weekly
- Flag missed readings within 24 hours
- Monitor device return and reactivation time
Forecast from billable census only, not total enrollment. Keep a cushion above 2,817 active billable patients so normal drop-off does not break monthly operating coverage.
1
Net Revenue Per Patient Per Month
Net PMPM Revenue
Net revenue per patient per month (PMPM, per patient per month) is the cash yield that actually funds payroll, overhead, and owner pay. Using the disclosed mix at $85, $135, and $195, the first-year proxy is about $124.50 PMPM. That’s the real revenue quality metric, not the billed rate.
The $2,500 implementation fee helps first-year cash, but it should not be treated as recurring PMPM unless the contract says it repeats. If collections, denials, or payer mix slip, the same patient count can produce less cash and less money available for the owner to draw.
Protect Cash PMPM
Track the bridge from billed revenue to cash: payer mix, collection rate, denial rate, provider contract rates, and reimbursement-share terms. Here’s the quick math: billed PMPM minus denials and uncollected amounts equals cash PMPM, and that is what supports owner income.
- Separate setup fees from recurring PMPM
- Review denials by payer each month
- Reprice low-yield contracts fast
- Forecast cash by patient cohort
2
Patient Engagement And Data Transmission
Billable Patient Engagement
Remote patient monitoring (RPM) only pays on active, transmitting, billable patients, not on enrolled names in the system. Missed readings, inactive devices, poor onboarding, and low adherence shrink the active census, and each lost active patient removes about $84 per month of first-year contribution.
Here’s the quick math: lose 10 active patients, and you give up about $840 monthly before payroll, overhead, and marketing. The inputs that matter are transmission rate, onboarding completion, device return rate, support tickets, and reactivation time. Enrollment looks good on paper, but cash depends on patients actually sending data.
Track Activation, Not Just Enrollment
Run the business from a weekly dashboard. Track enrolled, active, transmitting, and billable patients separately, then flag anyone who stops sending data within days, not weeks. If onboarding is weak, the active base will leak and owner pay will fall even when sales keep growing.
- Measure onboarding completion rate.
- Watch missed readings daily.
- Count inactive device days.
- Track reactivation time.
- Review support tickets by patient.
Keep one rule: if a patient stops transmitting, treat it as a revenue problem first. Faster outreach and cleaner onboarding protect recurring contribution and keep more cash available for owner draw.
3
Clinical Labor Productivity
Clinical Labor Productivity
In remote patient monitoring, clinical labor is the cost of nurses or care staff who review data, handle escalations, and document work. First-year support is 3 FTE at $75,000 each, or $225,000 a year, which is about $18,750 per month. If minutes per patient, overtime, and documentation time rise faster than active billable patients, owner pay gets squeezed even if revenue keeps growing.
The key test is contribution per patient versus labor load. Here’s the quick math: if each active billable patient adds about $84 per month before payroll, overhead, and reserves, then labor has to stay light enough to preserve that spread. In the mature year, labor can rise to 16 FTE and $12 million, so utilization and escalation volume matter just as much as patient count.
Measure minutes, not just headcount
Track minutes per patient, escalation rate, documentation time, overtime, and staff utilization each week. Also separate enrolled, active, and billable patients, because labor tied to inactive patients destroys margin. If onboarding is messy or alerts are noisy, staff time goes up before cash does, and that directly cuts owner draw.
Set a simple rule: compare clinical labor cost to contribution per active patient, not total revenue. If the team needs more labor to support the same census, fix workflows, tighten documentation, and reduce avoidable alerts before adding staff. One clean metric to watch: how many active billable patients each full-time clinician supports without overtime.
4
Device And Platform Cost Control
Device and Platform Cost Load
Device and platform costs eat margin before cash hits owner pay. In the first year, disclosed variable costs equal 323% of revenue from 180% device costs, 80% cloud infrastructure, 35% shipping, and 28% processing. That means every $100 of revenue can carry about $323 of variable cost before payroll and overhead. One clean rule: if the platform price doesn’t cover device and data costs, volume makes the loss bigger.
This driver includes cuffs, pulse oximeters, scales, glucometers, connec tivity, shipping, returns, losses, replacements, and platform subscriptions. The mature-year variable cost load still runs at 235% of revenue, so owner income depends on lowering unit cost, not just adding patients. Track costs per active patient, not just per device shipped.
Cut Unit Cost Fast
Measure this with device mix, cloud use, shipping rate, processing fees, and replacement rate. If one patient needs more replacements or support, margin falls fast because variable cost is tied to activity, not enrollment. The quick test is simple: compare monthly revenue per active patient to total device and platform costs per active patient.
Improve it by tightening onboarding, reducing returns, and matching the right device to the right patient need. Keep a clean log of shipments, failures, lost units, reorders, and subscription fees, then reprice or drop channels that don’t clear the variable cost load. If variable costs stay above revenue, there is no owner draw to protect.
- Track cost per active patient.
- Log returns and replacements.
- Review cloud cost per transmission.
5
Provider Acquisition And Retention
Provider Contracts and Retention
In remote patient monitoring (RPM), provider contracts drive patient flow and recurring revenue. With $850,000 in first-year marketing and $2,800 customer acquisition cost (CAC), the company can fund about 304 provider wins before collections mature, so weak retention hurts cash fast. If clinics slow referrals or churn, owner pay drops before fixed costs reset.
Track Payback and Churn
Measure each contract’s referral ramp, onboarding time, active patient count, and renewal risk. Payback depends on how fast a clinic turns into billable patients, not just signed accounts. Retention protects runway because every lost provider breaks future patient flow and pushes new CAC spend to replace it.
- Track referrals per clinic monthly.
- Watch churn and renewal dates.
- Measure onboarding-to-billing time.
Here’s the quick math: $850,000 ÷ $2,800 equals about 304 acquisitions. If referral consistency slips, the payback period stretches and owner income falls even if reported revenue still looks stable for a few weeks.
6
Compare low, base, and high RPM owner income cases
Scenario table
Owner income moves with active patient volume, collected PMPM revenue, and how fast payroll, marketing, device, and cloud costs are covered. The model starts cash negative, so pay timing matters.
| Scenario | Low CaseDownside case | Base CaseModeled case | High CaseUpside case |
|---|---|---|---|
| Launch model | Owner pay stays limited while active billable patients and collected PMPM revenue ramp slowly. | Owner pay is funded at the modeled salary level once breakeven lands in the opening months. | Owner pay can extend beyond salary into draws once higher patient volume and faster collections support stronger cash flow. |
| Typical setup | Collections trail plan, device and cloud costs stay heavy, marketing CAC is high, and fixed overhead plus payroll keep cash tight. | Active patients grow at the plan rate, collected PMPM improves, and the staffing model carries the listed payroll, marketing, and overhead loads. | Higher active patient counts, a better mix toward Pro Analytics and Enterprise Suite, and lower CAC lift gross margin and speed payback. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Deferred owner payCash tight | CEO salary onlyModeled pay | Salary plus drawsUpside pay |
| Best fit | Use this to stress-test the month 7 cash dip and delayed payback. | Use this as the main operating case for planning cash and owner compensation. | Use this to test the stronger case where owner income can rise after payback. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Remote Patient Monitoring Porter's Five Forces Analysis
- Remote Patient Monitoring BCG Matrix
- Remote Patient Monitoring Business Model Canvas
- 7 Critical KPIs for Remote Patient Monitoring Success
- Remote Patient Monitoring Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Remote Patient Monitoring Profitability
- Operating Budget: Analyzing Monthly Costs for Remote Patient Monitoring
- Remote Patient Monitoring Startup Costs: $650K CAPEX Plan
- Remote Patient Monitoring Financial Model Template in Excel
- How To Start A Remote Patient Monitoring Business In 90 To 180 Days
- How to Write a Remote Patient Monitoring Business Plan
- Remote Patient Monitoring Marketing Mix
- Remote Patient Monitoring Marketing Plan
- Remote Patient Monitoring Business Proposal
- Remote Patient Monitoring PESTEL Analysis
- Remote Patient Monitoring Pitch Deck Example Editable PPTX
- Remote Patient Monitoring Business SWOT Analysis
- Remote Patient Monitoring Value Proposition Canvas
Frequently Asked Questions
The model includes $200,000 in annual CEO pay, or about $16,667 per month before tax That is planned compensation, not guaranteed owner draw Real take-home depends on active billable patients, collections, reserves, and whether the business can cover about $237,000 in first-year monthly operating load