 Time to Open6-9 monthsSetup window
Time to Open6-9 monthsSetup windowHow To Open A Rheumatoid Arthritis Treatment Clinic In 6–9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6-9 monthsSetup window  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckPayer gateAuth and enrollment
Key BottleneckPayer gateAuth and enrollment First Revenue StepInitial consultsReferred patients
First Revenue StepInitial consultsReferred patients


To open a rheumatoid arthritis clinic, you typically need licensed providers, a legal entity, malpractice coverage, clinic space, a HIPAA-ready electronic health record, payer credentialing, lab and imaging relationships, specialty pharmacy or infusion workflows, trained staff, referral channels, and a launch-ready intake process A lean outpatient launch usually takes 6–9 months adding an infusion suite or major buildout can take longer In the researched planning case, Year 1 assumes 2 rheumatologists, 2 infusion nurses, 1 physical therapist, 1 occupational therapist, and 2 clinical assistants At Year 1 capacity assumptions, monthly service revenue models at about $193,150 before variable costs, so the launch plan must validate patient ramp, payer mix, and credentialing delays before go-live
Time to Open6-9 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckPayer gateAuth and enrollmentFirst Revenue StepInitial consultsReferred patientsLaunch timeline
Short web roadmap; the XLSX export holds the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8
Entity setup
- Form entity
- Open banking
- Tax registrations
- Draft policies
- Sign lease
Licensing and compliance
- License application
- Malpractice binder
- Payer enrollment
- Follow-up calls
- Compliance review
Site buildout
- Buildout plan
- Renovation work
- Refrigeration install
- Ultrasound install
- Infusion setup
EHR and billing
- EHR setup
- Prior auth rules
- Billing workflow
- Intake forms
- Claims testing
Staffing and training
- Recruit clinicians
- Hire assistants
- Credential staff
- Train workflows
- Mock visits
Referral and go-live
- Referral list
- Outreach calls
- Patient education
- Pilot scheduling
- Go-live review
Why test the rheumatoid arthritis clinic launch model before opening?
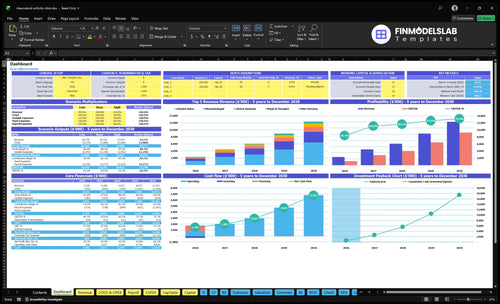
Open the Rheumatoid Arthritis Treatment Clinic Financial Model Template for revenue, costs, cash needs, assumptions, and break-even logic.
Financial model highlights
- Launch timing and ramp
- Provider capacity by role
- Patient volume by month
- Payer mix and runway
- Visits from $75 to $1,200
- Capacity: 65/50/60/55/70%
- Variable costs at 21%
- Delayed credentialing scenario stress
- Split visits from revenue
- Separate staffing from overhead
What mistakes delay a rheumatoid arthritis clinic launch?
For a Rheumatoid Arthritis Treatment Clinic, launch delays usually come from opening before credentialing is active, underestimating prior authorizations, and skipping a full test patient run. The other common breaks are weak referral flow, poor CBC/CMP tracking, and staff who do not know specialty workflows. If you add infusions, you also need nurse coverage, storage steps, and specialty medication coordination before day one.
Launch blockers
- Open only after credentialing is active.
- Map prior authorizations before first visit.
- Assign one owner for medication approvals and payer documentation.
- Build a steady referral pipeline.
Go-live checks
- Run one test patient end to end.
- Track CBC/CMP, imaging, and reminders.
- Train staff on specialty workflows.
- Hold infusion setup until nurse and storage are ready.
How long does payer credentialing take for a rheumatology clinic?
For a Rheumatoid Arthritis Treatment Clinic, payer credentialing usually fits inside a 6–9 month lean launch window, and it’s the gate that decides when you can book insurance-covered visits. Start with provider licensing, malpractice, CAQH profile updates, payer applications, contract review, electronic remittance setup, and effective-date confirmation. If that slips, first revenue slips too, even when the space and staff are ready.
Credentialing sequence
- 6–9 months for launch planning
- Licensing comes before billing
- Malpractice proof is required
- CAQH must be current
What slows opening
- Prior authorization workflows take time
- EHR setup can delay intake
- Specialty meds need coordination
- Effective dates must be confirmed
What do you need to open a rheumatoid arthritis clinic?
To open a Rheumatoid Arthritis Treatment Clinic, you need state medical licensing, a professional healthcare entity, malpractice coverage, payer enrollment, clinical protocols, and HIPAA-compliant operations before the first patient is scheduled; for the cost side, see What Are Operating Costs For Rheumatoid Arthritis Treatment Clinic?. The need is real: rheumatoid arthritis affects about 1.5 million US adults, and Year 1 staffing should cover 2 rheumatologists, 2 infusion nurses, 1 physical therapist, 1 occupational therapist, and 2 clinical assistants.
Must-Haves
- Active state medical licenses
- Professional healthcare entity setup
- Malpractice insurance in force
- Payer contracts and enrollment active
Launch-Ready Workflows
- DMARD monitoring and lab tracking
- E-prescribing and prior authorization ownership
- Imaging referrals and pharmacy coordination
- Scheduling, documentation, and referral intake live
Confirm the rheumatoid arthritis clinic is ready before seeing patients
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Licensing
- State license and entity activeCritical
No launch without state license, entity papers, and clear legal ownership.
- Malpractice policy boundCritical
Active malpractice coverage must start before any patient visit.
- Payer contracts effectiveCritical
Contract effective dates keep claims from getting denied at opening.
- Billing privileges confirmedHigh
Credentialing must be done so billing can start on day one.
Clinical flow
- EHR configured for rheumatologyCritical
EHR must support charting, orders, and audit trails for rheumatology.
- E-prescribing and prior auth testedCritical
Test e-prescribing and prior auth so meds do not stall.
- Intake and referral path liveHigh
Patients need one clear path from referral to booked visit.
- Billing and claims workflow testedHigh
Billing flow should post charges, claims, and payments cleanly.
Support services
- Core lab partners in placeCritical
Core labs must cover CBC, CMP, and inflammatory markers.
- Monitoring labs mapped to follow-upHigh
Follow-up labs keep biologic monitoring from slipping.
- Imaging referral path readyHigh
Imaging access keeps treatment decisions moving.
- Specialty pharmacy handoff documentedHigh
Pharmacy handoff is key for infusion or specialty drug starts.
Staffing
- Rheumatologists scheduledCritical
The Year 1 roster assumes 2 rheumatologists, so coverage must match.
- Infusion nurses scheduledCritical
Two infusion nurses are needed for planned infusion flow.
- Therapy coverage staffedHigh
PT and OT coverage support function and adherence.
- Intake and billing trainedHigh
Front desk and billing staff must know intake and claims steps.
Facility
- Buildout and renovation completeCritical
Buildout must finish before patient traffic begins.
- Infusion suite equippedCritical
Infusion suite equipment must support safe chairside care.
- Biologics refrigeration runningCritical
Cold storage must protect biologics and other meds.
- Ultrasound and PT gear installedHigh
Ultrasound and PT gear must work on day one.
Finance
- Cash runway covers setupCritical
Cash must cover the Month 2 dip to $846k minimum.
- Fixed overhead reconciledCritical
Overhead of $24,900 before wages has to be funded.
- First-month revenue model reviewedHigh
Year 1 volume should support about $193,150 monthly service revenue at planned use.
- Go-live signoff approvedCritical
Final signoff should confirm every launch gate is green.
Want the six launch drivers that control go-live?
1Provider Licensing
License gateNo reimbursable visits start until licensing, payer enrollment, and billing are active.
2Prior Auth Workflow
Auth gateClean prior authorization cuts biologic delays and keeps treatment plans moving.
3Clinic Space Flow
6-9 mo / $24.9KA tested intake-to-follow-up flow keeps the 6-9 month opening ramp from stalling.
4Specialty Staffing
2 R / 2 NYear 1 needs 2 rheumatologists and 2 infusion nurses to keep patient flow open.
5Lab and Pharmacy
Day-1 netPretested lab and pharmacy links prevent monitoring gaps and treatment delays.
6Referral Pipeline
$193K/moLive referral intake and held consult slots turn outreach into early revenue faster.
Provider Licensing And Credentialing
Provider Licensing And Credentialing
For an insurance-based RA clinic, active state licensure and payer credentialing are the gatekeepers to day-one revenue. You can have the space, staff, and schedule ready, but if the rheumatologist is not enrolled and effective dates are not live, payer-driven claims sit unpaid and opening slips into a cash delay.
The readiness signal is clear: license active, malpractice coverage in force, CAQH profile updated, payer applications submitted, contracts signed, and effective dates confirmed. Miss that chain, and you risk seeing patients before reimbursable status is active, which can delay first revenue even when the clinic is physically open.
Lock Credentialing Before Scheduling
Assign one owner to provider enrollment, billing setup, electronic remittance, and claim testing. Build the launch plan around the slowest payer, not the buildout, because one missing effective date can stall the whole revenue stream. No active credentialing means no clean first claims.
- Confirm payer effective dates in writing.
- Test claim routing before go-live.
- Verify remittance setup matches billing.
- Hold patient volume until reimbursement is live.
Before opening, check that the first billable visit date matches payer approval status. If the clinic sees patients too early, you create unpaid clinical work and a confusing start for patients who expect insurance to work on day one.
1
Prior Authorization And Treatment Approval Workflow
Prior Auth Workflow
Prior authorization, the payer approval step, has to be live before the first patient arrives. In rheumatoid arthritis, treatment often cannot start until the clinic can route requests, answer payer questions, and document why the drug is needed. If that flow is weak, care stalls, trust slips, and cash timing slows because approved treatment moves later.
The launch risk is simple: a clinic can look ready, but still fail on drug approvals. Day-one readiness means staff own payer policies, documentation standards, denials, appeals, and patient updates. Without that ownership, treatment plans sit in queues, handoffs get messy, and first visits turn into follow-up calls instead of starts.
Own the approval queue
Before opening, build the approval path inside the electronic health record (EHR) and assign one owner for each step: intake, medication history, lab proof, specialty pharmacy contact, denial review, appeal, and patient notice. Test the full route from visit note to submitted request so no patient leaves without a clear next step.
- Use EHR templates for payer notes.
- Capture medication history at intake.
- Attach lab results before submission.
- Track pending requests in one queue.
- Script patient updates for delays.
If the workflow is loose, biologic authorizations become the first bottleneck and the clinic opens with patients waiting, not starting treatment.
2
Clinical Space And RA Care Workflow
Clinic Space And Visit Flow
Space setup decides whether the clinic can open on time. A lean RA launch needs exam rooms, check-in, accessible patient flow, EHR workstations, phlebotomy or lab coordination, medication documentation, and referral handoffs. If the layout forces staff to backtrack between rooms, first-day visits slow down and the clinic looks busy before it is truly ready.
Infusion-ready space adds more risk. Once you add nurse workflow, storage, and patient monitoring space, the plan becomes more complex and needs tighter sequencing. The readiness test is simple: intake to exam to lab order to follow-up must work without staff improvising. One smooth visit flow matters more than a polished lobby.
Test The Full Patient Path
Walk the route before opening. Use one dry run for intake, rooming, documentation, lab order routing, and follow-up handoff. If any step depends on a missing workstation, unlabeled storage, or unclear phone handoff, fix that before go-live. The goal is not a finished buildout; it is a visit flow that works on day one.
Keep the first setup lean unless infusion is ready. A lean outpatient launch is easier to staff and easier to control. Infusion planning needs extra space, more monitoring, and tighter coordination, so delay that scope unless the people, equipment, and room flow are already locked. Clean setup now reduces bottlenecks during the early ramp-up.
- Confirm exam room count and flow
- Place EHR stations at point of care
- Test lab and referral handoffs
- Separate lean care from infusion needs
3
Specialty Staffing And Training
Specialty Staff Readiness
Headcount alone will not get a rheumatology clinic open on time. The Year 1 team needs 2 rheumatologists, 2 infusion nurses, 1 physical therapist, 1 occupational therapist, and 2 clinical assistants, plus lead, director, reception, and care coordination coverage. If those roles are filled but not trained on specialty workflows, first visits slow down and prior authorizations get stuck.
The launch risk is hiring general clinic staff who can room patients but do not know referrals, scheduling, prior authorizations, lab follow-up, billing handoffs, and patient reminders. That creates delays before the first billable care cycle and can leave patients waiting on medication approval instead of starting treatment.
Train the handoffs before day one
Before opening, assign one owner for each step: intake, referral chase, authorization tracking, lab results, and billing handoff. The readiness signal is simple: staff can explain the full path from referral to follow-up without guessing. If they cannot, the clinic will open with gaps that show up on day one.
Test the workflow with real scenarios, not just job titles. A good launch plan proves that reception can route requests, clinical assistants can flag missing records, and care coordination can keep reminders moving. That reduces dropped authorizations and helps the first patient visits happen faster.
- Map every handoff before scheduling starts.
- Train on specialty meds, not general intake.
- Test prior auth and lab follow-up.
- Confirm billing handoffs before first claims.
4
Lab, Imaging, And Specialty Pharmacy Network
Lab and Pharmacy Network Setup
Rheumatoid arthritis clinic day-one care depends on a live lab and specialty pharmacy network. The clinic needs CBC and CMP monitoring, inflammatory marker workflows, imaging referrals, medical supplies, billing clearinghouse links, and electronic health record integrations. If any handoff is late, patients wait for results or fills, and the clinic opens with delays instead of safe, same-day care.
Year 1 cost assumptions also matter: 45% medical consumables and lab supplies and 85% specialty biologic drug inventory. That makes vendor terms, reorder timing, and stock control part of launch readiness, not back-office cleanup.
Test the Order-to-Result Loop
Before go-live, test the full path: place an order, route it to the lab or imaging partner, receive the result, confirm the referral, and close the staff follow-up task. The readiness signal is clear: orders move, results track, referrals confirm, and the team knows who calls the patient.
- Confirm lab turn times.
- Map imaging referral owners.
- Verify pharmacy shipment steps.
- Test EHR and clearinghouse links.
- Assign follow-up coverage before opening.
5
Referral Pipeline And First-Patient Scheduling
Referral Intake and First-Patient Booking
Referral marketing is a launch readiness system, not a last-minute ad push. If the clinic cannot turn referrals into scheduled visits, opening on time does not matter much. For a rheumatoid arthritis clinic, the launch risk sits in the handoff from primary care, orthopedics, pain specialists, hospitals, insurance directories, local search, condition pages, and pre-opening outreach into booked initial consultations.
The readiness signal is operational, not cosmetic: referral intake live, records request process tested, consult slots held, and waitlist patients confirmed. Year 1 patient marketing and digital ads are modeled at 5% of revenue, so this funnel has to work before day one if you want a faster revenue ramp.
Test the Booking Path Before Go-Live
Set up who receives each referral, who requests records, and who schedules the consult. The goal is one clean path from referral to first visit, with no dropped names and no dead time between intake and slot assignment.
- Confirm source-specific intake rules.
- Test records requests end to end.
- Hold consult slots before opening.
- Confirm a waitlist of ready patients.
If the team cannot answer a referral in one step, the pipeline is not launch-ready. That gap slows first revenue and leaves exam rooms idle while the clinic is technically open.
6
Related Products
- Rheumatoid Arthritis Treatment Clinic Porter's Five Forces Analysis
- Rheumatoid Arthritis Treatment Clinic BCG Matrix
- Rheumatoid Arthritis Treatment Clinic Business Model Canvas
- What Are The Five KPI Metrics For Rheumatoid Arthritis Treatment Clinic?
- Rheumatoid Arthritis Treatment Clinic Business Plan Template in Pre-Written Word
- How Increase Profits Rheumatoid Arthritis Treatment Clinic?
- What Are Operating Costs For Rheumatoid Arthritis Treatment Clinic?
- Rheumatoid Arthritis Clinic Startup Costs: $305K CAPEX Plan
- Rheumatoid Arthritis Clinic Financial Model Template in Excel
- How Much Can A Rheumatoid Arthritis Clinic Owner Make With $232M Revenue?
- How To Write A Business Plan For Rheumatoid Arthritis Treatment Clinic?
- Rheumatoid Arthritis Treatment Clinic Marketing Mix
- Rheumatoid Arthritis Treatment Clinic Marketing Plan
- Rheumatoid Arthritis Treatment Clinic Business Proposal
- Rheumatoid Arthritis Treatment Clinic PESTEL Analysis
- Rheumatoid Arthritis Clinic Pitch Deck Example Editable PPTX
- Rheumatoid Arthritis Treatment Clinic Business SWOT Analysis
- Rheumatoid Arthritis Treatment Clinic Value Proposition Canvas
Frequently Asked Questions
Yes, a licensed rheumatologist can open a private clinic if state medical rules, entity structure, malpractice coverage, payer enrollment, and clinical operations are set up correctly For this planning case, the Year 1 model starts with 2 rheumatologists and 2 infusion nurses The bigger issue is not eligibility it’s whether payer contracts and specialty workflows are ready before visits begin